
Abstract
This study aimed to describe patients’ perceptions of tele-rehabilitation (TR) and investigate the association between TR-related factors and both the patients’ age and type of rehabilitation services. A cross-sectional survey was conducted to obtain data about patients’ demographic and medical information, technological familiarity as well as patients’ experience and opinions about TR. The 227 patients completing the survey reported a mean ± SD age of 40.7 ± 13.9 years and musculoskeletal disorders as the most common condition treated by TR. The majority of patients expressed satisfaction and confidence with their therapists’ ability to assess and treat their problems using TR. Approximately 75.3% of participants stated that therapists demonstrated a strong understanding of their health conditions, while 82% reported that TR entailed a convenient service during COVID-19. The study found associations between age and patient's ability and confidence to use technology as well as a relationship between the type of treatment received and participants’ overall opinions. Patients demonstrated acceptance, confidence, and satisfaction with TR during COVID-19. Patient age and treatment type fulfill a major role in patients’ perceptions of TR.
Introduction
Tele-rehabilitation (TR) is a rehabilitation service provided at a distance through either audio and/or video digital media. It is communally used to address patient needs (1‐3) through diagnostic, therapeutic, preventative, counseling, and consultative services via interactive communication technology (4). TR contains several advantages, such as reduced treatment expenses, time savings, improved access, and continued care for clients with infectious diseases.
Physical therapists (PTs) as a provision adopt a mixture of hands-on and hands-off skills to treat patients, which most often requires a huge physical contact between patient and therapist making virtual treatment sometimes difficult and may be not accepted by patients and/or caregivers. TR services still require improvements, especially for treating home-based patients with a trained team and technological model of care. In particular, PTs comprise primary practitioners that possess experience in managing injuries, functional recovery, movement, and pain. Prior research (5) reported that in comparison to office-based PT, TR programs demonstrate similar levels of functional improvements among patients with knee Osteoarthritis (OA) and recommended TR for older populations in remote areas. A systematic review revealed strong concurrent validity (6) for PT assessments that use range of motion, muscle strength, gait, balance, pain, swelling, and body functions.
Previous studies (7,8) investigating TR contain limitations, including small sample sizes and the lack of a control group. Moreover, these studies failed to investigate important aspects of TR, including patients’ perceptions of remote care. Few studies have focused on patients’ satisfaction, with only two investigations examining chronic pain sufferers’ perspectives of TR (9,10). While a previous study found that people with knee and/or hip OA report positive perceptions about TR for providing physical therapist-prescribed exercise services (11), few works investigate whether the same perceptions exist among patients with other health conditions assessed and treated by different rehabilitation team members. This gap highlights the need for studying patients’ experience with TR and technologies used to deliver rehabilitation services. Therefore, this study aims to describe patients’ experience with TR by exploring patients’ familiarity, experience, and opinions of TR and its technology in Saudi Arabia. Moreover, this investigation considers patients’ age and type of rehabilitation services along with the association between those and other factors.
Methodology
Study Design
A descriptive cross-sectional study ethically approved by the Institutional Review Board of the College of Medicine at King Saud University, Riyadh, Saudi Arabia [Project No. E-20-6573; dated May 4, 2020]. The study took place at the Medical Rehabilitation Department (MRD) at King Saud University Medical City (KSUMC) in Riyadh, Saudi Arabia.
Participants
All participants/caregivers were recruited from the MRD at KSUMC. Eligible patients were those who received remote treatment using the TR program in the period from June 1 to September 30, 2020. Patients who have been treated using the TR program were called to complete a semi-structured survey designed and validated by the research team. All patients with any age or diagnoses referred to the MRD were eligible to participate in the study.
TR Program
TR program embraces the concept of providing interactive remote consultations and treatment sessions for patients who require rehabilitation services on a virtual platform. The program has been designed to facilitate rehabilitation services regardless of the patient locations using audio/video conference call in special virtual clinic platform and system developed by the Information and Technology department at KSUMC using the Microsoft webinar and internal eSihi (Electronic Medical Record system) software.
