
Abstract
User feedback is an important element of health-service evaluation and can be used to improve services but can be difficult to obtain, particularly in acute care situations. As part of a national study, we explored stakeholders’ perspectives on paediatric critical care retrieval processes through questionnaires and interviews. Obtaining feedback in a highly charged, stressful and busy paediatric intensive care unit (PICU) environment is fraught with difficulties so we aimed to optimise each stage of data collection by being both proactive and reactive. Patient and public involvement occurred throughout and engagement with sites and supporting local research staff to approach and recruit families were prioritised. High-quality study materials were developed to reduce local staff burden and promote and maintain study awareness. We describe strategies used and what worked/did not work. We suggest approaches for optimising elicitation of parents’ experiences in difficult circumstances, highlighting the importance of engagement and commitment of PICU staff.
Background
Learning from patients about the care they have received is crucial for improving health-care services (1). A number of mandatory approaches for collecting patient experience data have been established within the National Health Service (NHS) in England, including the Friends and Family Test (FFT) (2). Local organisations also collect feedback through a variety of different methods such as surveys, patient forums, and informal feedback from Patient Liaison Services (1). Despite FFT being the largest source of patient opinion worldwide, it provides limited information and, in the absence of any further data, cannot drive change (3). Collecting actionable feedback and making changes based on the findings to improve services remains a challenge.
Within paediatric services, parents are often asked to provide feedback about their experiences of care received by their child, frequently because children are unable to provide feedback themselves due to their age, cognitive ability and/or health condition (4). Ideally, however, both parents and children and young people (CYP) should be asked to provide feedback as they experience the same situation differently (5).
Since the centralisation of paediatric intensive care services in the United Kingdom (UK) (6), specialist paediatric critical care transport teams (PCCTs) have been established to travel to local hospitals to assist in stabilising and transferring critically ill children to regional paediatric intensive care units (PICUs) (7). In the UK approximately 5000 critically ill children require emergency transport to PICU every year (8). Stresses associated with a PICU admission are well documented, including long-term psychological trauma (9–11). Patients’ and families’ experiences associated with critical care retrieval are less well understood, but parents of sick children have described the process of PICU retrieval as ‘the worst journey of their lives’ (11,12).
To date feedback about the retrieval of critically ill children has been sought via questionnaires developed by individual services, given directly by PCCTs to families, and local audit data indicate that return rates have generally been low (<20%). Specific reasons for low response rates in this context are unknown, but possible reasons are that staff may feel it inappropriate to approach families at a time of great stress and/or families may be simply too anxious to provide feedback. Timing of the approach to families is clearly extremely important.
The DEPICT Study
The DEPICT study (
Study Context
There are 24 PICUs located across 21 NHS Trusts in England and Wales and all participated in the study. Within the relatively small PICU community, there is a well-established network of existing relationships that helped to facilitate the recruitment of committed site Principal Investigators and provided multiple opportunities for the central research team to engage and network with staff, including attending meetings of the Paediatric Intensive Care Society and Acute Transport Group. The PICUs have a history of working collaboratively on successful multicenter trials (14,15) and have the infrastructure to participate in large studies, although variability exists in resources available for research across the sites.
A detailed description of the methods is provided in the final study report (16).
Anticipated Challenges and Strategies to Increase User Feedback
In view of the historically low uptake of opportunities to provide feedback about PCCTs and the nature of the situation in which we were asking families to do this, we anticipated a number of challenges. A range of strategies was therefore employed proactively to increase user engagement at each stage of the study (Table 1).
Anticipated Challenges of Recruitment and Strategies Used to Increase User Engagement.

CI, Chief investigator; RN, Research nurse; PI, Principal investigator; PICU, Paediatric intensive care unit; CYP, children and young people.
Questionnaire Study
Each PICU team kept a log of eligible participants and outcomes of decisions to approach and consent.
Recruitment
Recognising that families of critically ill children are likely to be highly stressed, written consent was deferred to a time after PICU admission judged to be suitable by the clinical team, although we recommended speaking to families within the first 24–48 h to facilitate recruitment of short-stay admissions. Parents were offered a number of options to facilitate questionnaire completion based on evidence that providing participants with a choice of methods for completion increases response rates (17–19).
