
Abstract
Nurses experience high levels of stress as they deal with the patients having complex health care problems. Stress in nursing affects the practice of nursing profession worldwide. In response to this, the investigators explored the sources of work-related stress (WRS) among Omani Nurses. Samples were selected through proportionate population sampling from 5 selected tertiary care hospitals. Data were collected through self-administered nursing stress scale (NSS). The study included 383 Omani nurses. Descriptive and inferential statistics were used to analyze the data. The sources of WRS among nurses showed the percentage mean scores ranging from 8.5% to 21%. The overall mean score for the NSS was 42.85 ± 17.705. Out of 7 subscales, the highest level of WRS was on workload with a mean score of 8.99 (21%) followed by emotional issues related to death and dying 8.72 (20.4%). The lowest mean score was seen on the lack of support 3.65 (8.5%) and inadequate preparation to meet the emotional demands of patients and their families 3.86 (9%) of the total mean. WRS was associated with the nursing position as staff nurses, performing night shift and reduced job satisfaction. The study's results may help in developing human resource strategies aimed at minimizing nurses’ stress and improving quality of health care and task force performance.
Introduction
Nurses encompass the largest workforce and play an important role in the provision of direct patient care. 1 Additionally, nurses play a significant intermediary role between the patient and the physician. 2 In addition to providing direct patient care and dealing with the human suffering daily, nurses are expected to meet multiple and conflicting demands imposed by nurse managers, supervisors, medical and other administrative staff in the hospital. These lead the nurses to experience stress, role conflict and workload, which seriously impairs the efficacy of delivery of quality healthcare service. 3
Over the past decade, nurses have regularly been reported to experience highest job stress regardless of their specialty. 4 Earlier studies indicate that work-related stress (WRS) is particularly prominent among nurses. 5 WRS is the physical and emotional reactions that occur due to encounters between a nurse and their work environment when job demand exceeds the nurse's expertise and resources. 6 As nurses play a critical and most extensive role in providing holistic patient care and deal with the patients having acute and chronic illness with disability and discomfort from birth to death, there is no surprise that nursing has been unfailingly known globally as stressful work. 7
Considerable (9.20%-68.0%) percentage of nurses worldwide suffer from stress; in particular, 20% to 40% of nurses suffer from WRS. 8 Irrespective of countries they work, nurses experience WRS across the world. In nurses from 41 hospitals in Shanghai, China, 74.8% of nurses suffer from WRS. 9 Almost three-quarter of nurses in Australia reported “extremely high” or “quite high” level of stress. 10 In India, 87.6% of nurse's experience stress, with 2.1% reporting severe stress. 11 In Dubai, 95% of nurses experienced varying degrees of stress and 86% of them were less than 36 years. 12 While in Oman, no studies have reported about the WRS among nurses.
WRS can be caused due to physical, social, and psychological sources either related to the environment or workplace. Firstly, the physical stressors are associated with complexity of highly interactive medical technology. In addition, due to understaffing and escalating healthcare costs, the number of nurses available has decreased which increases their workload. Secondly, nurses’ psychological sources of WRS are related to higher demands for nursing care by patients and families. 13 The social sources of nurses’ WRS include lack of good relationships with peers, superiors, and colleagues, resulting in low productivity and low risk solving interests. 14
In Sultanate of Oman, nurses account for the highest proportion in the healthcare sector and they serve in a variety of settings. With a growing population and ongoing healthcare needs, nursing sector suffer from a shortage. 15 Additionally, nurses in Oman experience 10% of work load pressure and spent 9% and 33% variation in the proportion of time in support activities. 16 Moreover, due to Omanization, non-Omani nurses started leaving the country, leaving the Omani healthcare system difficult in finding replacement. Therefore, Omani nurses encounter increased workload, which may negatively affect the healthcare quality. 17 Moreover, nurses working especially in Omani tertiary care hospitals face more challenges due to overcrowding. Furthermore, nurses in Oman feel that staffing shortages, heavy workloads, lack of job choice, and difficulty meeting family obligations negatively influence their professional lives. In some hospitals, nurses have no formalized job descriptions and are assigned tasks that have nothing to do with nursing, such as dispensing medication after midnight in the pharmacy and performing online statistical reports. 18
In the personal experience, the principal investigator noticed that the shift schedules for most of the nurses are determined by factors like demand and location, rather than by personal preference. Moreover, the nursing schedule for each ward is typically developed by the ward's charge nurse and is in accordance with the hospital policy. Omani nurses often work 8- or 12-h shifts, spreading their full-time schedule over 5 days. Because of the shift work required by nurses, they often miss important family and religious celebrations. This is believed to increase the WRS among Omani nurses.
