
Abstract
Background
A multidisciplinary team of health scientists and educators at an academic medical center came together to consider the various factors that impact well-being among self-identified women working in healthcare and conducted a comprehensive literature review to identify the existing body of knowledge.
Objectives
To examine how well-being is defined, what instruments are used to measure it, and correlation between professional and personal gender-specific factors that impact the well-being of women in healthcare occupations.
Methods
A total of 71 studies published in 26 countries between 1979-2022 were extracted from PubMed. Studies enrolled adult women (18-74 y.o.) healthcare professionals including nurses, physicians, clinical social workers, and mental health providers. Well-being related phenomena such as quality of life (QOL), stress, burnout, resiliency, and wellness were investigated. In this review, women are broadly defined to include any individual who primarily identifies as a woman regardless of their sex assigned at birth.
Results
The results of our analysis were consistent across the scope of the literature and indicated that women in healthcare occupations endure a significantly higher level of stress and burnout compared to their male counterparts. The following gender-specific factors were identified as having direct correlation to well-being: job satisfaction, psychological health, and work-life integration.
Conclusions
The findings from this review indicate a need for evidence-based integrative interventions across healthcare enterprises to combat stress and burnout and strengthen the resiliency and well-being of women in healthcare. Using information from this review, our team will launch a comprehensive well-being assessment and a series of interventions to support resiliency and well-being at our academic medical center.
Keywords
Introduction
Women have driven 80% of the overall growth in the booming healthcare field since the turn of the century. 1 The number of full-time, year-round workers in healthcare occupations almost doubled since 2000, increasing from 5 million to 9 million according to the US Census Bureau, where women currently account for 3 quarters of this number. 1 The global increase of women working in healthcare has raised concerns regarding their well-being. 1 Due to the varying roles that women play in society, they are more prone to experiencing mental health issues brought on by immense pressure and stress to succeed both at home and at work simultaneously. This issue can affect their physical and mental health to the point of causing psychological distress, occupational burnout, depression, anxiety, rapid turnover, or suicidal thoughts. 2 For example, a 2018 study revealed that 60% of female physicians experienced burnout compared to 40% of male physicians. 3 Similar circumstances appear in the literature as early as graduate studies.4-6 The magnitude of this issue leads to decreased work performance, lower quality care, and a loss of patient trust and adherence to treatment protocols.3,7,8 Further, this issue negatively affects employee productivity, healthcare system costs, and turnover rates—each associated with a sizeable cost burden. 3 As the number of women entering the healthcare profession continues to rise, concerns about the health of women are becoming more prevalent, and it is critical that they receive adequate support.
The George Washington University (GW) School of Medicine and Health Sciences (SMHS) Resiliency & Well-being Center (R&WC) was recently founded to support whole person health, which is grounded in purpose–one’s reason for being or existing. The R&WC serves the GW medical enterprise and strives to strengthen resilience (elastic adaptation) and well-being (health and wellness) of SMHS faculty, staff, and medical trainees. To effectively serve our community, we must prepare for program assessment by measuring the well-being of our community members at baseline. The R&WC utilizes a version of the Center for Disease Control and Prevention (CDC) definition of well-being: an integration of mental health (mind) with physical health (body) resulting in a more complete approach to disease prevention and health promotion that also takes into consideration high life satisfaction, a sense of meaning or purpose, and the ability to manage stress.
With women’s well-being as a priority for the R&WC, we begin our investigation by determining methods and strategies grounded in empirical research and evidence for assessing well-being in women healthcare professionals by way of this comprehensive, scoping review. In our evaluation of existing instruments, we aim to assess if they reflect the above definition of well-being and comprehensively assess both physical and mental components of it including threats to well-being.
The findings of this review will inform the metrics we use to measure well-being at the GW medical enterprise. Therefore, this review aims to identify the primary factors that determine the well-being of women in healthcare professions, determine the most effective, evidence-based metrics of well-being in this population, and inform the design of a well-being instrument to be used annually in the GW medical enterprise.