The process of recruiting patients to the program featured three steps.
The triage coordinator reviewed patients’ electronic referrals and medical files by considering diagnoses and complaints before evaluating possibilities and risks of serving the patient through the program. The triage coordinator is a senior physical therapist with 17 years of experience. He has been the triage coordinator for about 5 years before the beginning of the study. There is an unpublished triage system used at the Medical Rehabilitation Department since 2015 which has been built by expert therapists and the research team inside the department. All applicable patients were referred to a specialized therapist. During the initial appointment, the therapist assesses the patient condition and schedules him/her through the virtual clinic. During the consultation, the therapist performs the usual evaluation and provides a comprehensive treatment plan, sends the exercise program to the patient using the Physiotools program, and schedules him/her for follow-up appointments. This initial assessment happens via videoconference.
If the patient's case is complex and the therapists determined that a videoconference cannot be used to make the decision and treat the patient. Then, face-to-face assessment is crucial and the therapist will schedule an appointment for the patient to be seen physically at the MRD, and if it is possible, the patient will then move back to virtual follow-up when it is applicable.
The treatment session may include thermotherapy (application of heat or cold), therapeutic exercises, active and assistive limb mobilization, flexibility training, aerobic exercises, balance, and gait training. All the participants or caregivers were provided with handouts of treatment procedure (including appropriate time and number of repetitions) to make sure nothing of treatment missed out.
The TR program was performed as a complete treatment session. During the session, the therapist fully assesses and treats the patient. The patient has been asked to perform the required treatment while the therapist watches to make sure the patient can do the treatment appropriately. The number of sessions and time of sessions were varied according to the case and the need of the patient. The therapist-patient meeting happens virtually. If there are any home exercises needed, the therapist explained such exercises and made sure the patient can apply in a correct manner.
Survey Instrument
This study examined patients’ experiences and opinions about TR by using a semi-structured survey, which underwent development processes according to a very structured method to design the survey. The first step was to identify the best method and type of survey to be used, communication method, and the length of the survey. The second step was to determine the target population and to gather all required information and necessary questions, gathered from the literature review in the areas of TR, telehealth, technology adoption, and other related fields as well as feedback from senior physical therapists through a focus group session. The survey was then tested on 15 patients who demonstrated similar characteristics to the targeted sample. This pilot aimed to verify the survey structure, absence of ambiguous or leading questions, clarity of wording, inclusion of important issues, and time required to complete the survey. Based on this testing, a revision and the final version of the questionnaire was created. Appendix 1 shows the used survey.
All patients who received virtual rehabilitation services were invited to complete the survey. Once the patient was discharged from the TR program, s/he was listed to be called by the investigators. Before completion, participants received a clear introduction of the study purpose. The survey included four major areas: demographic and medical information, patients’ familiarity, experience, and opinions about TR. After obtaining participant consent, a data collection team conducted the survey in a 10-min phone call using department phones at the end of the intervention period.
Data Analysis
All statistical analyses employed SPSS Statistics 25 (IBM Inc., Chicago, IL, USA). Descriptive statistics for all participants expressed the frequency and percentage for all categories. Researchers investigated associations using a chi-square test with the P value set at ≤0.05.
Results
Researchers contacted 275 participants to complete the survey, 227 of whom responded, yielding an 82.5% response rate and mean age of 40.7 ± 13.9 years. The majority of participants fell in the 40–60- and then 25–39-year-old categories, representing 46% and 24%, respectively. Most participants were female (73%), unemployed (61%), and obtained a bachelor’s degree (35%) or a high school diploma (25%). The most common treatments for this sample included Musculoskeletal (MSK) and Orthopedic PT. Nearly 57% of the sample never received any prior physical therapy treatment sessions in the department. More details about the breakdown of personal information appear in Table 1.
Demographic and Other Characteristics.

