
Abstract
The purpose of this study was to determine the extent to which grit influences the quality of life (QOL) in patients diagnosed with multiple sclerosis (MS). Mixed-methods included a survey (n = 51) via Qualtrics utilizing the Grit Scale, Short Form-36 (SF-36), and general demographic questions and phenomenological interviews (n = 14). Quantitative data were analyzed using the SPSS25. Qualitative data were analyzed using whole-parts-whole analysis. The average grit score for participants diagnosed with MS was 3.8 ± 0.5. Moderate correlations existed between grit scores and emotional role limitations (r = .542, P < .001), emotional well-being (r = .542, P < .001), and social functioning (r = .448, P < .001). Common themes that emerged from the phase II interviews included (a) an initial shock or relief factor, (b) an identity shift, and (c) advocacy and victories. Higher levels of grit correlate with a better QOL.
Introduction
Angela Duckworth, the originator of the Grit Scale, defines grit as the passion and perseverance for long-term goals (1–3). Researchers have suggested that grit positively correlates with the quality of life (QOL) across multiple populations (4–8). QOL is a broad term that encompasses overall general health, wellness, and satisfaction in daily activities (9). It also refers to outlook and positivity about an individual's current and future states. QOL is typically measured by surveys or scales, which assign quantitative values to these different domains (9). When an individual is diagnosed with a chronic, progressive disease, like multiple sclerosis (MS), an array of emotions can be evoked which can be best examined by qualitative approaches that attend to lived experience.
MS is a chronic, inflammatory disease that is driven by an autoimmune reaction against the myelin sheaths and/or oligodendrocytes of the central nervous system (9, 10). There are 4 primary types of MS that range in severity of signs and symptoms. These signs and symptoms experienced from MS influence a patient's perception of QOL post-diagnosis. Health is one of the key determinants of QOL. The World Health Organization defined health as, “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” (10). Because health is a difficult concept to standardize, the Short Form-36 (SF-36) questionnaire is often used to obtain qualitative measures of self-perceived health and QOL in 8 domains across multiple populations (7,11,12).
The SF-36 consists of 8 scored domains exploring different aspects of overall health, including the physical, emotional, social, and mental factors to determine the perceived QOL of an individual. Those diagnosed with MS are influenced in all areas of their lives and the SF-36 can assess the extent of that influence. The data obtained from the SF-36 can then be correlated to individuals” grit scores to establish a relationship between the two.
Several studies suggest positive health outcomes are correlated with positive perspectives and grit (7,8,13). One study indicated positive associations between academic grit and academic achievement, life satisfaction, and school satisfaction (13). Another study suggests that physical fitness and health behaviors that constitute physical health QOL could also relate positively to grit (7). Grittiness is a powerful tool for improving one's QOL. Because grit has been found to be an acquired trait, it could potentially be used to enhance rehabilitation outcomes for patients. The purpose of this study was to investigate how grit influences one's life after a diagnosis of MS.
Materials and Methods
A mixed-methods approach was used in this study. The IRB at the University of North Georgia granted exempt approval. Participants were recruited via a convenience sample through survey invitation links sent to MS support groups throughout the United States. Part I of the study involved a survey administered via QualtricsTM which included questions on basic demographics, the 12-item Grit Scale, and items from the SF-36 questionnaire. Informed consent was obtained by a brief statement about the study and potential participants were offered an opportunity to contact the primary investigator and ask questions. Clicking on the start button implied consent. After completing the survey, participants were invited to participate in an optional phenomenological interview for Phase II of the study. Informed consent was provided by obtaining a signed consent form. Participants were allowed to ask questions. These interviews provided a thick, rich description of the lived experience of being diagnosed with MS. Transcripts from the interviews were shared with each participant to ensure that the transcription was a credible and trustworthy representation of the interview. A vertical analysis of each interview provided a deeper understanding of each participant's lived experience and provided initial themes for analysis. A horizontal analysis explored common themes across all interviews to develop a common description of the lived experience of receiving a diagnosis of MS.