Although a great deal of research has been done on stress among nurses internationally, to the best of our knowledge, no research has been done and published about WRS among nurses in Oman. Given that the international hospital settings and the provision of health services are different than those in Oman, it would not be appropriate to use the results of previous international studies to explain the WRS among Omani nurses. Therefore, the authors explored the source of WRS among Omani nurses.
Materials and Methods
Study Design
This study used a descriptive cross-sectional design.
Setting
The study was conducted in Sultan Qaboos University Hospital (SQUH), Royal hospital (RH), Armed Forces hospital (AFH), Khoula hospital (KH), and Al-Nadha Hospital, Muscat, Sultanate of Oman. All these 5 hospitals were tertiary care public hospitals extending health care services to people from various governorates of Oman. The number of Omani nurses working in SQUH were 490, AFH (484), RH (787), KH (486), and Al-Nadha hospital (258), respectively.
Sample Size
The sample size for this study was estimated using the preceding sample size formula as 383. n = (nf * N in a health facility)/N total, where n = number of potential participants in a given public hospital, nf = final sample size obtained using the Cochrane formula. N = the total number of potential participants in the government tertiary hospitals (2505). Therefore, the proportion for SQUH was calculated as; n = (nf * N in a health facilities)/N total n = (490*380)/2505, making n = 75; RH had 787 nurses, contributed to 120 nurses; KH had 486 nurses, contributed to 74 nurses; Al-Nahdha hospital had 258 nurses, contributed to 39 nurses; and lastly AFH had 484 nurses, contributed to 75 nurses. The total sample size for this study was therefore 383 nurses.
Sampling Method
Samples were selected through proportionate population sampling from the selected 5 hospitals. Thereafter, a random number table was used to select the required number of participants from each setting.
Sample Characteristics
Omani registered nurses, working in tertiary governmental hospitals in Muscat City, with at least 1 year of clinical nursing experience, and who were able to speak, write, and read English language were included. If the nurses were suffering from psychological problems like depression, and anxiety-related diseases, and the nurses who were working in COVID-19 departments during the time of data collection or 1 month before data collection were excluded. Additionally, nurses having less than 1 year of experience were excluded as they were considered to be on probation as per the Ministry of Health policy. During this period, they complete the orientation to the unit and formal training program in the hospital. The inclusion and exclusion criteria were mentioned in the first page of the Google form, which allowed the nurses to decide whether they are eligible to participate in answering the Google form.
Instruments Used for Data Collection
A self-administered questionnaire was used in data gathering. The questionnaire had 2 sections, namely, demographic/job-related nurses’ profile and nursing stress scale (NSS).
Demographic/job-related nurses’ profile
This part consisted of 11 questions that tapped information regarding participants’ gender, age, marital status, education level, working institution, working department, working years of experience, nursing position, working in night shift and job satisfaction and thought of changing profession.
