
Abstract
A large academic hospital system (Allegheny Health Network) introduced inpatient electronic consultations (e-Consults) during the COVID-19 crisis. Providers were invited to complete an anonymous survey on their perceptions of e-Consults. Descriptive statistics were used to analyze Likert-scale data. Cronbach’s alpha was used to assess internal consistency. Ninety-five providers completed the survey. Requesting and consulting providers agreed that e-Consults were easy to use (100% and 96.2%, respectively). Both groups also concurred that e-Consults either decreased or did not significantly impact their workload (81% and 74%, respectively) and that training was appropriate (77.8% and 86.8%, respectively). The advantage and barrier selected most frequently by specialists was “timelier completion of the consult versus in-person” and “inadequate information to complete the consult,” respectively. The disadvantage selected most frequently by requesting physicians was “lack of communication between providers.” Open-ended comments were categorized into themes. Concerns were raised regarding whether provider–provider communication via this platform offered enough information to make recommendations compared to traditional encounters. The perceived benefits and barriers of e-Consults should be further explored with the goal of improving patient care delivery and provider satisfaction.
Introduction
Never before has our health care system seen more compelling empirical evidence of the value of telemedicine than in the midst of the novel coronavirus disease 2019 (COVID-19) pandemic.
The mission of telemedicine has always been in part to break down geographic barriers and improve access to primary and specialty services. Prior to the pandemic, a strict regulatory environment and limited reimbursement models left the promise of telehealth largely unfulfilled (1). Telemedicine remained peripheral to routine clinical practice despite its ascent in specific care settings, including decision support in trauma care, treatment of low-acuity or episodic conditions, and chronic disease management (2 –4). In 2019, physician adoption of remote care stood at 28%. Only 1 in 3 specialists felt that telemedicine had the potential to enhance their practice, while only 8% of patients had received virtual care (5,6).
The rapid onset of COVID-19 has propelled a paradigm shift in the urgency to virtualize health care delivery. Financial and regulatory barriers were lowered over a matter of weeks to enable nonvisit delivery pathways that would support continuity of care while scaling hospital capacity. Geographic and originating site restrictions for Medicare reimbursement were waived and insurers expanded coverage to ensure reimbursement parity for virtual visits (7,8). Further expanding access, the US Department of Health and Human Services waived regulations allowing telehealth to be delivered over non-Health Insurance Portability and Accountability Act compliant applications (9). Before the advent of the pandemic, fee-for-service Medicare beneficiaries participated in 13,000 telemedicine services a week, but by the last week of April 2020, this number reached 1.3 million (10).
As telemedicine continues to grow and provide access to care during the COVID-19 pandemic, assessing the limitations and possibilities that surface during this critical period will have important implications for potential future adoption of a novel standard of care. In response to this public health emergency, the ensuing literature on the role of telemedicine has largely focused on either developing infrastructure or trends related to this rapid transition (11,12). However, little data on provider perspectives has been collected and probed.
The objective of this study was to obtain feedback from health care providers (HCPs) in diverse subspecialties regarding their perception of e-Consults, including advantages, disadvantages, and concerns related to this modality of telemedicine. A survey was done as part of a quality improvement effort to capture HCP perspectives regarding the training, implementation, and ongoing use of e-Consults at a large academic hospital system in Pittsburgh (Allegheny Health Network [AHN]) during the COVID-19 pandemic. Addressing providers’ concerns regarding this transition will help ensure that all facets of patient care during consultative services are met. Critically, obtaining insight into the expectations and experiences of HCPs will pave the path for long-term health care delivery in the post-pandemic clinical landscape.
Methods
Setting and Context
Allegheny Health Network is a multifacility academic health care system in the Western Pennsylvania region. It is connected on a single electronic health record (EHR) system (Epic, Verona, WI). Telemedicine has been available at AHN since 2011, primarily through a Telestroke program that delivers specialized stroke care to regional affiliated hospitals and satellite clinics.