Methods
This review followed the five-stage process of developing a scoping review as outlined by Arksey and O’Malley:
9
(1) Identifying the Research Question (2) Identifying Inclusion/Exclusion Criteria (language, target population, study design, outcomes) (3) Identifying Relevant Studies (4) Study Selection (5) Charting the Data (6) Collecting, Summarizing, and Reporting the Data
The protocol for this review was previously published as a preprint in PsyArXiv. 10
Identifying the Research Question
With the primary objectives of this review in mind, our research team, which includes a nutrition scientist, health sciences researchers, psychotherapist, librarian, and a physician assistant, designed specific research questions: (1) How do women in healthcare define/understand well-being? (2) What instruments are used to measure well-being among healthcare workers? (3) What gender specific factors that emerge from biological differences, societal norms, and cultural expectations related to masculinity, femininity, or other gender identities impact an individual’s sense of well-being?
Identification of Relevant Studies and Search Terms
A systematic search of the literature was conducted with the help of a GW reference librarian, who assisted in developing the search strategy for PubMed. Our choice of PubMed was determined by its public accessibility, focus on biomedical and life sciences literature, and reliability based on peer reviewed sources.
PubMed Search Terms.

Study Selection: Inclusion/Exclusion Criteria
From our search we identified 103 studies from 26 countries (e.g., US, Canada, China, and Japan) published between 1979 (the earliest article that returned from our literature search) and 2022. Those studies were imported into Covidence systematic review software (Veritas Health Innovation; Melbourne, Australia) for screening of their titles and abstracts to determine relevance to our research question. At this stage, 3 members of the research team voted on the inclusion of each article. To move forward into full-text analysis, articles had to have at least 2 votes for inclusion. At this stage, a total of 24 studies were excluded for various reasons including being publishes in any language other than English, Russian, Ukrainian, or Polish, or for considering a topic unrelated to the well-being of women in healthcare. We then assessed the full-text of the remaining 79 manuscripts and further excluded 8 studies that did not consider women healthcare professionals (n=4), were not peer-reviewed academic articles (n=2), and did not contain full-text in our languages of review (n=2). A total of 71 studies were included in this comprehensive review (Figure 1). Literature review search and screening process.
Charting the Data: Data Extraction from Full-Text Review
In our review of the literature, we searched for well-being as a broad phenomenon and discovered data on related concepts such as job satisfaction, burnout, stress, resiliency, psychological health, quality of life, and work-life integration. We systematized results based on how the above factors impacted the well-being of women healthcare workers. The outcome measure instruments that were used to assess well-being ranged widely depending on the angle from which each source viewed this phenomenon.
Reviewing the Quality of Literature
Some studies that we investigated were conducted using evidence-based instruments to measure well-being, including Maslach Burnout Inventory (MBI),10-27 Copenhagen Burnout Inventory (CBI),28-31 Short-Form Health Survey (SF 36 V-2),7,31,32 Minnesota Satisfaction Questionnaire (MSQ),10,33,34 Effort-Reward Imbalance Questionnaire (ERI).16,25 Of note, the World Health Organization (WHO) 5 Well-being Index (WHO-5) was only used once 35 but was the most concise well-being instrument among those used in the literature. Further, being designed by the WHO lends credibility to the metric. However, there were several other sources that used various non-validated self-developed outcome measurement tools, including qualitative instruments.36-55 Most studies used cross-sectional study design as well as descriptive correlational methods.
Maslach Burnout Inventory (MBI)
Is a measurement of an individual experience of an occupational burnout in 3 dimensions: emotional exhaustion, depersonalization and personal accomplishment. 56 MBI is used for assessing professional burnout in human services, education, medical personnel, students, and the general population. It assesses and validates the three-dimensional structure of burnout and helps to understand the nature of burnout for developing effective interventions. While burnout may be a symptom of poor well-being and even correlate with well-being, it is not a direct measure of well-being itself.