Nursing stress scale
NSS was designed to measure the frequency and sources of WRS experienced by nurses. Graft-Toft and Anderson developed this instrument in 1981. 19 This tool is publicly available for use by the researchers. It consisted of 34 items. The type of response ranged from “0” indicating “Never” to “3” showing “Very frequently” according to their perceived occurrence of stress in the workplace. The NSS identified 7 major sources of WRS including death & dying, conflict with doctors, inadequate preparation to deal with the emotional needs of patients and their families, lack of support, conflict with other nurses and supervisors’, and workload and uncertainty concerning treatment.
The NSS comprised of 34 items and the overall level of job-related stress can be calculated by summing all the items. The minimum score is 0 and maximum is 102. The higher score indicates higher level of stress. The scale also contains 7 subscales with percentage mean scores ranging from 8.5% to 21%. The overall mean score for the NSS is 42.85 ± 17.705. The mean score was used to categorize the level of WRS among nurses. Nurses are identified to have low stress if the mean score is less than the overall mean score and high stress if the mean score is equal or greater than the overall mean score. The questionnaire was pilot tested and had a Cronbach's alpha of 0.85.
Ethical Considerations
Ethical approval was sought from the Medical Research Ethics Committee (MREC) of Sultan Qaboos University (SQU-EC/263/2020 dated 08/11/2020), Ministry of Health (MOH/CSR/20/23891 dated 13/10/2020) and Armed Forces Hospital, Sultanate of Oman (AFMS-MREC 024/2020 dated 10/11/2020). The investigators provided sufficient information to the nurses about the purpose of the study and were given the privilege of clarifying their doubts. After assuring the confidentiality, implied consent was obtained. All the study participants were encouraged to participate in the study and were also told that they have the right not to participate. The collected data was stored in a password-protected computer and only the investigators had the access to the data.
Data Collection
Data were collected from October 15, 2020 to November 30, 2020. Data were collected using a Google form prepared by the investigators of the study. Data were transferred to Statistical Package for the Social Sciences (SPSS) version 25.
Data Analysis
Data analysis was conducted using SPSS software program version 25. Categorical sample characteristics were summarized using number and percentages, whereas continuous sample variables were summarized using mean and standard deviation. The association between sample demographic characteristics and the WRS was analyzed using the Chi-square. Independent samples t-test and 1-way analysis of variance were also used to determine the mean difference in the WRS variables across categories of the demographic variables. All statistical tests were 2-tailed and the significance level was set at 0.05.