Electronic consultations (e-Consults) in our hospital system are asynchronous provider-to-provider communications within the shared EHR. During the e-Consult process, the consultant reviews the patient’s electronic record rather than obtaining information directly from the patient. Medical history and examination findings are gathered from data in the patient’s chart which has been documented by the primary team and other consultants (who may or may not have seen the patient physically). Once the consulting provider reviews the chart, the consult note, including recommendations, is entered into the electronic chart and incorporated into the patient’s health record. The requesting provider has the option to have a face-to-face consultation or an e-consultation, with the flexibility to swap based on mutual agreement between the requesting and consulting provider.
In March 2020, as the risk of COVID-19 transmission increased, e-Consults were implemented to improve access to specialty expertise for patients and providers without the need for a face-to-face visit. This change was made to minimize the use of personal protective equipment (PPE), maintain social distancing, and potentially decrease risk of infection transmission. The health system’s Director of Informatics & Operational Excellence, together with the Medical Director of Inpatient Informatics/IT Officer, were responsible for creating e-Consult training materials. These materials were administered at a division directors’ meeting, at which time directors were instructed to disseminate these communications to their departments over a week-long period. Communications included (a) a video which captured the workflow of ordering and responding to an e-Consult request; (b) a memo with step-by-step instructions on how to include appropriate charges; and (c) a note template with smart phrases to meet billing requirements. Providers were also directed to the Telemedicine Inpatient & Emergency Department intranet site for additional information to review, and were encouraged to receive support from the IT officer who developed the e-Consult tools.
Two months after e-Consults were implemented, a quality improvement initiative was conducted in 7 hospitals across the greater Pittsburgh area to assess providers’ experience delivering telehealth via e-Consults. Surveys were distributed to the division heads of 16 specialties who were invited to share them with fellows, attending physicians, and advanced practice providers (APPs). Respondents fell into 1 of 3 categories: providers who requested subspecialist consultation using EPIC inpatient e-Consult (requesting providers), providers who received and responded to these requests (consulting providers), or providers who had done both. Surveys remained open from May 26 through June 5, 2020. The institutional review board granted quality improvement designation to this project.
An online anonymous and voluntary survey was created using the survey development tool SurveyMonkey® and included 19 individual questions. Of those, (a) 5 questions were used to gather general information about respondents—division affiliation, provider type, facility of primary practice in the network, and whether they had requested or provided an inpatient e-Consult; (b) 5 questions were based on a Likert scale rating and 2 were Likert-type questions (Table 1); (c) 2 were open-ended questions to assess the appropriateness of the training process and suggestions to improve; and (d) 4 questions were focused on assessing the advantages of and barriers to e-Consults. Another question inquired as to whether subspecialists request a face-to-face reviews more often than e-Consults.
Descriptive Statistics for Likert Scale Scores.a

a Clinicians’ attitudes related to inpatient e-Consult through EPIC from the perspective of both requesting physicians and consulting physicians. Table 1 shows that, using a cutoff point of half-way up the mean satisfaction score (1.5) on all questions, the survey indicated satisfaction, which is confirmed by the median and mode scores all > 2.
Statistical Methods
The survey data were analyzed in an exploratory and descriptive manner to gain insight into the use of remote consultation and telemedicine in the inpatient setting. The 5 Likert scale questions measuring agreement were scored on a 4-point Likert scale (eg, 3 = strongly agree, 2 = agree, 1 = disagree, 0 = strongly disagree). The 2 Likert-type questions were statements for evaluation, but were also rated on a 4-point scale. For analyses, the order of some 4-point Likert scale items was reversed to give the higher scores to responses that showed a more positive impact/less negative evaluation.
For the Likert scale questions and Likert-type questions, the corresponding mean and standard deviation, median and interquartile range, mode, and 95% confidence interval for the mean were reported (Table 1). Cronbach’s alpha was used to evaluate internal consistency. Statistical analyses were done using IBM-SPSS Statistics, version 26.0 (IBM Corp., Armonk, New York).