To increase saliency a range of visual cues was used to enhance awareness of the study in the PICUs (Figure 1). Particular attention was given to the ‘look and feel’ of the questionnaire to increase families’ perceptions of study integrity. The questionnaire was developed specifically for this study and was based on a review of relevant literature and existing questionnaires used by retrieval teams to gain feedback, as well as the experience of the study team, steering group and parent representatives to further inform content and format. The questionnaire was piloted with six families from two PICUs to check coherence, clarity and acceptability.

Examples of visual cues used to enhance awareness of the study in the PICUs.
Recruitment of Under-Represented Families
Bereaved families are often under-represented within health services research but evidence suggests that participation can be a positive experience for parents, allowing them the opportunity to reflect, remember their child and help improve the experience of subsequent bereaved families (20,21). Excluding bereaved families would also introduce selection bias. Families who do not speak/read English are also often under-represented and these families tend to have a poorer experience of health care (22). Additional measures were taken to facilitate the inclusion of these groups (Table 1).
Table 1 summarises other strategies used for subsequent stages of the study which involved re-contacting and recruiting families for interviews (including children and bereaved parents), collection of follow-up data by questionnaire at 12 months and attendance at stakeholder workshops. PICU staff were also invited to provide feedback on the study set-up, recruitment and support from the central research team via a brief, anonymous questionnaire.
Effectiveness of Methods Used to Improve Recruitment
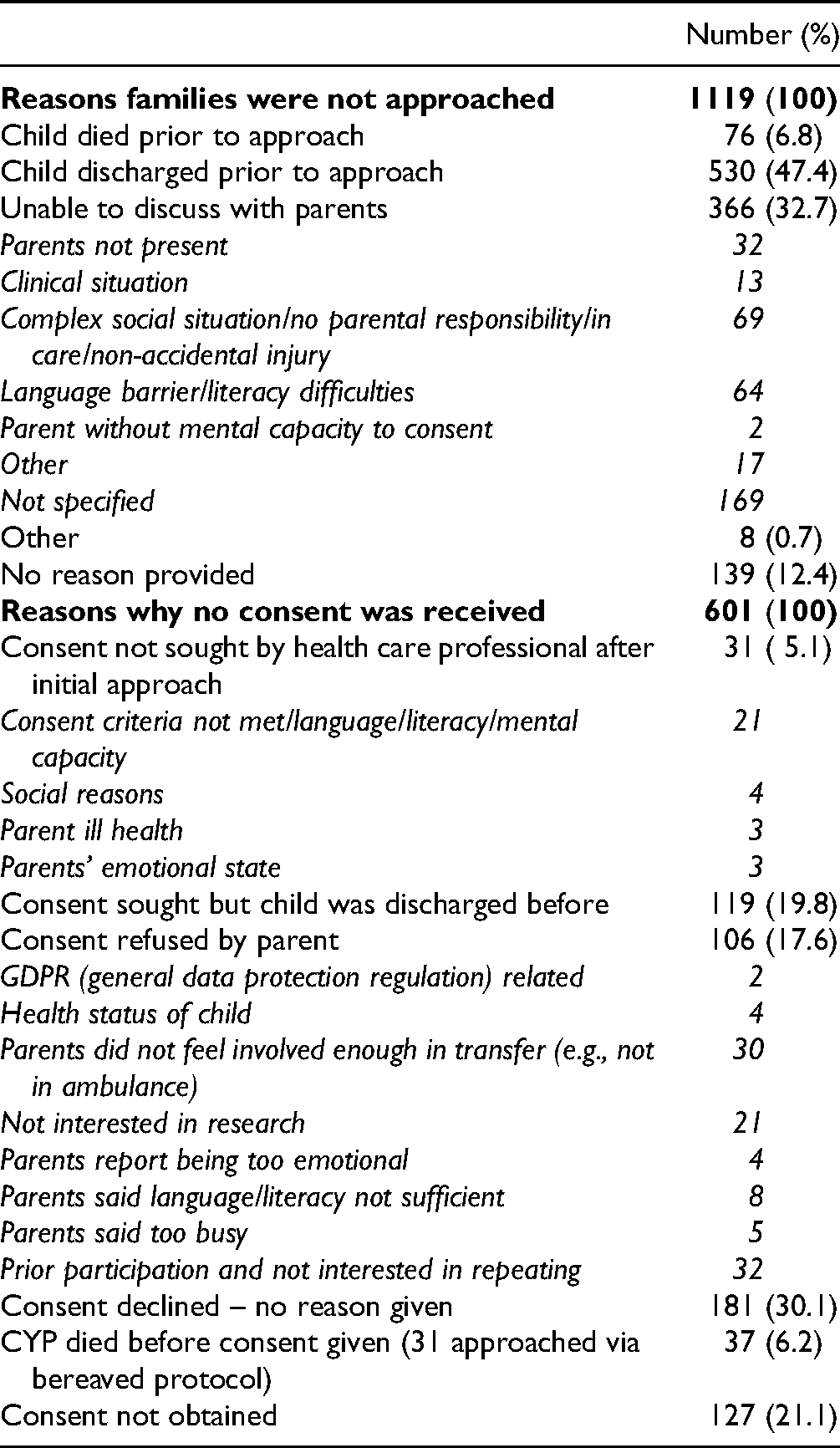
Figure 2 and Supplementary Figures S1-S3 indicate the numbers of families who were approached and participated at each stage of the study. Reasons why families were not approached or recruited are shown in Table 2.