Copenhagen Burnout Inventory (CBI)
Is an instrument for burnout measurement that consists of 3 scales measuring personal burnout, work-related burnout, and client-related burnout. CBI scales are found to differentiate well between occupational groups in the human service sector and correlate with measures of fatigue and psychological well-being. The scales also predict future absence, sleep problems, use of painkillers, and intention to quit. 57 Again, this is not a direct measure of well-being.
Short-Form Health Survey (SF 36 V-2)
Is a 36 item scale designed to survey health status and quality of life based on self-reporting. The SF-36 includes 1 multi-item scale that assesses 8 health concepts: (1) limitations in physical activities because of health problems; (2) limitations in social activities because of physical or emotional problems; (3) limitations in usual role activities because of physical health problems; (4) bodily pain; (5) general mental health (psychological distress and well-being); (6) limitations in usual role activities because of emotional problems; (7) vitality (energy and fatigue); and (8) general health perceptions. 58 It has excellent psychometrics and produces 2 summary scores: the mental health component and the physical health component. This is a direct measure of well-being.
Minnesota Satisfaction Questionnaire (MSQ)
Is a 5-point Likert-type scale with 20 items that measures how vocational needs and values are satisfied on the job. It is a well-known and validated instrument that has been stable over time. 59 It comes in 2 long forms and 1 short form. It is useful when an organization wants to measure the overall level of satisfaction with the job rather than how important specific aspects of the job are to the employee. 60 While job satisfaction is an important contributor to well-being, this is just one of many and thus not a direct measure of well-being as a whole.
Effort-Reward Imbalance Questionnaire (ERI)
Is a measurement of workplace satisfaction related to specific functional demands (the effort element of the instrument) and the professional recognition and rewards (the rewards element of the instrument) and how these are interrelated and impact professional well-being. 61 The tool is useful is measuring imbalance between challenge and reward and can capture information related to individual coping strategies, the management of stress, feelings of job security and adequacy, and how professional life can impact personal identity. The ERI is a more holistic measure of job satisfaction and its contribution to well-being, making it an important element in well-being. However, it is not a direct measure of well-being in its entirety.
World Health Organization 5 Well-being Index (WHO-5)
Is a measurement of overall well-being limited to a very specific timeframe–the assessment only measures well-being across a period of 2 weeks and is highly context dependent. 62 The WHO-5 was initially developed in 1982 as a 28-item instrument to measure well-being and, over time, has been refined and redesigned to ask only 5 questions: 4 related to positive impacts on well-being and 1 related to negative impacts on well-being. Importantly, multiple studies have confirmed clinical and psychometric validity for this tool, which is a direct measure of well-being.
Collecting, Summarizing, and Reporting the Data
Ultimately, the 71 articles included in the full-text review were imported into Dedoose for thematic analysis as described in detail below.
Thematic Review
Our research team followed an inductive coding process wherein we did not enter the review with a preexisting code book. Rather, we took time to familiarize ourselves with the manuscripts through an initial full-text review of the 71 articles, developed a data extraction form to capture relevant characteristics of each manuscript (e.g., country of study, professions examined, outcomes measures utilized, salient findings), and then conducted an initial coding process where we carefully reviewed the data extracted from each manuscript to identify the phenomenon of study, the instruments used to measure outcomes, and the findings, recommendations, and limitations to each manuscript. From here, we began to quantify code appearance and cooccurrence to identify emergent themes from across the literature. This allowed us to group literature together by theme and make comparisons of reported outcomes across countries of publication and professions under study.