For qualitative responses, HCP perceptions of the e-Consult service were gathered and categorized by provider type: providers who requested subspecialist consultation (requesting providers) or providers who received and responded to these requests (consulting providers). We then identified key themes from the qualitative data with regard to 4 individual satisfaction domains, as well as perceived barriers and facilitators to participating in the e-consult process. These descriptive responses are listed in Tables 2-5.
Advantages of e-Consult Use.

a Providers could give more than one response.
Advantages of e-Consult Use (Open-Ended Responses).

Abbreviations: HER, electronic health record; PPE, personal protective equipment.
Barriers to e-Consult Use.

a Providers could give more than one response.
Frequencies for e-Consult Barriers Identified in Survey by Requesting and Consulting Providers.

Abbreviations: HER, electronic health record; HPI, history of present illness.
Results
Of 96 HCPs who participated in the online Inpatient e-Consult survey, 95 were eligible for inclusion in this analysis. The majority of respondents practiced Academic Internal Medicine (26%). Among them, 74% were MD/DOs, 4% were Fellows, and 22% were APP (Table 6). Forty percent of providers reported that they had requested an inpatient e-Consult through EPIC and 60% had not. Fifty-seven percent of providers indicated that they had responded to an e-Consult request through EPIC and 43% had not. Additionally, 19% of providers had both requested and provided care through e-Consult.
Summary of e-Consult Survey Responses.
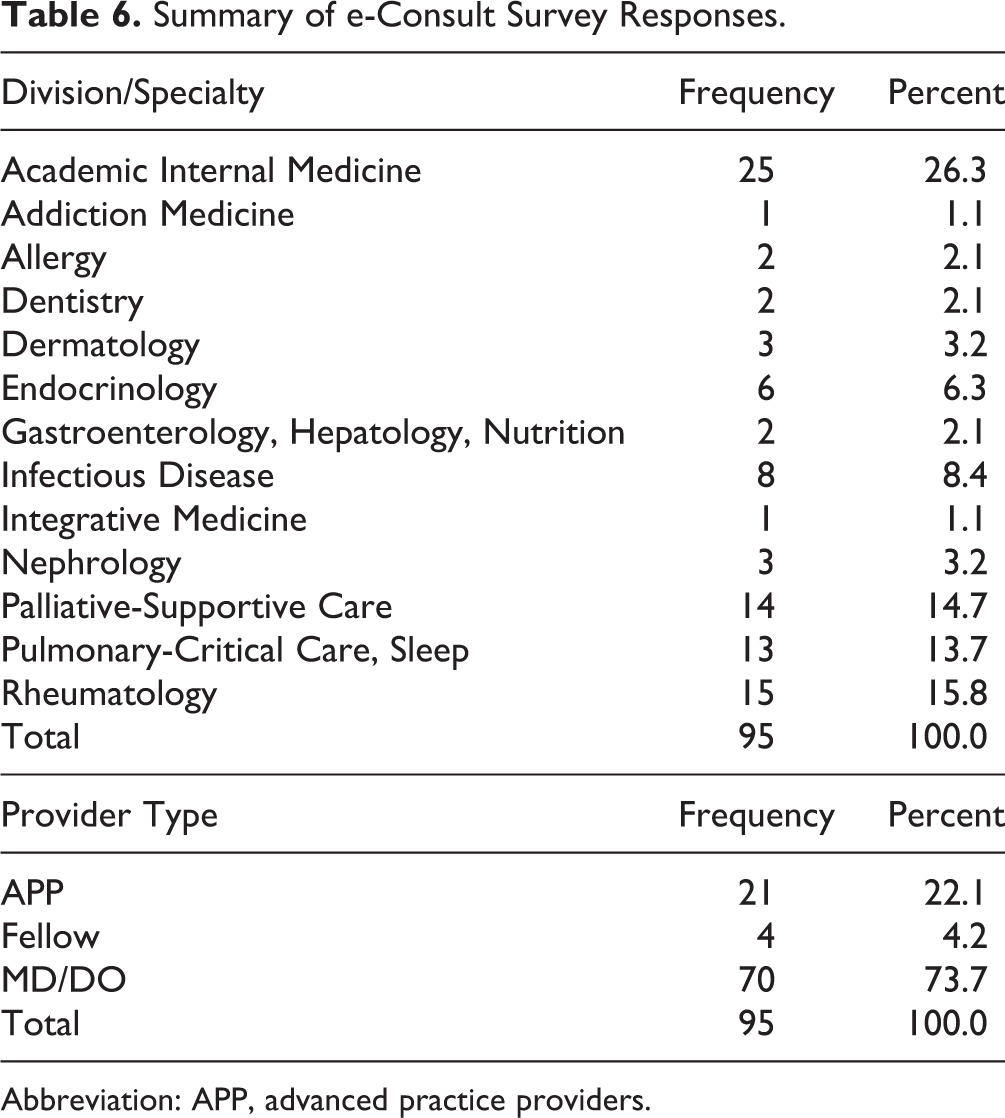
Abbreviation: APP, advanced practice providers.