Results
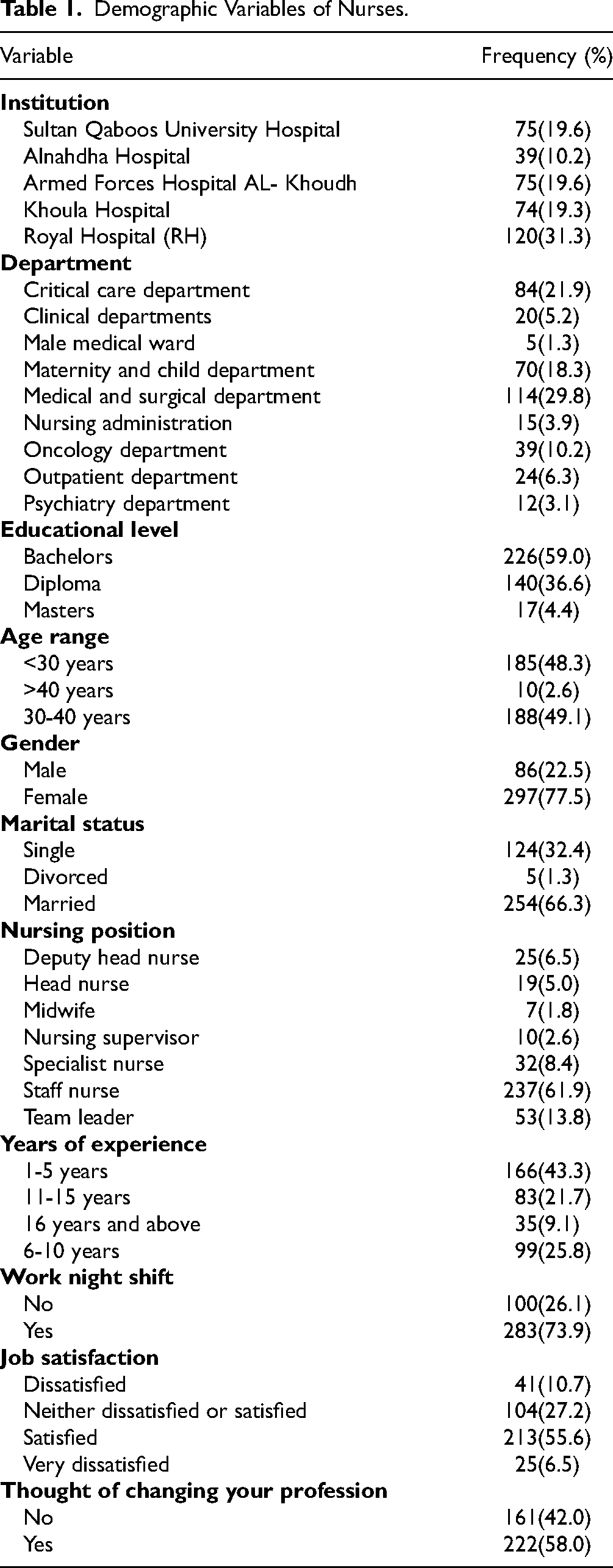
In our study, 383 subjects participated. Most of the nurses were working at RH (31.3%); majority were from the Medical and Surgical Department (29.8%); most nurses had 1 to 5 years of work experience (43.3%); majority had a bachelor's degree in nursing (59.0%); were aged between 30 and 40 (49.1%); 77.5% were females; 66.3% were married; 61.9% were staff nurses; 73.9% worked in night shifts; 58.0% thought of changing profession, and 55.6% were satisfied with their job (Table 1).
Demographic Variables of Nurses.
The sources of WRS among nurses showed the percentage mean scores ranging from 8.5% to 21%. The overall mean score for the NSS was 42.85 ± 17.705. Out of 7 subscales, the highest level of WRS was on workload with a mean score of 8.99 (21%) followed by emotional issues related to death and dying 8.72 (20.4%). The lowest mean score was seen on the lack of support 3.65 (8.5%) and inadequate preparation to meet the emotional demands of patients and their families 3.86 (9%) of the total mean.
On the individual items per subscale I related to death and dying, the most stressful condition was watching a patient suffering (1.75 ± 0.941) followed by performing procedures that patients experience as painful (1.56 ± 0.854) and feeling helpless in case of a patient who fails to improve (1.31 ± 0.867). The least stressful source of stress was physician not being present when a patient die (0.89 ± 0.966).
On conflict with physician's subscale II, the least stressful events were conflict with a physician (1.14 ± 0.902) and disagreement concerning the treatment of a patient (1.15 ± 0.828). However, making a decision concerning a patient when a physician is unavailable was the most stressful event in the subscale-II (1.29 ± 0.904).
Feeling inadequately prepared to help with the emotional needs of a patient (1.23 ± 0.906) was the least stressful event in subscale III; inadequate preparation to meet the emotional demands of the patients and their families is the most stressful event in the subscale III (1.32 ± 0.931) (Table 2).
Items on Conflict With Physicians, Inadequate Preparation to Meet the Emotional Demands of Patients and Their Families and Lack of Support Subscales Respectively (n = 383).

0 = Never, 1 = Occasionally, 2 = Frequently, 3 = Very frequently.
In the sub-scale IV lack of support, the least stressful event is lack of opportunity to express to other personnel in the unit about the negative feelings toward patients (1.17 ± 0.867). However, the lack of opportunity to talk openly with other unit personnel about problems in the unit was the most stressful event in subscale IV (1.28 ± 0.916) (Table 2).