Most patients felt very (59%) or moderately confident (25%) that their therapists successfully assessed and treated their problems using TR. Most respondents would recommend this service to others, especially during COVID-19 pandemic. However, more than 60% of the sample believed that TR failed to provide as effective a service as traditional face-to-face assessment (Table 2). More than half of the sample (55%) experienced improvements in their condition after TR treatment. Most respondents reported a high level of satisfaction with TR. Finally, many patients (83%) did not face any technical problems during TR, which, along with other details, appears in Table 2.
Patient Experience with TR.

Approximately 22% of patients believed that therapists experienced challenges during the assessment. Those patients were questioned more to understand the kinds of challenges they mean using a qualitative analysis. Among this group, more than half (54%) believed that the therapist struggled to reach the correct diagnosis, and 15% described problems with the technologies. The remainder reported that the therapist's assessment challenges related to other issues, such as commitment to the treatment program (11.5%), inability to attend in person (11.5%), and uselessness of the software (8%).
Approximately 17.2% of participants reported technical problems during TR. Among those patients, 38% reported difficulties with software, 28% encountered impaired internet signals or connection interruptions, 24% encountered audio and/or visual problems, and the remaining 10% reported communication difficulties with the therapist.
Most participants (98.7%) accessed the internet through smartphones, while the rest used other devices, such as tablets, laptops, and desktop computers, with more than 90% of respondents confident in using electronic devices. In addition, most participants (86%) were very familiar in using the internet during past 5 years, with 96% of patients using it daily.
Table 3 and Figure 1 show patients’ opinions about their TR experience. About 75.3% of respondents agreed that the therapist possessed a strong understanding of their health conditions. Most participants (96%) failed to find any breach of privacy during the TR process. While 36% of respondents believed that phone calls provided equal benefits to a face-to-face treatment, 48% felt otherwise (16% patients were neutral). Similarly, 43% reported that using video conferencing equaled to face-to-face conversations while 35% disagreed with this opinion (22% of patients were neutral).

Patient opinion with respect to TR experience.
Patient Opinion with Respect to TR Experience.
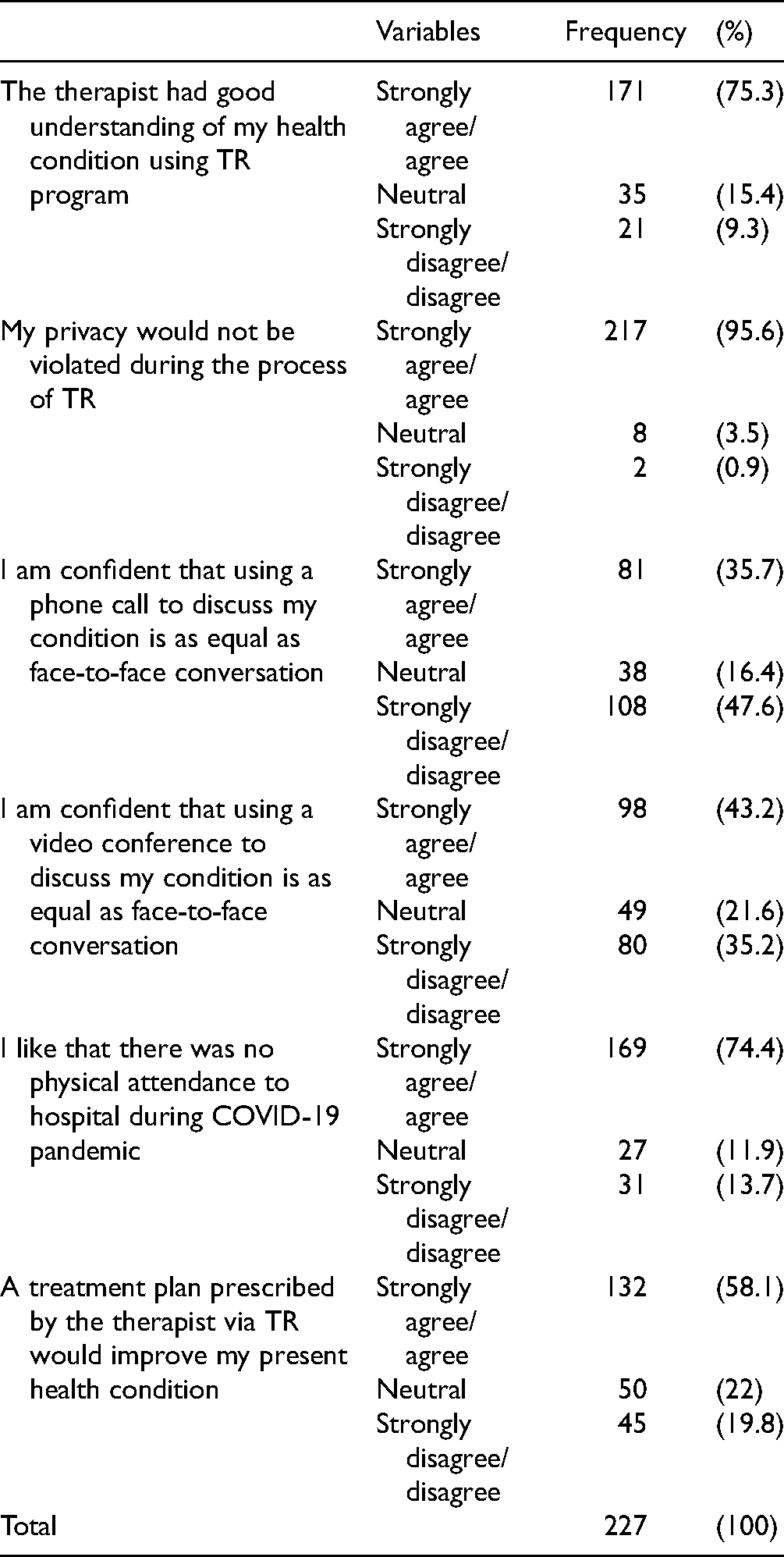