For the 7 questions related to training, implementation, and ongoing use of e-Consults (Table 1), the majority of HCPs indicated satisfaction with the service. This finding was confirmed by the median and mode scores all >2, with a score of “2” indicating a positive perception of e-Consults. On the most important single question (“Overall, how satisfied are you with the Specialist e-Consult” option), the difference between those HCPs who responded being “Satisfied” or “Very Satisfied” (86.5%) with those being “Dissatisfied” or “Very Dissatisfied” (13.5%) was 73%. The margin of error was ±16.4%.
Among requesting providers, 94.7% felt that e-Consults were simple and easy to use. In terms of logistics, 75% observed that introduction of e-Consults had no significant impact on their workload whereas 19% indicated that the process increased their workload either acceptably or significantly. Additionally, 77.8% of requesting providers either strongly agreed or agreed that the training offered to them was appropriate.
Among consulting providers, 96.2% agreed or strongly agreed that the e-Consult process was simple and easy to use. In total, 74% observed that the introduction of e-Consult either decreased their workload or did not significantly impact their workload, whereas 26% responded that its introduction increased their workload either significantly or acceptably. Overall, 86.8% of consulting providers either strongly agreed or agreed that e-Consult training was appropriate.
Cronbach’s alpha was used to evaluate the internal consistency of the Likert scale/ Likert-type questions that measured agreement. This ranged from 0.651 to 0.785 across the questions (with an acceptable internal consistency of > 0.70).
When participants were asked about the advantages of using e-Consult over face-to-face consultations, multiple responses were allowed. The advantage selected most frequently by consulting physicians was “timelier completion of the consult versus in-person.” In comparison, the advantage selected most frequently by physicians requesting e-Consult was “None of the above,” suggesting that there was no one primary benefit perceived by the requesting providers. Other advantages are outlined in Tables 2 and 3.
When participants were asked about the barriers of using e-Consult compared with face-to-face consultations, multiple responses were similarly allowed. The barrier selected most frequently by consulting physicians was “inadequate information to complete the consult.” In comparison, the disadvantage selected most frequently by requesting physicians was “lack of communication between providers.” Other barriers are listed in Table 4.
Forty-four percent of the requesting providers expressed the belief that subspecialists request face-to-face review more often than they do e-Consults because of either a perceived complicated clinical scenario or discomfort with the e-Consult process in general.
Qualitative Themes
Several key themes emerged from participants’ qualitative responses: (a) issues with billing and reimbursement, (b) lack of provider–provider communication, (c) insufficient quality of work-up data available within the health record, and (d) an overall preference for in-person visits. We describe these inflection points below and provide select provider comments to further illustrate these results.
