
Abstract
Introduction
Workload in oncology during a pandemic is expected to increase as manpower is shunted to other areas of need in combating the pandemic. This increased workload, coupled with the high care needs of cancer patients, can have negative effects on both healthcare providers and their patients.
Methods
This study aims to quantify the workload of medical oncologists compared to internal medicine physicians and general surgeons during the current COVID-19 pandemic, as well as the previous H1N1 pandemic in 2009.
Results
Our data showed decrease in inpatient and outpatient workload across all three specialties, but the decrease was least in medical oncology (medical oncology −18.5% inpatient and −3.8% outpatient, internal medicine −5.7% inpatient and −24.4% outpatient, general surgery −17.6% inpatient, and −39.1% outpatient). The decrease in general surgery workload was statistically significant. The proportion of emergency department admissions to medical oncology increased during the COVID-19 pandemic. Furthermore, the study compared the workload during COVID-19 with the prior H1N1 pandemic in 2009 and showed a more drastic decrease in patient numbers across all three specialties during COVID-19.
Discussion
We conclude that inpatient and outpatient workload in medical oncology remains high despite an ongoing COVID-19 pandemic. The inpatient medical oncology workload is largely contributed by the stable number of emergency department admissions, as patients who require urgent care will present to a healthcare facility, pandemic or not. Healthcare systems should maintain manpower in medical oncology to manage this vulnerable group of patients in light of the prolonged COVID-19 pandemic.
Introduction
Coronavirus disease 2019 (COVID-19) had spread across the globe in a span of 3 months from January to March 2020,
1
leading the World Health Organization to declare COVID-19 as a pandemic on 11 March 2020.
2
Singapore diagnosed its first imported case of COVID-19 on 23 January 2020 in a visitor from Wuhan.3,4 Following this, the Ministry of Health has put forth a progressive range of public health measures to mitigate the impact of COVID-19 on the healthcare system to prevent it from being overwhelmed. Most recently, a circuit breaker was introduced on 7 April 2020 to staunch further spread of COVID-19.5,6 Most businesses were required to stop work with the exception of essential services, such as healthcare, social services, and public transport. A timeline of COVID-19 development in Singapore is shown in Figure 1. Timeline of COVID-19 in Singapore.
During a pandemic, doctors are often asked to cut back on elective cases and postpone non-essential clinic reviews. Manpower is shunted to other areas of need, such as the screening area, emergency department, and intensive care units (ICU).7,8 In addition, healthcare staff was deployed to dormitories, community care facilities, and other hospitals to supplement manpower to care for patients with COVID-19. These personnel required strict segregation in view of the elevated risk of exposure. These measures taken to cope with the demands of a pandemic should be carefully balanced with a need to maintain standards of care for cancer patients. Irrespective of a pandemic, cancer continues to affect the at-risk population. We should continue oncology care to minimize any uptick in late stage cancer diagnosis or mortality due to delays in surveillance or treatment.
We hypothesize that the oncology workload remains high regardless of the evolving pandemic situation. A failure to recognize this during manpower planning for pandemic situations may result in a reduced workforce having to shoulder the heavy workload of oncology care. Heavy workload can impact the health of both oncologists and their patients.9,10 Physicians are at risk of fatigue and burnout due to the increased workload, leading to poor personal health.11,12 Patient care can also be affected by the high workload, with increased medical errors and lower patient satisfaction. 13
This study aims to quantify the workload of medical oncologists (ONC) compared to physicians in Internal Medicine (IM) and surgeons in General Surgery (GS) within a tertiary hospital during the COVID-19 pandemic. Second, we compared the trend of workload as the COVID-19 pandemic progressed to see if any parallel can be drawn to the previous H1N1 pandemic.