Most participants (74%) preferred not to physically attend their appointment during the pandemic and 82% of the participants stated that TR constituted a convenient form of healthcare during the COVID-19 pandemic. Most respondents agreed that TR comprised an appropriate (70%), useful (64%), effective (57%), affordable (89%), and safe (94%) treatment method during COVID-19. While 58% of the participants agreed that a TR-based treatment plan would improve their present health conditions, 20% disagreed with this opinion.
Results concerning the association between age and other factors appear in Table 4. Age demonstrated a significant association with the presence of technical difficulties and/or problems, confidence in using electronic devices, and belief in the therapist's ability to completely monitor the patients’ health via TR.
Associations Between Age and Current Treatment Provided, and Other Factors.

Significant associations between treatments provided and other factors appear in Table 4. The current treatment provided was significantly associated with the opinions about therapists’ understanding of patients’ health through TR, and belief in therapists’ ability to completely monitor patients’ health conditions via TR.
Discussion
The current study aimed to describe patients’ experiences and opinions regarding TR. Most patients expressed moderate-to-high confidence that therapists can assess and treat health conditions when using TR. Furthermore, the majority of patients indicated satisfaction when using TR and believed that therapists strongly understood their health conditions. However, most respondents concurred that face-to-face assessment possesses greater effectiveness than TR. Patients reported disagreement about their confidence in using audio or video conferences to discuss health conditions. Moreover, the study found an association between patients’ age and type of rehabilitation services along with other factors pertaining to TR. These findings support previous studies, one of which reported high satisfaction levels when using TR services and the relationship between therapists and patients (12). In addition, another study from Sweden found that patients treated via TR after shoulder joint replacement reported that therapists treated their pain and guided them during home exercise programs (13). However, another paper from Canada revealed that patient populations and settings failed to impact high rates of satisfaction among patients and therapists (14).
The greatest beneficiaries of TR involved patients in the 40–60-year-old category, followed by patients aged 25–39 years. Patients over 60 comprised only 7.5% of the participants. Moreover, most respondents held educational degrees of high school or above, indicating that their educational status suggests familiarity with technology. MSK PT represented the most common type of rehabilitation services among participants. Prior research reported that TR was highly effective among patients with MSK conditions, even in older demographics (15). This finding, combined with the present study, indicates the need to continue ensuring the effectiveness of TR for MSK disorders and all other health conditions.