Survey results revealed that many providers’ reluctance surrounding the use of e-Consults stemmed from concerns about billing and reimbursement. Several described frustration that they were not adequately compensated for their time. As one participant explained, “billing thresholds are much lower than actual time spent performing the consult.” Another participant vocalized dissatisfaction with “dismal reimbursement.” In addition, one provider cited confusion about billing codes without having received “billing clarification and templating in advance.”
The e-Consult survey also revealed a disconnection in clinician-to-clinician communication. For example, a consulting provider associated their dissatisfaction with inter-team confusion between ordering and consulting providers: “In my experience, the primary teams expected and assumed that the consultant was speaking with the patient for obtaining the history of present illness, although technically this is not required for an e-Consult. It lead to some issues with communication.” On the other side of the e-Consult encounter, a referring provider noted that issues arose from e-Consults because roles and responsibilities were not clearly delineated, noting a need for “better agreement in advance about consultant role in ongoing communication with patients and families and documentation of communication.”
Consulting physicians often reported that the quality of information made available via a patient’s electronic record was insufficient for clinical decision-making. As one subspecialist described, “We have to rely on someone else’s visual assessment of the patient and not our own.” Another consulting provider noted that multifaceted cases cannot be reliably managed through a patient’s history alone: “Many of the patients, especially the complicated ones, need to be seen in person. The history in the chart may not answer all the questions we need from the patient.” Similarly, a referring physician agreed that simply relaying workup data to a consulting subspecialist asynchronously is “not the same information as they would have received in person by seeing the patient.”
Despite favorable views of e-Consults in general, some participants articulated a clear preference for traditional in-person visits. One consulting physician described resistance to virtual visits based on the nature of their subspecialty, citing the centrality of a physical exam: “The e-Consult is not appropriate for the pulmonary physician. I could not in good conscience do an e-Consult.” In addition, a referring physician stated: “I feel specialists are doing more e-Consults inappropriately when they should be seeing the patient.” However, several respondents pointed out that the e-Consult process is flexible, and offers the option of choosing an in-person visit if necessary. As one participant described, “Some [patients] do require in-person evaluation. But the consultant has the ability to go physically see those patients still. So I do not see a downside with having this option available when the consultant deems appropriate.”
Additional quotes regarding these themes are illustrated in Table 5.
Discussion
In the midst of the coronavirus disease 2019 crisis, it is clear that our health system has reached the tipping point for telehealth. From March to April 2020, Medicare claims data show an exponential increase in telemedicine services (13). As the prospect of in-person visits presents a lesser risk of transmission in some areas, the ongoing use of telehealth among Medicare patients indicates that interest in virtual care will endure even post-pandemic (14).
This study was conducted to analyze the adoption of e-Consult use in a large academic hospital system and summarize the lessons learned from this rapid transition necessitated by the COVID-19 pandemic. In order to ensure that all facets of patient care were met during consultative services, we sought to understand facilitators and barriers to this process from the perspective of inpatient HCPs.
Participants largely reported satisfaction with the e-Consult process in terms of ease of use and convenience. In the past, requesting providers have reported that the e-Consult process creates additional work, but this issue was not cited by our cohort, with “improved time management” as the second most frequent advantage reported by specialists (15,16). Both requesting and consulting providers concurred that e-Consults either decreased or did not significantly impact their workload. However, in terms of barriers, our analysis conveyed 4 major themes: (a) issues with billing and reimbursement, (b) lack of provider–provider communication, (c) insufficient quality of workup data available within the health record, and (d) an overall preference for in-person visits. Examining and addressing these areas of concern will help our health system and others develop a better clinical pathway to utilize e-Consults.
Although an e-Consult program represents a promising approach to the challenge of continuing care in a way that is convenient and cost-effective for patients, consulting physicians in the current study raised concerns about documentation and reimbursement. Prepandemic, many consulting physicians felt strongly that e-Consults were useful for referring providers and their patients but that reimbursement and time allotted were not adequate (17,18). Despite recent temporary regulatory changes that ensure reimbursement parity, participants expressed frustration in the belief that they were not being compensated fairly for their time. The correct way to document virtual consultations was also a source of confusion among providers in the present study. These results emphasize the value of protected time and credit for providers as well as clear industry guidelines that simplify coding and billing. In response to frequent questions regarding billing/code changes, relevant training materials were updated and redistributed throughout our system.