Similarly, on conflict with other nurse's/supervisors’ subscale V, the most stressful condition was asked to relieve other units that are short-staffed (1.27 ± 0.902) followed by criticism by a supervisor (1.13 ± 0.921) (Table 3).
Items on Conflict With Other Nurses/Supervisors, Workload and Uncertainty Concerning Treatment Subscales Respectively (n = 383).
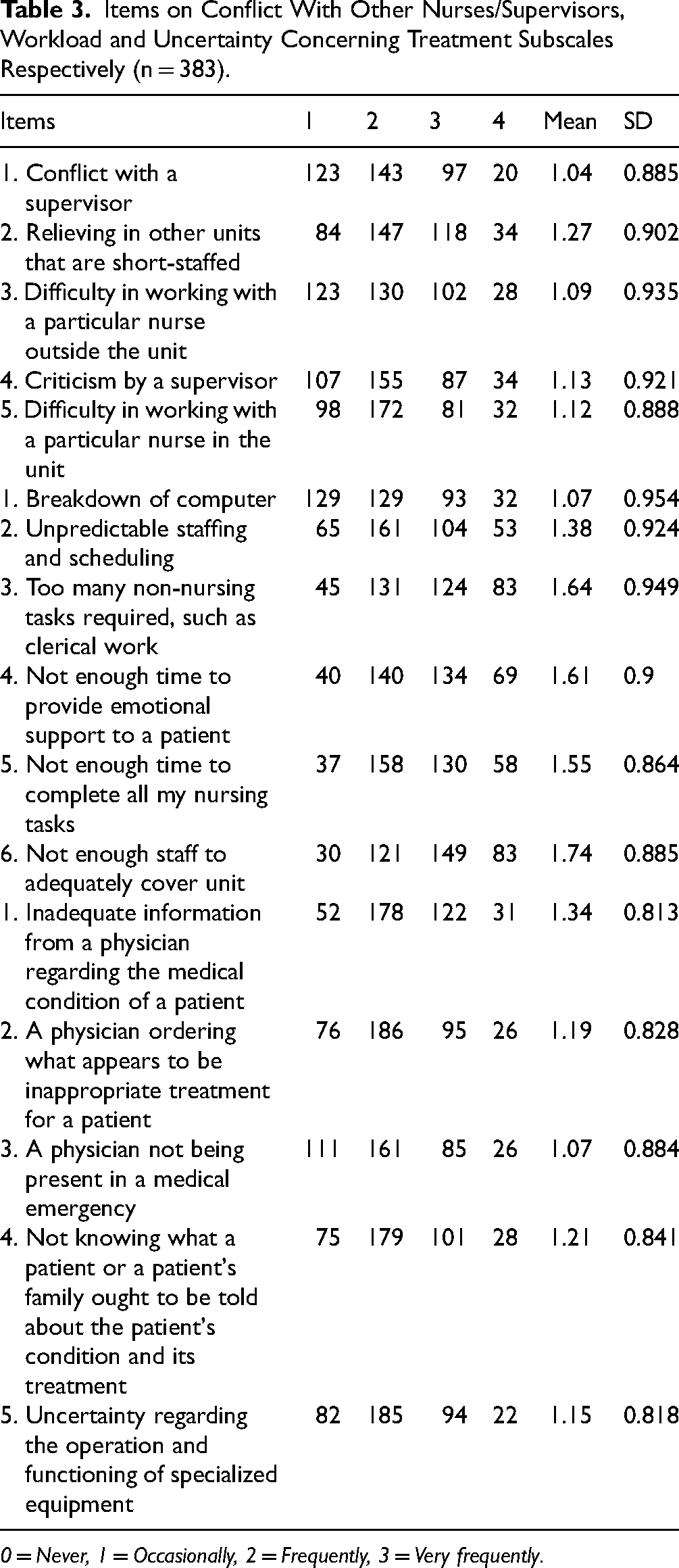
0 = Never, 1 = Occasionally, 2 = Frequently, 3 = Very frequently.