Participants expressed confidence about therapists’ knowledge and abilities to assess and treat health conditions via TR. Most respondents (95%) reported that TR services protected privacy, which related to moderate-to-high levels of satisfaction during TR assessment and treatment. These findings support previous studies about the convenience, ease of use, and privacy of TR (11). In addition to safety, privacy comprises another issue mentioned in the American Telemedicine Association's (ATA) A Blueprint for Telerehabilitation Guidelines in 2010 (16) as well as in Saudi culture.
Most participants deemed face-to-face assessment is more effective than TR. This finding may result from the presence of chronic pain, which, according to previous evidence done in the Netherlands, reduced patients’ confidence in performing exercises via TR (9). Moreover, prior research reported that physical contact constitutes an important factor for building trust between therapists and patients (17). However, 78% of participants in the present study reported that therapists correctly assessed patients’ health conditions via TR, while 22% felt concerned about the diagnoses. This study highlighted the need for investigations that determine whether exercise performance outcomes differ based on physical touch. Previous evidence found that the absence of physical contact impedes the formation of an emotional bond (9). Conversely, previous research from Canada reported that patients found TR “at least as effective as traditional face-to-face physical therapy following primary total joint arthroplasty (18).”
Most participants experienced improvements after TR treatment. This finding concurs with previous literature in which patients reported that therapists customized exercise treatments to their ability, pain, and fatigue (19), which studies of patients with OA supported over the short term (20,21). Moreover, previous evidence found that only 23% of patients preferred the lack of physical contact during TR (11). Furthermore, the type of medical condition may fulfill a role in TR. These collective findings suggest several issues regarding the relationship between therapists and patients, quality of health information, and organizational challenges (22). Therapists can address concerns about the therapeutic relationship by scheduling at least one in-person session with the patient.
Australian participants indicate a preference for audio calls during TR, which concurs with a study of clients who have undergone arthroplasty reporting relatively equivalent outcomes between a six-week in-person rehab program and internet-based TR (23). Similarly, a UK-based phone service revealed similar outcomes when comparing TR assessments with regular physical therapy for patients with MSK (24). Another research reported that a four-week TR session yielded significant improvements in several outcomes among patients with low back pain, such as pain, muscular strength, and functional capacity (25). These results extend beyond rehabilitation patients, as phone-based telecare reduced hospital admissions among patients complaining of heart failure (26). This finding may result from patients’ improved access to specialists and lower costs of TR. However, a minority of patients expressed confidence that TR provides an equitable platform for discussing their conditions in comparison to face-to-face conversations. This result indicates the need to explore reasons that people prefer physical contact for rehabilitation. Moreover, the impact of education and/or experience on changing this belief remains unknown. A previous study found that one-third of patients expressed uncertainty about the benefits of therapeutic exercises for OA despite their prominence in OA treatment (27).
This study found that TR may represent the most convenient method of rehabilitation, especially during COVID-19, as most participants appreciated the ability to remain at home. Most participants deemed TR as an appropriate, useful, effective, affordable, and safe treatment method during COVID-19. Most respondents also believed that treatment prescribed via TR improved their health conditions. Finally, most patients expressed their desire to recommend TR to their friends, thus indicating high satisfaction levels with TR during COVID-19.
Participants’ positive opinions and experiences may partially result from the high percentage of patients (83%) who did not experience any technical problems during TR. This result may reflect the accelerating digital transformation in Saudi Arabia (28). As studies from other countries (12,19) reported that patients express concerns about technology. To resolve this issue, therapists can potentially combine TR with in-person services.