After the common description was created, it was shared with participants via email in a resonance round for confirmation that the description indeed represented the lived experience of individuals diagnosed with MS. Resonance rounds serve to build credibility and trustworthiness that the common description created represented the lived experience of individuals diagnosed with MS. Resonance rounds were also conducted with nonparticipants who did not complete the survey or interview but who were familiar with MS to build further credibility and trustworthiness of the common description.
Quantitative Results
There were 51 individuals (12 males, 39 females) who completed the survey in Phase I of the study. The mean age for participants diagnosed with MS was 51.8 ± 13.8 years. Mean years living with MS was 16.5 years ± 11.4 years. The mean grit scores for both male and female participants diagnosed with MS was 3.8 ± 0.5 (Table 1). Fourteen participants completed the Phase II interviews (6 males, 8 females) and 1 identified as African American and the others as European American.
Participant Descriptive Data.

Abbreviations: MS, multiple sclerosis; SF-36, Short Form-36.
Significant correlations between grit scores and subscales of the SF-36 existed. There were moderate correlations between grit scores and emotional role limits (r = .542, P < .001), emotional well-being (r = .542, P < .001), emotional role functioning (r = .476, P < .001), and social functioning (r = .448, P < .001). Cronbach's alpha for the SF-36 was .954 and .752 for the Grit Scale. There were also correlations between years lived with MS and emotional role limits (r = .301, P < .05), energy fatigue (r = .329, p < .05), emotional well-being (r = .356, P < .05), and social functioning (r = .297, P < .05) (Table 2).
Correlation Tables for Grit and SF-36 Constructs.
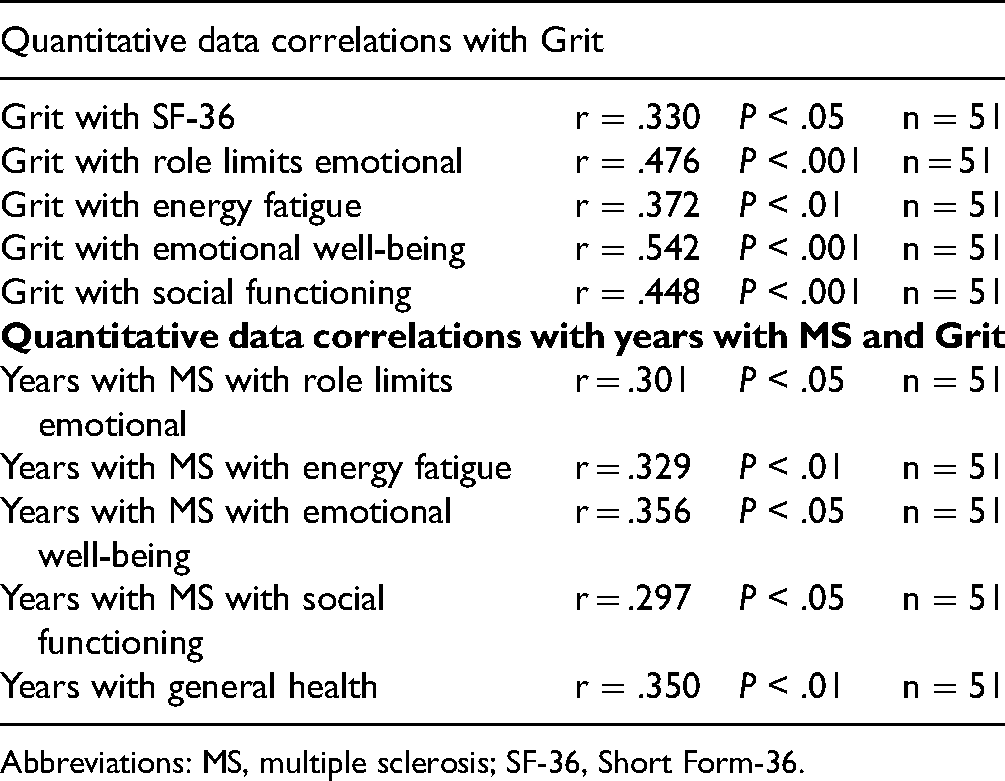
Abbreviations: MS, multiple sclerosis; SF-36, Short Form-36.