Not having enough staff to adequately cover unit (1.74 ± 0.885) was the most stressful event in the workload subscale VI followed by the item too many non-nursing tasks required, such as clerical work (1.64 ± 0.949). Finally, inadequate information from a physician regarding the medical condition of a patient (1.34 ± 0.813) was the most stressful situation in the uncertainty concerning treatment subscales VII (Table 3).
Furthermore, Chi-square analysis was done to determine the association between demographic variables and WRS. The analysis showed that nursing position was significantly associated with work stress (X2 = 18.297, P = .004) using Fisher's exact test. In addition, working in the night shift was significantly associated with work stress (X2 = 14.933, P < .001). Furthermore, job satisfaction was significantly associated with work stress (X2 = 8.752, P = .033). The frequency analysis revealed that those dissatisfied with their job are more highly stressed compared to those who are satisfied (Table 4).
Association Between Socio-Demographic Variables and Work-Related Stress Among Nurses.

*Significant at P = .05.
**Fishers exact test used.
Discussion
Owing to the taxing nature of the nursing profession, confronting inappropriate communication in the workplace, stressful work environment, and lack of sufficient competency of the individual or colleagues in performing some tasks, nurses feel stressed out with their work on a daily basis. Moreover, nurses continually face patients who are physically and mentally in critical conditions and go through the huge pressure of job responsibilities besides personal obligations. 20
WRS in the context of work involves stress related to work organization, career development, and interpersonal relationships while content of work stress include risk factors arising from the work environment and equipment, division of tasks and planning, hours of work and workload. 21 In our study, it is obvious that workload was the cause for highest level of WRS. This finding corroborated with a study that showed that major stressors are experienced with excessive workload. 22 Furthermore, in a study conducted in Jimma Zone, South West Ethiopia, workload was significantly higher in public health hospital. 6 Another study conducted in 2 specialist hospital in the city of southwest Nigeria 23 and an Italian healthcare company 24 showed that workload was a major source of stress.
In our study, we found 2 reasons for increased workload. Firstly, there was not enough staff to adequately cover the unit; secondly, too many non-nursing tasks required, such as clerical work. Similarly, Faremi et al 23 identified too many non-nursing tasks such as clerical work, inadequate staff to cover ward workload, lack of drugs and equipment required for nursing care, and unpredictable staffing and scheduling, as the frequently reported stressful events. Likewise, administrative issues reported were shortage in nursing workforce, inadequate support from nursing supervisors, low salary, and high levels of expectations. 25 Nurses are working more than ever before due to increased demand for nurses, an insufficient supply of nurses, reduced staffing, increased overtime and patient length of stay. 26
Firstly, the demand for nurses is growing as the population ages, and Oman is undergoing an age-structural transformation towards a greater proportion of older adults (65+). Secondly, the number of nurses are insufficient to satisfy the existing demand. The shortage is expected to worsen when potential demand rises and nursing schools are unable to keep up with the demand for the adequate number of graduate nurses. Thirdly, because of the global economic crisis, Oman tends to reduce the supply of money and work force to health care services. As a result, hospitals cut nursing personnel and mandated overtime to satisfy unusually high demand, dramatically increasing nursing workloads. 27 Consequently, nurses now provide care for sicker patients than in the past, and would need a more intensive workload. 14 Therefore, strategies should be designed to minimize the workload of nurses.