Methods
This study has been granted IRB exemption by the Singhealth Centralized Institutional Review Board, as only aggregated data were used with no identifiable patient data. This study was conducted in the largest hospital in Singapore, Singapore General Hospital (SGH), a multidisciplinary tertiary hospital with more than 1700 beds and 110 ICU beds, as well as the National Cancer Centre Singapore (NCCS), a dedicated outpatient cancer center in close proximity to SGH.14,15 NCCS has an ambulatory treatment unit (ATU) to administer the majority of chemotherapy outpatient in a clinic setting. 16 Patients who require complex multiday chemotherapy regimens or hospital admissions are managed as inpatients in SGH. In 2019, SGH managed nearly 750,000 visits in the outpatient setting and had 80,000 inpatient admissions. NCCS saw more than 150,000 patients visits in the outpatient clinics during the same time period.
Data were retrospectively extracted from the Electronic Medical Records (EMR) and included inpatient admission and outpatient visit history in three different specialties—ONC, IM, and GS. Admission and visit details include source, length of stay, specialty, primary physician, diagnosis code using the International Statistical Classification of Diseases and Related Health Problems 10th revision (ICD-10), outcome of admission and readmissions. The timeframe of the dataset was set at June 2019 (6 months before the start of the COVID-19 pandemic) to April 2020.
Inpatient admissions and outpatient visits per physician were used as a marker for physician workload. This was derived by dividing the average monthly patient load by the total number of consultant physicians in the specialty. Junior manpower consisting of House Officers, Medical Officers, Registrars, and Senior Residents were not included. No doctor was infected with COVID-19 in our hospital during the study time period, 15 we thus assumed the number of physicians to be similar before and during the COVID-19 pandemic. The comparator was the average number of patients in the preceding 6 months before the pandemic. ICU admissions were not included in the analysis, as ICU patients were cared for by intensive care physicians or anesthetists in SGH. They are not managed by their primary specialty physicians and were thus excluded from the analysis of workload.