Qualitative Results
Table 3 presents common themes that emerged from the phenomenological interviews.
Common Themes With Exemplars.

The first theme was the shock or relief factor experienced at the initial diagnosis. Some participants, like Turkey, described the initial diagnosis to be depressing which led to a mourning process. She states:
I went into a depression state but did not know why I was depressed. The feeling was like somebody had died… and for the life of me I couldn’t figure out who died. But I had that feeling like when a close relative or somebody died… It finally dawned on me. YOU HAVE DIED! Yeah. I was mourning myself.
Karen described the anticipation she felt with the uncertainty of her diagnosis stating: It's kind of like waiting for the other shoe to drop… waiting for something to progress because I do feel it as a disease.
The second theme identified was an identity shift where participants described the crucial time after diagnosis as an evolution of self. John Wayne stated, “The other thing you have to do is that you have to reinvent yourself.” This evolution is often fostered by one's support group. Nancy advised others with MS stating, “Reach out to an MS group. It will help you as you go through the identity shift.”
Support quality was a recurring sub-theme that came with the identity shift. Power was felt with the right support. Some participants felt they did not benefit from traditional MS support groups. Others, like Frank, ended up much more involved with his support group than he initially expected: And I went to my first MS support group meeting and met some people there and heard their stories. Long story short on that, I now run that support group there. You have to stay resilient… You don’t know what tomorrow will bring. But let's not worry about tomorrow. Let's deal with today right now.
Jean added to the statement saying, “I have MS. It does not have me!”
In terms of going with the flow, Nancy stated: There is so much plasticity in the brain. Don’t be a cement block. Be more like a river and let the water flow. Have an open mind.
The third and final theme that came through in the phenomenological interviews was entitled advocacy and victories. Daily battles are common to those diagnosed with MS, especially in regard to the health care system and insurance companies. Advocacy was crucial. One respondent during resonance rounds stated: It's a full-time job . . . fighting doctors, pharmacies, people's attitudes towards you . . . and on and on. Eleven years after getting MS, I still have to fight the medical system. I took on city hall and created 9 handicap accessible parking spaces in our town. My legal advocacy paid off.
Advocacy for and by patients with MS elicit victories on multiple levels. For some, getting out of bed is a victory in itself. For others, like Grace, it's the personal victories that keep her going. She shared, “I set a goal and accomplish it. I set another goal and accomplish it. It builds my self-esteem.”
Most participants suggested optimism is key to reaching goals and experiencing everyday victories. When faced with a diagnosis like MS, one response may be a can-do attitude. Samm shared her response to her doctor's diagnosis: The doctor told me I had MS. He said, “Congrats, you have MS officially.” And the very first words out of my mouth were, “Bring it on.” And that is exactly how I have lived it. Just bring it on.
Participants with MS believed that it is important to keep life to it fullest. Nancy articulated in her interview, “I have so much more of my life left and I am ready for it!”
The common description across interviews was developed. Resonance rounds with participants clarified points and built credibility and trustworthiness from the emic perspective. Further resonance rounds were conducted with nonparticipants who had not been involved in the study but who were familiar with MS. These rounds enhanced the credibility and trustworthiness of the description from the etic perspective (Table 4).
Resonance Round Feedback on Common Description.

Abbreviation: MS, multiple sclerosis.