Flow diagram of participants recruited into the questionnaire study.
Reasons Families Were not Approached or Consent was not Received for Participation.
Questionnaire Study
Based on the number of children transported to PICU and data about response rates in questionnaire-based research (23), we estimated receiving 800–1000 completed questionnaires (16%–20% response rate). During baseline data collection (January 2018–January 2019), 4558 families were identified as eligible for participation (Figure 2). Of 3439 approached for consent, 2838 consented to the initial questionnaire, of whom 2133 returned at least a partially completed questionnaire (47% of those eligible overall; 62% of those approached for consent), more than double the number expected.
On the screening logs 110 families were identified as non-English speaking. Ninety-three families were not approached due to lack of available interpreter services/appropriate translated materials; 17 were given an alternative language pack and 6 completed questionnaires were received. One site reported that two families declined participation because of translation errors of the Urdu and Bengali questionnaires which, for those with low literacy levels, were difficult to comprehend.
Interview Study
We planned to recruit approximately 50 parents, a sufficient number to capture the range of parents’ experiences across the different models of care delivery (24). A large number of families initially consented to being contacted about interview participation (Figure S1) of whom 100 families were contacted and 30 interviews were completed, at which point no new evidence was being obtained.
We hoped to recruit 20–30 CYP but were unsuccessful and recruited none. Finding eligible children was challenging due to the young age (<2 years) of most CYP transported. Two interviewed families whose child was eligible to participate were asked if their child would like to participate: one declined as the parent was concerned about the process of revisiting the event and one did not respond after initially expressing interest.
12-Month Follow-up Questionnaires
We originally anticipated receiving 200–250 questionnaires based on the estimated original questionnaire responses of 800–1000. We received 520 completed questionnaires, representing 21% of those who consented at baseline to receive follow-up questionnaires but 29% of those who could be contacted and sent a follow-up questionnaire (Figure S2).
Stakeholder Workshops
Our aim was for approximately 30 stakeholders to attend workshops (5–7 families and 5–7 clinicians at each of two workshops) (Figure S3). For the first workshop (12/3/20) six parents registered to attend but only three attended on the day; those who did not attend cited the COVID-19 pandemic. The second scheduled workshop was cancelled due to COVID-19.
PICU Staff Feedback
Twenty-seven surveys were received from 16/21 (76%) Trusts. Results of measures put in place to support staff are summarised in Figure S4. Study set-up, study materials and support received from the research team were positively evaluated by most staff. They highlighted the difficulty of approaching families when there was a language barrier and suggested having finances available to use translators would have been useful to encourage non-English speaking families to participate. Suggestions for future collection of parent feedback included a shorter, anonymous questionnaire with options for completion including the provision of tablets with preloaded surveys.
Discussion
User feedback is an important element of health service evaluation but historically has proved difficult to obtain for PCCTs. We have reflected on our methods and effectiveness of collecting feedback to inform learning for both future research and routine collection of patient experience data. It is clear that a large proportion of families of CYP transported to PICU are willing to provide feedback about their experience. Our findings suggest it is feasible and acceptable to acquire user feedback within a critical care setting but it requires careful consideration about how and when to approach parents. Of note, in our study parental ratings of the transport service were generally very high, so motivation to provide feedback may also have been influenced by the experience they had and a desire to thank the team.