We compared the inpatient admissions and outpatient visits during the COVID-19 pandemic with the most recent pandemic, the H1N1 influenza, that occurred in Singapore between May and September 2009. We attempted to compare the difference in workload between the current COVID-19 pandemic with the Severe Acute Respiratory Syndrome (SARS) epidemic in 2003. Unfortunately, there was missing information on manpower availability and outpatient workload two decades ago. This was thus removed from our final analysis.
A Wilcoxon–Mann–Whitney test was used to calculate statistical significance, which was set at p < 0.05. All statistical analyses were performed using IBM SPSS version 26.
Results
COVID-19 pandemic
Average number of patients per physician showed a decrease in workload in all specialties before and during COVID-19.

At the start of the COVID-19 pandemic, the number of inpatients per physician in ONC fluctuated from 7.3 (January 2020), 5.7 (February 2020), 6.2 (March 2020) to 4.3 (April 2020). Inpatients per physician in IM gradually increased during COVID-19 from 13.2 (January 2020), 11.0 (February 2020), 13.2 (March 2020) to 15.7 (April 2020). The inpatients per physician in GS mirrored the fluctuating ONC trend and showed from 7.3 (January 2020), 6.0 (February 2020), 6.4 (March 2020) to 5.7 (April 2020) (Figure 2a). (a) Monthly inpatient admission trend showed decrease in ONC and GS during COVID-19; (b) Monthly inpatient admissions during H1N1 in ONC, IM, and GS.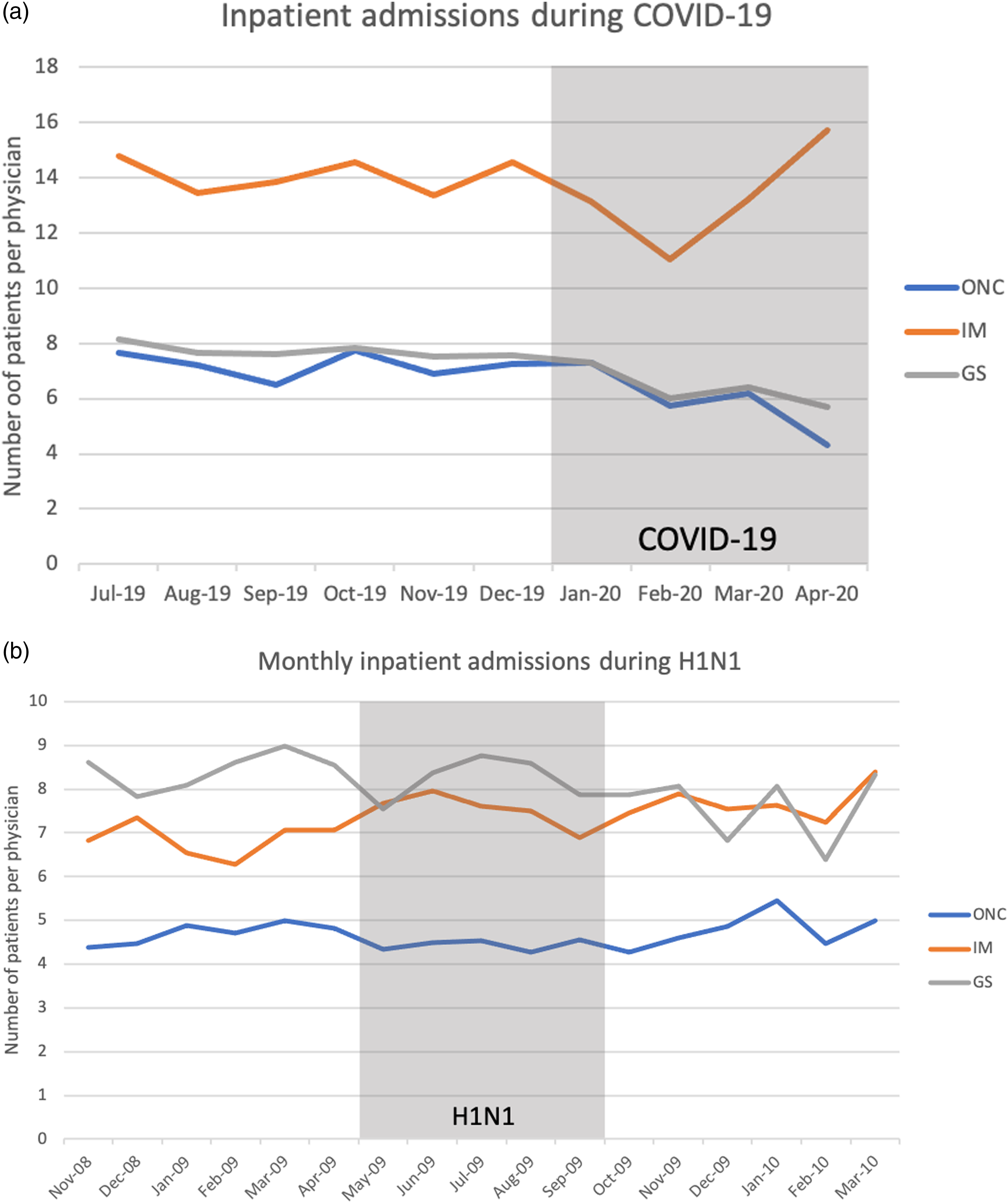
Outpatients per physician in ONC during COVID-19 maintained at 199.7 (January 2020), 180.1 (February 2020), 191.9 (March 2020), and fell slightly to 176.2 (April 2020) with the start of the circuit breaker. Outpatients per physician in IM decreased from 11.1 (January 2020), 7.2 (February 2020), 6.9 (March 2020) to 6.9 (April 2020). Similarly, GS outpatients per physician also dropped during COVID-19 but on a larger degree from 17.1 (January 2020), 8.8 (February 2020), 7.8 (March 2020) to 9.1 (April 2020) (Figure 3a). (a) Monthly outpatient visits showed a small drop in ONC during COVID-19; (b) Monthly outpatient visits during H1N1 in ONC, IM, and GS.
Inpatient admissions during COVID-19 showed minimal change in emergency department admissions to medical oncology and internal medicine.