In our study, “watching a patient suffering” was the most stressful condition. Additionally, the nurses reported, “performing procedures that the patients experience as painful” and “feeling helpless in case of a patient who fails to improve” as stressful events. This can be explained by the fact that multiple aspects of death anxiety contribute to individuals’ anxiety and stress which affect a person's well-being psychologically, physically, and socially. 28 The most common feelings described by nurses in other studies were feelings of inadequacy, incompetence, followed by self-blame as the result of a patient's death. 29 In addition, nurses may not have enough time to support one another's emotions in general, and those related to death and dying in particular, because of their increased workload. 30
In our study, nurses reported that making a decision concerning a patient when a physician is unavailable as the most stressful event. However, no consistent literature is found to support our study findings. Therefore, we recommend further studies to investigate the availability of a physician while making a patient decision as a predictor for stress among nurses. In general, conflict with physicians is a key cause of stress in nursing which can be managed through integrating, dominance, obliging, avoidance, and compromise. 31 Therefore, nurses and physicians should understand their roles and work collaboratively.
The most stressful event found in our study is “Inadequate preparation to meet the emotional demands of the patients and their families.” Likewise, another study stated that it is stressful when collectivist beliefs predominate among the patients’ and their families’ 32 which is difficult to handle. On the contrary, a study conducted among nurses in Hungary, Israel, Italy, United Kingdom, and the United States found that the contact with patients and their families was not a cause of stress among nurses of United States. 33 It may be related to the fact that American nurses are trained to cope with social interactions on the job. Additionally, since the United States is the most individualistic country of the 5 nations, families probably have less influence over individuals’ medical treatment. Therefore, further studies are required to confirm these contradictory study findings.
The lack of opportunity to talk openly with other unit personnel about problems in the unit was the most stressful event in our study. In general, job satisfaction is related to the environment in which the nurse works. The presence of support from colleagues and supervisors is a significant predictor of job satisfaction and it is a major factor responsible for reducing stress. In addition, organizational support is highly essential for the nurses. 34 Therefore, support from colleagues, supervisors, and organization is very much needed to reduce the stress among nurses.
Similarly, being asked to relieve other units short-staffed was most stressful. We could not find any supportive literature to support this finding. We recommend studies to explore on this finding. Furthermore, criticism by a supervisor was a stressful factor. Conflict among nurses has been a critical problem in health care settings, which is due to variations in management styles, employee perceptions, personnel shortages, and goal variations and competition among work groups. When the conflict between the nurse supervisor and the nurse is serious and persistent, it might result in unsatisfactory patient care. 35 Therefore, it is critical that the nurse supervisors resolve and manage conflict effectively.
Finally, inadequate information from a physician regarding the medical condition of a patient was the most stressful situation in our study. In line with our study findings, another study showed that 49% of nurses had reported the frequent occurrence of stress, 30% experienced occasional occurrence of stress, and 21% had extreme stress due to uncertainty concerning treatment. 36 These findings alarm us that the communication between nurses and physicians should be improved to enhance the treatment process, thus the quality of patient care.
In our study, working in the night shift was significantly associated with WRS. Nursing shift work results in highly pressurized work performance and risk for limited job performance, which might also lead to several health issues in nurses. 37 Nurses in our study had different shift rotation depending on each hospital regulations and policies. For instance, nurses working in SQUH had 2 shifts, that is, 12 h per shift. The rest of the nurses in other tertiary hospitals works 3 shifts, that is, 8 h per shift. The frequency of shift changes in these hospitals occurs due to daily movements, weekly rotations, or urgent rotations. This could be the reason for the stress among nurses. In consistent with our study results, several studies showed that the nurses working on rotating shifts and night shifts were more likely to experience stress and burnout than those working on fixed shifts.38–42 Therefore, allowing workers the flexibility of work time will help in reducing stress in employees. 43
Furthermore, our study showed that nursing position was significantly associated with WRS. In our study, deputy head nurses, head nurses, midwifes, nursing supervisors, specialist nurses, staff nurses, and team leaders participated. However, more number of staff nurses participated in our study. Consistently, Khaleel et al 44 informed that the newly employed nurses undergo WRS than the senior nurses, as the new nurses perform too many responsibilities in their duty while the senior nurses perform official and documentary work which is less stressful. However, Ojekou & Dorothy 45 and Al-Aameri 46 reported inconsistent findings with the previous 2 study findings. These studies reported that the nurses in the higher positions experience higher levels of stress as they were accountable for more number of subordinates and supervise administrative responsibilities. Therefore, more studies are to be conducted to confirm these conflicting study findings. In addition, higher positions in nursing and its relationship with WRS shall be studied.