This study found that most patients in Saudi Arabia confidently used and accessed the internet via smartphones, concurring with previous research in which all participants had a mobile phone (11). In the present study, among the 17.2% of the participants who reported technical problems during TR, the majority experienced difficulties with software (38%), followed by impaired internet signals or connection interruptions (28%), audio and/or visual problems (24%), and communication difficulties with therapists (10%). Such findings may result from patients’ cognitive, motor, or social impairments, as individuals with neurological issues may struggle to use technology and communication devices. However, TR services still require more research with clinical outcome measurements using longitudinal observational studies and randomized clinical trials.
This current study constitutes the first investigation to examine the association between age and other factors associated with TR. Among all cohorts, the 0–14 age group demonstrated the greatest likelihood of facing technical problems, which may relate to difficulties that caregivers/parents face while managing children and dealing with technologies, indicating the need for improved understanding of therapists’ instructions. Finally, the confidence in using electronic devices was not an issue among all age categories except patients aged 61 years or older who appeared to be less confident. This may be justified by the Digital Transformation that has been accelerated in Saudi Arabia (28), as it was mentioned earlier in this section.
Among all age groups, parents/caregivers of patients aged 0–14 years most often expressed their belief that therapists could monitor health conditions over phone and/or video conferencing. This finding may encourage professionals to use TR for patients aged 14 years old and younger. Conversely, patients aged 15–24 years had the greatest likelihood of disagreeing with this statement, which may indicate the need to provide education about TR and its impact on this age group.
This study constituted the first investigation to examine associations between treatment type and other factors related to TR. Among all therapy types, patients receiving neurological (Adult / Paediatric) rehabilitation had a greater likelihood of agreeing that therapists possessed a strong understanding of health conditions through TR and could remotely monitor health conditions. Although such cases may suffer from complicated cognitive and motor disorders, this finding provides promise for the possibility of using TR in such cases; however, additional studies with larger sample sizes need to confirm such findings.
Future Recommendations and Limitations
This study used a non-probability sampling technique. It was not feasible to draw a random probability-based sample of the population due to the pandemic time and cost considerations. However, researchers reduced selection bias by contacting all patients treated via TR during the study period. Another limitation concerns the small sample size. This limitation may have been the reason behind the high proportion of females and patients with MSK. Therefore, there is a need for future studies to target more males and non-MSK patients. However, the patients’ female-to-male ratio at the Medical Rehabilitation Department is 65%–35%, which might have caused the high proportion of female participation in this study
Conclusion
This study revealed high levels of acceptance and satisfaction with TR services, including confidence in therapists’ understanding of patients’ health conditions as well as ability to assess and treat. The age of patients and type of treatment play a prominent role in patients’ perceptions toward using TR. Lastly, patients indicated their preference for TR during COVID-19. Additional studies should confirm findings with complicated neurological cases and include more rehabilitation departments throughout Saudi Arabia.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221130820 - Supplemental material for Tele-Rehabilitation Service from the Patient's Perspective: A Cross-Sectional Study
Supplemental material, sj-docx-1-jpx-10.1177_23743735221130820 for Tele-Rehabilitation Service from the Patient's Perspective: A Cross-Sectional Study by Fahad Saad Algarni, Majed O Alshammari, Umkalthoum Sidimohammad, Sarah A Khayat, Abdullah Aljabbary and Abdulrahman Mohammed Altowaijri in Journal of Patient Experience
Footnotes
Acknowledgments
Algarni FS would like to extend his appreciation to the Deanship of Research, Research Centre, College of Applied Medical Sciences at King Saud University for the constructive scientific support during this study. He also thanks the Deanship of Scientific Research and RSSU at King Saud University for their technical support.
Altowaijri AM, Alshammari MO, Umkalthoum Sidimohammad, Khayat SA, ALJABBARY A extend their appreciation to the Medical Rehabilitation Department at King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia for logistically supporting the research project through allowing the use of materials, infrastructure and man power.
Authors’ Contributions
All authors contributed to conceptualization, design, planning, and interpreting results for this study. All authors read and approved the final manuscript.
Data Availability
The study data employed to support this study's findings are available from the corresponding author upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This research was approved by the Institutional Review Board of the College of Medicine at King Saud University, Riyadh, Saudi Arabia (E-20-5152).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.