H1N1 pandemic
The average monthly inpatient admissions per physician in ONC preceding the H1N1 pandemic (November 2008 to April 2009), during the H1N1 pandemic (May 2009 to September 2009), and after the H1N1 pandemic (October 2009 to March 2010) was 4.7, 4.4 (−5.8%) and 4.8 (+7.6%), respectively. Average monthly inpatient admissions per physician in IM pre-, during, and post-H1N1 were 6.9, 7.5 (+9.8%), and 7.7 (+2.2%). In GS, average monthly inpatient admissions per physician pre-, during, and post-H1N1 was 8.4, 8.2 (−2.5%) and 7.6 (−7.8%). Monthly inpatient admission trend in ONC, IM, and GS during the H1N1 pandemic are shown in Figure 2b.
Average monthly outpatient visits per physician in ONC before, during, and after the H1N1 pandemic was 75.7, 77.0 (+1.7%), and 76.2 (−1.0%), respectively. In IM, outpatient visits per physician was 10.1, 9.9 (−1.8%), and 10.2 (+3.2%) before, during, and after the pandemic. Outpatient visits per physician in GS before, during, and after the pandemic was 66.7, 67.0 (+0.4%), and 66.3 (−0.9%). The monthly outpatient visits in ONC, IM, and GS during the H1N1 pandemic are shown in Figure 3b.
Discussion
Inpatient and outpatient numbers in ONC showed a much smaller overall decrease compared to IM and GS during COVID-19. There was a larger decrease in inpatient admissions to ONC and a smaller drop in outpatient visits. Despite the decrease in inpatient admissions, there was an increase in the proportion of emergency department admissions to ONC. We can draw five key conclusions from these data.
First, ONC inpatient admission numbers decreased to a larger magnitude than the other specialties during the COVID-19 pandemic in Singapore. The drop in admission numbers during COVID-19 is also of a larger magnitude compared to the H1N1 pandemic. This decrease in ONC inpatient admission could be due to a variety of reasons, such as patient’s fear of contracting COVID-19 during hospital admission, or the physician’s higher threshold for admission given early studies showing that cancer patients are at elevated risk for COVID-19 infection and do poorly if they are coinfected. 17 Major oncological society also published guidelines for various cancers to minimize hospital visits and promote oral agents to minimize exposing patients to COVID-19. There was a bigger impact of COVID-19 on inpatient numbers compared to H1N1 which could be due to improved health awareness and literacy over the decade.
Second, outpatient visits in the ONC clinics saw a negligible drop during COVID-19 when compared against the other specialties. Our institution requested all healthcare professionals to cut back clinic load by 50% from February to free up resources in preparation for COVID-19. We actively called patients to postpone non-essential clinic appointments, routine surveillance visits, and regular follow-up consultations. This was more successful in IM and GS, with both departments showing more than 25% decrease in outpatient visits. However, ONC only managed to reduce outpatient visits by 3.8%. We postulate the reason for the minimal change in outpatient attendance may be due to patients’ perceived importance of continuing oncological treatment and follow-ups. Most patients were likely to be on active treatment for metastatic disease instead of surveillance and hence required continued care in the oncology clinic. Moreover, the changing paradigm of care from inpatient to outpatient during COVID-19 may also increase the number of outpatient visits.
Third, inpatient admissions from the emergency department to ONC decreased marginally during the COVID-19 pandemic when compared to GS, illustrating that patients who needed emergency cancer care will still present to the emergency department in spite of ongoing pandemic fears. However, there was no increase in emergency department admissions despite the drop in outpatient visits. We believe this is due to the success of community care services, such as home hospice, community nursing, and telehealth providers, in managing cancer patients without the need for a tertiary care facility. 18 Oncology and palliative home care are complementary and there was a smooth transition to continue care at home with the support of home hospice services. This bypassed the hurdles experienced by most telehealth providers who were required to overcome multiple administrative, legislative, and technological limitations in short weeks to initiate telemedicine during COVID-19.19,20
Fourth, the change in workload in the early phase of the COVID-19 and H1N1 pandemics are similar. There is a fall in inpatient admissions and outpatient visits in the first few months of the pandemic, before a recovery several months later. The recovery is more pronounced in the outpatient setting and occurred within one to 2 month during H1N1, while inpatient admissions remained more stable. The short delay in outpatient visits may be due to the backlog of patients who were initially hesitant about presenting themselves to a healthcare facility, but subsequently did so as the consequence of delaying cancer treatment weighs heavier in their minds than the fear of the pandemic. However, this may not play as much of a role in patients who require inpatient care and will present to the emergency department regardless.