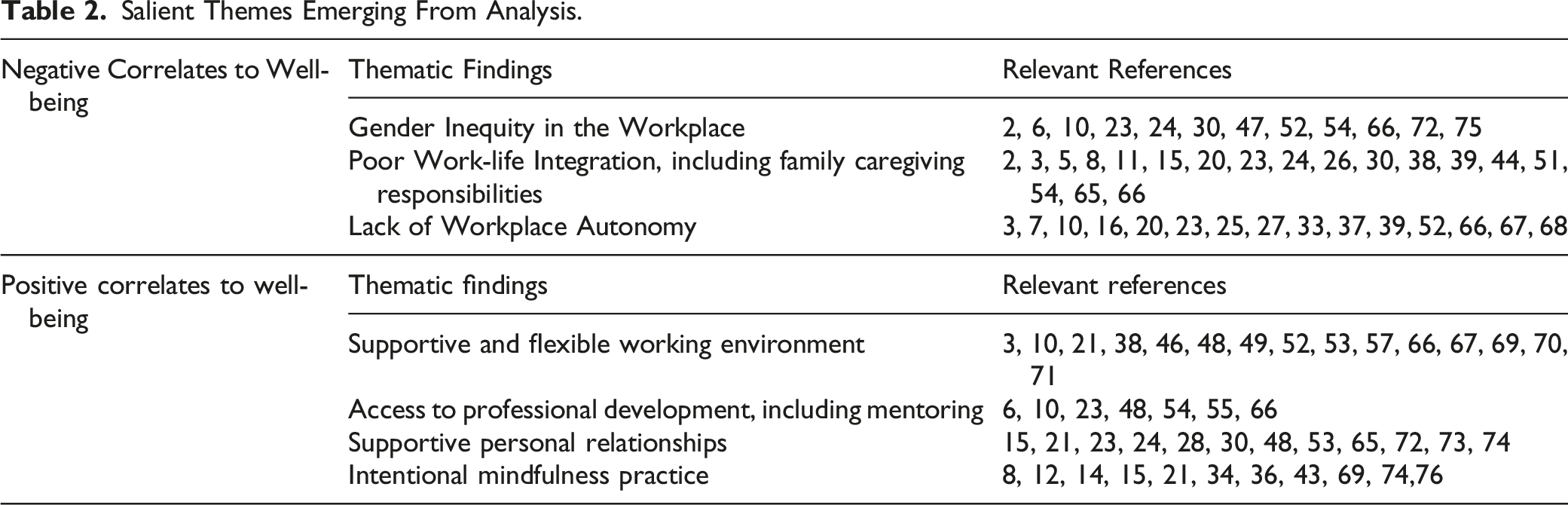
Salient Themes Emerging From Analysis.
Results
Measurements of Well-Being in the Literature
Based on the findings of this review, instruments were used to measure the absence of well-being (e.g., burnout) rather than the presence of well-being itself. Many of the studies in this review only conducted disease-centered evaluations reflecting an area in research that has room to grow (See Reviewing the Quality of Literature Section). Just 10% (n=12) of the assessment tools used in this review seek to quantify individual characteristics such as hope, optimism, resiliency, self-acceptance, self-esteem, or the impact of the lived experience like positive work-life integration, personal and professional growth, meaningful social support, religiousness/spirituality, or having a sense of purpose. Given this, to further bring clarity to the definition of well-being, our study will require a substantially greater utilization and dependence on assessment tools that are anchored in a complete approach to holistic well-being and not solely isolating pathology such as the Cassidy Social Support Scale, Chinese Psychological Capital Questionnaire, or Connor-Davidson Resilience Scale, ERI, MBI, or Perceived Stress Scale-10 (PSS-10).