Recognising that obtaining feedback in a highly charged, stressful and busy critical care environment is fraught with difficulties, we tasked ourselves with optimising each stage of the process by being both proactive and reactive. We placed great importance on the role of patient and public involvement (PPI) (25), working closely with expert parents and professionals and ensuring that PPI was embedded in the research. Two parents and three external PICU/transport staff were members of the central research team and were integral to each stage of the project design, implementation and evaluation of progress.
Throughout the study, engagement with sites and supporting local research staff (directly and indirectly) were prioritised. The central research team was responsive to local staff need, initiating regular (initially weekly then monthly) contact and being available to answer questions about eligibility and recruitment and requests for support. We also prioritised the development of high-quality study materials, pre-packed questionnaires and appropriate study cues which, while resource intensive for the central research team, helped to reduce local staff burden and promote and maintain awareness of the study across the units. We believe our higher than anticipated rates of approach and recruitment are testament to our strategy and to the commitment and engagement of the local PICU teams. Previous studies have identified local ‘gate-keeping’ in terms of who is or is not approached (26) but we suggest that adequately resourcing site engagement helps to reduce this.
The high response rate also suggests families found the questionnaire content relevant and acceptable, highlighting the importance of engaging with families during development and piloting to ensure the feasibility and acceptability of what we were asking families to do. However, although families could complete the questionnaire online, the majority opted for paper completion, possibly because that was their preference or because access to the online questionnaire was not efficient enough. Providing an additional method of accessing the e-questionnaire such as on a tablet-computer while in PICU may have increased response rates. Improving online response rates for future research or routine feedback would be more efficient in terms of preparation and data input. However, the evidence about offering mixed-mode methods of collecting questionnaire data to increase response rates (17–19) suggests families should still be offered options for questionnaire completion.
Despite our successes, there were some areas in which we did not do well. Although study materials were translated into five languages, we recruited very few non-English speaking families. Many were not approached as no interpreter was available and we did not have translated materials for all languages. Furthermore, during times of distress and anxiety cognitive processing may be impacted as well as literacy levels (11,27). Having study information and questionnaires available on a tablet computer with read-aloud functionality for alternative languages may be a cost-effective and logistically feasible way to improve response rates among this group in future. We also recruited a very low number of bereaved families. Not all families whose child died in PICU were approached. It is unclear why this was, but sites may not have been clear about the procedures of the bereaved protocol or felt uncomfortable implementing it. Bereaved families are frequently excluded from research (20,21) and may not be asked about their experiences yet they are often willing and want to participate and this needs to be addressed in future.
A sufficient number of parents were interviewed but we did not recruit any CYP, primarily due to their young age and because most were sedated and ventilated for the transport. However, a few CYP were willing to provide feedback by completing the questionnaire so a CYP-specific questionnaire for later postal completion might have increased engagement with them. Furthermore, completing a questionnaire rather than participating in an interview may have reduced parental concerns over the effects on their child of revisiting the event.
Collecting follow-up data is important but challenging (28). Re-engaging with families 12 months after their initial recruitment was not always feasible which meant the response rate was lower than anticipated. Re-engaging families is resource intensive yet if we want families to complete follow-up measures we suggest the same level of commitment and allocation of resources are required as we were able to dedicate initially. Some strategies we employed, such as personalising emails and sending email reminders, likely increased our response rate but we were unable to use a similar reminder method for those without email addresses who were sent postal questionnaires, where the return rate was lower.
Although our successes with initial recruitment are to be celebrated, they resulted in unanticipated demands on the central research team including an increased number of families to follow up at 12 months; additional time supporting sites and related administration tasks; and additional time pressures related to data entry, cleaning and analysis. Finally, COVID-19 was an unforeseen challenge that we could not overcome in the study time frame. However, using online technologies with materials provided in advance are consideration for future dissemination and elicitation of participant feedback.
Conclusion
We used a number of effective strategies for recruiting families and, learning from our experiences, suggest approaches to maximise response rates for future research and/or routine collection of patient experience data (Box 1). Importantly, despite the stressful situation they were in, a high proportion of families were willing, and wanted, to provide feedback. The engagement and commitment of PICU staff were crucial for maximising parental participation and should not be under-estimated when developing strategies for asking parents for feedback. How to engage under-represented populations as well as CYP themselves needs to be addressed and understanding and facilitating families’ preferences are important considerations in maximising feedback.