Besides, job satisfaction was significantly associated with WRS. Those dissatisfied with their job are highly stressed compared to those who are satisfied. To substantiate our study findings, Dagget et al, 6 and others47–50 found job satisfaction as a predictor for WRS among nurses. However, Gulavani 36 has reported dissimilar findings whereas job satisfaction was not related to occupational stress. Henceforth, future studies should be done to confirm these different findings.
Finally, among Omani nurses, we observed no correlation between WRS and demographic factors including department, education, age, gender, marital status, or years of employment. This calls for further studies to explore the relationship of these variables with WRS.
Limitations
As we utilized self-reported stress questionnaires, the nurses might have provided subjective measures representing individuals’ perceptions. This might have affected the validity of our study findings. In addition, this study was limited to Omani nurses only. As our study was a cross-sectional study and provided only a snapshot within the study period, longitudinal research can be done to examine whether there is an evidence of WRS changes over time. WRS could have been reported higher during the COVID-19 period, calling for further studies to see the differences in WRS during the non-COVID-19 period. Moreover, since the study's context was tertiary care public hospitals in Muscat city, it would be useful replicating this study in other hospitals including primary, secondary, urban, rural, and private hospitals of the Sultanate of Oman, which might give different results. In addition, this study was limited to Omani nurses only. Therefore, further research is needed to include nurses who are different nationalities, which would give a broader view of the working conditions regardless of nationality.
Conclusion
Omani nurses working in tertiary care hospitals suffer from high levels of workload, which is related to severe shortage in number of nursing staffs and performing non-specified responsibilities. Nursing position, night shift duties, and job satisfaction were statistically significantly associated with WRS.
Recommendations
Since workload was identified as the primary source of WRS, organizational strategies should be attempted to reduce the workload. These interventions could involve recruiting additional registered nurses, which is an obvious way to reduce workload; increasing appointing nurse aids to perform bed linen change, temperature and blood pressure taking; and employing clerical staff to reduce non-nursing activities. We understand that hiring new nurses is not an easy choice in the present economic crisis of the country; however, Omani Ministry of Health shall plan different strategies to minimize the WRS among nurses. Additionally, nursing administrators in all hospitals shall provide a supportive work environment for nurses. In addition, counselling services should be made available for the nurses when they face stressful events. Nurse managers may help nurses cope with stress by establishing effective 2-way communication systems, clarifying role and performance expectations, resolving conflicts practically, developing policies that minimize the stress associated with shift work, establishing support groups for nursing personnel, making psychological counselling accessible and available to the affected nurses, and enhancing observational skills to detect increased stress and burnout levels among nurses. Finally, more studies are needed to understand stress, burnout, depression, and other psychological issues experienced by Omani nurses.
Footnotes
Acknowledgement
We would like to express our deep gratitude to all the nurses who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval was sought from the Medical Research Ethics Committee (MREC) of Sultan Qaboos University (SQU-EC/263/2020 dated 08/11/2020), Ministry of Health (MOH/CSR/20/23891 dated 13/10/2020), and Armed Forces Hospital, Sultanate of Oman (AFMS-MREC 024/2020 dated 10/11/2020). The investigators provided sufficient information to the nurses about the purpose of the study and were given the privilege of clarifying their doubts. After assuring the confidentiality, implied consent was obtained. All the study participants were encouraged to participate in the study and were also told that they have the right not to participate. The collected data was stored in a password-protected computer and only the investigators had the access to the data.