The common description discusses the lived experience as: Receiving a diagnosis of Multiple Sclerosis involves a shock factor. It may provide a sense of relief and may even confirm some of our suspicions. We once questioned our symptoms, but with the validation of an official diagnosis, we finally know we aren’t crazy. We may feel a bit of depression and have to mourn our previous self. We have been busy, successful individuals. Once we accept the diagnosis, we wait for the other shoe to drop. Nevertheless, an identity shift must occur. In reinventing ourselves, we learn leadership skills and face challenges in the physical, emotional, and social realms. We remind ourselves that MS does not have us; we have MS. Just because we have MS, does not mean we are MS. As life goes on, we learn to go with the flow. Optimism helps us move forward like the flow of a river. The right support is powerful. This power allows us to survive little battles and achieve victories. Battles with the system will always exist and our victories may include battles won through advocacy, or simply the optimism to get through each day on a personal level. Advocacy may also allow us to orchestrate community-based successes to educate others and dismantle barriers. MS is a snowflake disease. Each person will experience MS and its progression differently.
Discussion
Participants in this study had high levels of grit based on their grit score. Many shared stories of gritty adaptation after their diagnosis of MS. The mean grit score of the participants with MS was 3.8 ± 0.5. According to the research done by Duckworth (1,2) and others (3,6,7,14,15) grit correlates with strong passion and perseverance to achieve goals despite obstacles and adversity, or in this case, a diagnosis. High grit scores can also be seen in populations diagnosed with other neuropathologies, including Parkinson's disease and stroke (14,15). Individuals with MS had higher grit scores (3.8 ± 0.5) than individuals with Parkinson's (3.65 ± 0.5), and survivors of stroke (3.77 ± 0.5). Researchers of this study speculate that although stroke, Parkinson's, and MS are all neurological diagnoses, the grit values are not that different. Consequently, individuals with neurological impairments such as MS, stroke, and Parkinson's score high in grit as they learn to adapt to participation in new life roles. The rehab recovery process may be the reason individuals with neurological impairments have a high level of grit (8,10,12,14,15). Levels of grit have also been explored in wheelchair basketball players (8). In this study, participants who had higher levels of grit were the most involved in their sport. Higher levels of resilience, hardiness, and QOL were also found. If rehabilitation is viewed as a gritty activity, then grittier individuals who are more engaged in their rehab activities are more likely to also have higher QOL and be more successful at achieving their goals. Assessing grit among individuals with MS may provide insight into perceived QOL.
QOL is often a measure of how a person is coping after a diagnosis. The SF-36 measures 8 subscales (physical function, role limits for physical health, emotional role limits, energy/fatigue, emotional well-being, social functioning, pain, and general health) that are believed to collectively reflect one's general health and are directly related to QOL (16,18). When a person possesses a high level of grit, the high passion and perseverance to overcome challenges may contribute to the overall SF-36 score and several subscales measured by the SF-36.
Time lived with MS may deteriorate grit scores and QOL. A weak correlation existed between years with MS and emotional role limits (r = .301, P < .05). We hypothesize that over time, individuals with MS may lose grit as their physical function deteriorates; however, there are many factors such as support systems and personal optimism that may be protective of the grit and QOL. The weak correlation between grit scores and energy fatigue (r = .329, P < .05) may be explained by the limiting physical effects of MS on a person despite possessing a high grit score. Although a person may be motivated and willing to have a productive day, their body may not tolerate it. MS often limits activity levels due to physical fatigue (10, 12).
A moderate correlation existed between grit scores and emotional role limits (r = .542, P < .001), emotional well-being (r = .542, P < .001), and social functioning (r = .448, P < .001). Participants with higher levels of grit are able to participate in life roles more successfully without interference from emotional problems. Those with higher levels of grit also possessed a greater emotional well-being fostered by the drive to face everyday challenges and overcome them. Social function was also affected by grit levels. Grittier participants were more driven to discover and learn about their diagnosis by seeking meaningful experience and social connections, often in the form of social groups.