Our analysis captured another important trend in provider attitudes: the need for enhanced coordination between ordering and consulting teams, particularly when relaying patient information via EHR. Physicians on both sides of the e-Consult encounter expressed the belief that the process was impeded by a lack of streamlined provider-to-provider communication. The barrier selected most frequently by consulting physicians was “inadequate information to complete the consult,” while the disadvantage selected most frequently by requesting physicians was, more generally, “lack of communication between providers.” Although specialists were equally wary of answering vague consult questions before the advent of COVID, insufficient clinical information and provider input is a problem that has been emphasized during the transition to e-Consult use during the pandemic (19,20). These concerns highlight the importance of improving the clarity of documented clinical questions and the quality of work-up information made available to reviewers. Communication-based training could also be an important step in enhancing the delivery of virtual care, with the end goal of creating data that is both accurate and sufficiently detailed.
Several providers also noted their preference for conventional consultations even during the current transition to remote health care. Both requesting and consulting providers indicated that some complicated clinical situations clearly warrant an in-person visit. In a recent specialty-specific study, a survey of neuro-ophthalmologists gauging adoption of telehealth during the pandemic highlighted examination limitations and data quality as key concerns, particularly in pursuit of a diagnosis, whereas visits relying on history or external examination were deemed more appropriate for this mode of telemedicine (21). While telehealth has proven its efficacy in terms of remote monitoring of chronic conditions, digital care is less feasible in yielding challenging diagnoses (22). Knowing that historically, having to convert consultations into face-to-face visits is a source of dissatisfaction with the e-Consult process, a better understanding of which cases are appropriate for electronic consultation is needed (20). Ideally, a streamlined e-Consult system will allow providers to intelligently triage every referral with a professional review.
Moreover, the open-ended portion of the survey revealed an unanticipated barrier to e-Consult implementation: a perceived lack of clarity surrounding expectations. Although training materials stated that the e-Consult platform facilitated recommendations made purely by chart review, some health care workers were under the impression that they were expected to speak with the patient over the phone to obtain a medical history. It is likely that this miscommunication is situational, related to the remarkably rapid implementation of virtual care during the pandemic. Reiterating the purpose and objectives of e-Consults via iterative follow-up communication with HCPs helped clarify expectations and ultimately promote adoption of virtual consultations. Additionally, several providers noted discomfort with the e-Consult process despite its ease of use. As reported here, the source of this unease may be related to the restricted nature to one-on-one patient–provider relationships inherent in digital consultations, which can create a feeling of inadequacy in patient care.
This study has several limitations due to the post hoc nature of analysis in the context of the current pandemic. Because of the rapidly evolving nature of COVID-19, the survey was not pilot-tested. The survey sample was not randomly selected and therefore may be biased by “self-selection.” The total number of online surveys sent out to health care providers and the total number of provider types receiving the survey is uncertain, and as a result, the exact survey’s response rate cannot be calculated. No demographic data (eg, age, gender, race, and ethnicity) was collected to determine whether any significant differences in survey respondents existed.
Lastly, a 4-point Likert scale was used in this survey. This scale excludes a neutral midpoint and may force a respondent into expressing agreement or disagreement when they may have no clear opinion which may distort survey results.
Conclusion
COVID-19 has driven exponential growth in awareness and utilization of telehealth. This case study demonstrates the rapid upscale of e-Consult services at a large academic hospital system during the COVID-19 pandemic and provides insight into provider expectations for integrating digital technology into routine practice. Important themes surrounding e-Consults emerged from this project. The perceived benefits and barriers of e-Consults reported here may be beneficial to other health systems seeking to adopt this modality of telemedicine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.