Work-Life Integration
Among the articles reviewed, the negative relationship between poor work-life integration and a general sense of well-being appeared in approximately a quarter of all studies. 8,11,15,20,24,26,38,44,51,65,66 Studies cite how women are encouraged to prioritize the needs of their children and families over their own personal and professional development, often to their own detriment.2,8,30,39 In the context of our research question, our review found an emphasis on the dissatisfaction women feel when they are required to leave their careers to provide care to their family, even when they are the higher income earner in their families.2,3,5,23,54
Professional Autonomy
Almost 25% of the articles in this review suggest deficient working conditions and limited professional autonomy contribute to women experiencing burnout at greater rates than their male colleagues.16,20,25,27,37,39,52,67,68 Studies indicate that women feel powerless,10,39,52 more constricted by time pressures, 3 have higher workloads,7,33 and expend more emotional energy on psychosocially complex patients than their male colleagues. 3 These articles acknowledged deep professional conflict women have, as they tend to be the compassionate, empathic listeners in an environment that values speed.3,23,66
Supportive Work Environments
In 22% of included articles, the propensity of general satisfaction and a reduction of burnout in the workplace was linked to a supportive environment and flexible schedules, which accommodate childcare and other contributors to well-being.21,46,53,69 In the context of this review, a supportive work environment included those that provided professional recognition,10,66 offered flexibility in terms of scheduling,3,38,70 provided vacation leave, 53 and extended additional training for those interested.3,10,45,48,49,52,57,67,71 The literature also reveals the positive impact of an atmosphere of camaraderie in the workplace. 15
Personal Relationships
Across the literature, 21% of the studies in this review emphasized the importance that personal relationships inside and outside of the workplace have on well-being.21,23,30,48,65,72 The community of friendships,15,28,73 romantic,53,74 and familial relationships24,53,65 provides an essential element of emotional support that positively influences the experiences of women employed in healthcare. These studies show the central phenomenon of well-being ultimately involving the individual’s lived-experience and the impact of environmental influence like social support to relieve stressors.
Implicit Gender Bias
In this comprehensive review, 16% of the articles cited instances of implicit gender bias in the workplace as a significant cause of mental distress among women in healthcare.6,23,24,30,52,54,66,75 This inequity appeared in various forms, from unequal pay for equal work,2,47,52,72,75 to a refusal to acknowledge women clinicians by their titles (i.e., referring to women physicians by their first names but using the Doctor honorific for their male colleagues), 2 and fewer opportunities for professional advancement for women despite similar qualifications to men.6,10,30,54,72,75 Importantly, these inequities were cited widely across the literature regardless of year of publication or country of study, suggesting that this phenomenon remains a persistent if not universal issue.
Intentional Mindfulness
Just 15% of the studies we collected focused on the positive relationship between well-being and intentional mindfulness (n=4),21,36,43,69 nutrition and exercise (n=4),8,12,14,15 and restorative sleep (n=3).34,74,76 These studies add to the growing body of knowledge that lifestyle interventions can reduce compassion fatigue, stress, and burnout with yoga, prayer, meditation, a balanced diet (non-specific), and quality sleep. The correlation between active coping mechanisms and stress management in the literature engenders discussions for future well-being research and the specific challenges of women in healthcare. At our center, this will be a key component of our interventions.77-83
Professional Development Opportunities
Opportunities to pursue professional development and mentoring made a positive difference in 11% of the articles included in this review. Mentoring relationships and professional development allow for a greater sense of belonging,48,54,55,66 a deeper connection to their supervisor, 48 fulfillment in professional opportunities,48,66 and more job satisfaction.6,10,23,54,55 This awareness highlights the fundamental importance of self-actualization in the workplace.