A diagnosis of MS and subsequent life journey can bring about many emotions and reactions as described by the participants. Three main themes emerged from the collective interviews from Part II of the study. The first theme was an initial shock or relief factor following the initial diagnosis of MS. Participants articulated feelings of depression, mourning, and uncertainty described as waiting for the other shoe to drop. After the initial diagnosis, participants described undergoing an identity shift requiring personal evolution through advocacy. Many individuals did reinvent themselves, and go with the flow in order to cope and adapt to their new journey with MS. Many participants started support groups and advocated for structural changes in their city. Although support groups were not appropriate for all of the participants, the power of support, whether through family and/or friends, played an important role in the evolution of their new self.
Despite the social and emotional challenges of living with MS, participants continued to face an array of battles and victories in their life. Because MS affects everyone differently, participants described it as a snowflake disease. No 2 people with MS experience it in the same manner. Whether the battles are fought on a personal level, such as getting out of bed, or on a community level, such as fighting for more handicap parking spots, all victories are significant. Grit appears to be correlated with successful functioning once diagnosed with MS.
Strengths and Limitations
Strengths of this study included the Grit Scale and SF-36 tool which possess strong psychometrics. The Grit Scale had a Cronbach’s α of 0.752 indicating an adequate construct validity. The Cronbach’s α for the SF-36 was 0.954 indicating an excellent construct validity. Survey and interview results were derived from a wide variety of responses across the United States. Saturation for Phase II interviews was achieved by 13 of the 14 interviews of the study. Common themes and a common description were developed from the data describing lived experiences of individuals diagnosed with MS. Member checking with participants ensured that each transcript represented each participant's story. Resonance rounds with participants and nonparticipants provided credibility and trustworthiness of the themes and common description.
Several limitations exist in this study. The diagnosis of MS may vary and consequently may affect an individual's QOL differently depending on the type of MS and support system a person may have. Results of this study may not apply to everyone with MS. The SF-36 was chosen as a tool to measure QOL because it had been used both by neurologists and individuals diagnosed with MS in previous studies (12,14). Because the SF-36 is lengthy, it may be difficult for those with severe MS to respond to the survey via the computer. The Grit Scale used in this study asked participants to recall details and events that occurred previously in their life. Participants may not accurately recall details related to their diagnosis of MS. Most participants in this study, however, responded that they will never forget the day they received the MS diagnosis. Finally, resonance rounds confirmed the common description of receiving a diagnosis of MS adding trustworthiness and credibility to that description by seeking perspectives of those who participated in the study and those with MS who did not participate in the study.
QOL is often a measure of how a person is coping after a diagnosis of MS. The SF-36 measures certain subsets that relate to one's overall QOL (17,18). The Grit Scale measures an individual’s resilience and perseverance to overcome and achieve goals despite obstacles such as a long-term progressive neurological diagnosis (1,2). Those with MS who demonstrate higher levels of grit are more likely to have a higher QOL. The participants in this study who scored higher on the grit scale exhibited higher scores in the physical function, emotional well-being, and general health subscales of the SF-36. If grit is a personality trait that can be learned, physical rehabilitation may be a mechanism to foster grit as individuals reenter life with a diagnosis of MS. Physical therapists play a role in enhancing QOL for patients as movement specialists who improve QOL and optimize function through prescribed exercises, hands-on care, and patient education (8,14,15,18,19). Engagement in the rehabilitation process may foster the development of grit and improve perceptions of QOL by helping the client focus on improved function or adaptations for function. Furthermore, facilitating grit in patients during rehabilitation may contribute to the social-emotional coping skills needed to reenter and redefine full participation in life roles.
Footnotes
Acknowledgments
The authors would like to acknowledge all the participants and caregivers who participated in this study and shared their stories with us.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Review Board (IRB) at the University of North Georgia approved this study for human subjects as an exempt approval #2020-106.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.