Strategies for increasing response rates to parent experience questionnaires
Clear information about the purpose of the questionnaire and how the information given will be used to improve the service Questionnaire should be short Multi-mode methods for completion offered Online versions available on tablets for completion before discharge and via an online link to complete later Paper versions in booklet format, printed in colour and on high quality paper; stamped return envelope for confidential return Available in multiple languages with speak aloud functionality Options for return of questionnaire (post-box on PICU, free post envelope) Assurances about anonymity and security of the data Opportunity to provide free text comments Indication of how previous information has been used – ‘you said, we did’ Contact details for the team if they want to discuss anything further Thank the participant!
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221143949 - Supplemental material for What Happens When you Ask for Feedback? Anticipating and Addressing Challenges Can Be Effective for Eliciting Parents’ Views About Their Critically Ill Child's Retrieval to Paediatric Intensive Care
Supplemental material, sj-docx-1-jpx-10.1177_23743735221143949 for What Happens When you Ask for Feedback? Anticipating and Addressing Challenges Can Be Effective for Eliciting Parents’ Views About Their Critically Ill Child's Retrieval to Paediatric Intensive Care by Victoria Barber, Ruth Evans, Padmanabhan Ramnarayan and Jo Wray in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735221143949 - Supplemental material for What Happens When you Ask for Feedback? Anticipating and Addressing Challenges Can Be Effective for Eliciting Parents’ Views About Their Critically Ill Child's Retrieval to Paediatric Intensive Care
Supplemental material, sj-docx-2-jpx-10.1177_23743735221143949 for What Happens When you Ask for Feedback? Anticipating and Addressing Challenges Can Be Effective for Eliciting Parents’ Views About Their Critically Ill Child's Retrieval to Paediatric Intensive Care by Victoria Barber, Ruth Evans, Padmanabhan Ramnarayan and Jo Wray in Journal of Patient Experience
Supplemental Material
sj-docx-3-jpx-10.1177_23743735221143949 - Supplemental material for What Happens When you Ask for Feedback? Anticipating and Addressing Challenges Can Be Effective for Eliciting Parents’ Views About Their Critically Ill Child's Retrieval to Paediatric Intensive Care
Supplemental material, sj-docx-3-jpx-10.1177_23743735221143949 for What Happens When you Ask for Feedback? Anticipating and Addressing Challenges Can Be Effective for Eliciting Parents’ Views About Their Critically Ill Child's Retrieval to Paediatric Intensive Care by Victoria Barber, Ruth Evans, Padmanabhan Ramnarayan and Jo Wray in Journal of Patient Experience
Supplemental Material
sj-docx-4-jpx-10.1177_23743735221143949 - Supplemental material for What Happens When you Ask for Feedback? Anticipating and Addressing Challenges Can Be Effective for Eliciting Parents’ Views About Their Critically Ill Child's Retrieval to Paediatric Intensive Care
Supplemental material, sj-docx-4-jpx-10.1177_23743735221143949 for What Happens When you Ask for Feedback? Anticipating and Addressing Challenges Can Be Effective for Eliciting Parents’ Views About Their Critically Ill Child's Retrieval to Paediatric Intensive Care by Victoria Barber, Ruth Evans, Padmanabhan Ramnarayan and Jo Wray in Journal of Patient Experience
Footnotes
Author Contributions
PR was the Chief Investigator for DEPICT. PR and JW wrote the protocol (with other team members). RE developed the patient information resources. RE and VB led the acquisition, analysis and interpretation of the data reported in this manuscript. VB drafted the manuscript and all authors critically reviewed and approved the final version.
Ethical Approval
This study was approved by the National Research Ethics Service – London Riverside Committee (ref: 17/LO/1267).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Institute for Health Research Health Services and Delivery Research programme (Project No: 15/136/45). The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the NIHR HS&DR programme or the Department of Health. The funder had no role in the study.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the National Research Ethics Service approved protocols.
Statement of Informed Consent
All participants provided written consent prior to their participation in the study, which included consent for anonymised data to be published.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.