Discussion
This is the first comprehensive review, to our knowledge, to examine multiple study designs related to the well-being of women working in the healthcare profession across various countries and social contexts. Most studies describe well-being as the absence of a disease state and/or absence of adverse effects due to low reward or dissatisfaction in the workplace. However, utilizing just the former definition is not truly indicative of well-being, as well-being goes beyond lack of disease and includes the promotion of security, comfort, and happiness. Therefore, a clear, widely accepted definition will be necessary to implement a standardized approach to well-being research. It is our recommendation that the definition from the CDC be utilized, “a positive outcome that is meaningful for people and for many sectors of society, because it tells us that people perceive that their lives are going well,” be adopted by the research community as part of harmonization efforts. 63 We have adapted the CDC’s language to craft the following definition for the GW R&WC:
Well-being integrates mental health (mind) with physical health (body) resulting in a more complete approach to disease prevention and health promotion that also takes into consideration high life satisfaction, a sense of meaning or purpose, and the ability to manage stress. Tracking these conditions is important for public policy. Yet, many indicators that measure living conditions fail to measure what people think and feel about their lives, fundamental states such as the quality of their relationships, their positive emotions and resilience, the realization of their potential, or their overall satisfaction with life—their “well-being.” 64
Multiple overlapping themes in connection with the absence of well-being in women healthcare professionals emerged throughout this literature review. Despite the significance of the analysis examined, the limited longitudinal data, self-reported questionnaires, and homogeneity of smaller participant groups in some studies could arguably weaken their overall strength and generalizability. This literature review analyzes the key gender-specific factors impacting an individual’s sense of well-being.
Therefore, future reviews considering well-being utilizing a whole-body framework are merited. We suggest examining neurological, psychological, and musculoskeletal outcomes of a supportive work environment, opportunities for professional mentoring, positive personal relationships, and attention to whole body health (e.g., mindfulness, nutrition, exercise, sleep) in relation to valid and reliable measures for disease prevention, health promotion, life satisfaction, a sense of meaning or purpose, and the ability to manage stress.
Conclusion
This review provides a comprehensive overview of studies conducted across 26 countries within the last 4 decades, which explored the well-being of women healthcare professionals and examined the correlation between complex work-related stressors and well-being. The included literature has revealed several important factors contributing to a higher prevalence of job dissatisfaction, emotional turmoil, and a lack of work-life integration, which has devastating effects on healthcare professionals and the quality of patient care. Based on the findings of this review, our future study will examine the impact of positive wellness culture and well-being in a larger construct in relation to women in healthcare professions.
This literature review can inform further investigation of different levels of gender-sensitive interventions, not only on individual but also on organizational level, and their effectiveness. They could take into account the broader context and structural determinants of gender inequality and look into increasing awareness and training on gender sensitivity, gender bias, and structured challenges faced by women in healthcare occupations. Our research would target interventions that could potentially create a more positive and well-being-focused work place culture for women healthcare workers. We present the hypothesis that positive wellness culture and holistic well-being practices will mutually reinforce each other and improve outcome measurements in our vulnerable population. For future study, we propose a definition of well-being that integrates mental health (mind) with physical health (body) resulting in a more complete approach to disease prevention and health promotion that also takes into consideration high life satisfaction, a sense of meaning or purpose, and the ability to manage stress. Furthermore, we want to implement prophylactic methods such as mindfulness practices, educational workshops, institutional policy, and professional- and peer-support to investigate the impact of more holistic well-being practices specific to women.
Footnotes
Acknowledgments
Our team would like to acknowledge the valuable contribution of the following individuals: Thomas Harrod, Associate Director of Reference, Instruction and Access of George Washington University’s Himmelfarb Health Science Library provided guidance in developing a search strategy that would provide rich data in a short window of time. We are also grateful to Ashley Drapeau, Physician Assistant at the George Washington University’s Resiliency & Well-Being Center, for her support in screening studies along with the authors.
Author Contributions
Conceptualization, VK and LAF; methodology, LAF and PGC; analysis, VK and PGC; writing—original draft, VK, HW, PGC, and LAF.; writing—review & editing, VK, PGC, and LAF; supervision, LAF; project administration, VK and PGC; funding acquisition, LAF. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the Rosemary Bowes, PhD, Women’s Mental Health Fund at the George Washington University School of Medicine and Health Sciences, which played no role in the design or conduct of this study.
Data Availability Statement
The template data collection form and extracted data may be available by request after the appropriate application process.