Lastly, there is a significant rise in inpatient and outpatient numbers in ONC, IM, and GS in the decade between the two pandemics. Inpatient numbers increased by 50%, but outpatient numbers have skyrocketed to more than 150%. Medical oncologists in NCCS have three to four half-day clinics a week. Assuming 12 clinic sessions in a month, a typical ONC outpatient clinic has 6.3 patients in 2009, but now sees 15.8 patients per clinic session. This remarkable increase could be explained by the explosion of cancer therapeutics in the last decade,21,22 which has successfully managed to prolong patients’ life and thus result in more patients in the oncology clinics. Other contributory factors could be the larger number of cancer survivors with modern day adjuvant cancer therapy as well as an increase in the number of cancer patients with enhanced screening.
However, this study has its limitations. The data are available only till April 2020 and much is still unknown about the natural history of the COVID-19 pandemic moving forward. It will benefit from a follow-up study to evaluate if the distribution of workload post-COVID-19 mirrors that of the past H1N1 pandemic. The study uses a surrogate marker of inpatient admissions and outpatient visits per physician to ascertain workload. It does not factor in the complexity of each patient, length of stay, or ICU admission neither does it take into account the experience and number of doctors that were ill, redeployed, or away. We have intentionally omitted ICU admissions in our calculation of workload as ICU patients are centrally managed in our hospital and do not fall under the care of ONC, IM, or GS if they were admitted to ICU. Future research will benefit from a multifaceted look at other variables not available in our dataset such as case severity and physician experience. 23 The number of patients in GS may be lower as patients in the various subspecialties, such as colorectal surgery, breast surgery, and hepatobiliary surgery are not represented. Thus, comparison of workload in GS should be interpreted with caution. In addition, there may be a monthly flux of patients; hence, we used the 6 months average preceding both pandemics as the basis for comparison. Furthermore, February coincides with the Chinese New Year, a major festival in the Asian calendar and patient numbers usually decrease during this period. This factor may result in decreased patient numbers, though the likelihood is small, as the patient numbers in March and April were consistently lower than pre-COVID-19 figures.
In summary, we have shown in this study that ONC workload in pandemics remains higher than other specialties. The workload will likely remain high during this extended COVID-19 pandemic and healthcare systems should make provisions for this increased workload in ONC to ensure optimal care for cancer patients continue to be delivered. This finding has implications for healthcare manpower planning purposes and healthcare systems must factor in necessary personnel to address the high workload in spite of the ongoing pandemic for optimal outcomes. The COVID-19 pandemic appears to be a drawn-out one, but cancer patients and their oncologists should not be made to bear the consequence of a heavier workload as manpower is shunted elsewhere to combat the pandemic. Optimal oncological care must continue, come what may, pandemic or not.
Footnotes
Acknowledgments
We would like to express our gratitude to our colleagues and leadership from the National Cancer Centre Singapore and Singapore General Hospital for their support. We would also like to thank all healthcare staff and patients for their willingness to participate in our research programs.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author contributions
JC conceived the study, gathered the data, and interpreted the results.
JC and SZ performed the statistical analysis.
JC, VY, SH and QZ drafted the manuscript.
All authors provided their critical review of the manuscript for insightful intellectual content.
JC attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
JC also affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted.
Ethical approval
Ethical approval for this study was waived by SingHealth Centralized Institutional Review Board because it is a quality improvement project meant to improve care delivery to patients. This study was completed in accordance with the Helsinki Declaration (CIRB 2020/3046).
Informed consent
The study was exempted from ethical review by the SingHealth Centralized Institutional Review Board (CIRB number 2020/3046).