
Abstract
Patient activation is the product of knowledge, skills, and confidence that enables a person to manage their own healthcare. It is associated with healthy behaviors and improved patient outcomes. We surveyed prevalent hemodialysis (HD) patients at 10 centers using the Patient Activation Measure 13-item instrument (PAM-13). Activation was reported as scores (0-100) and corresponding levels (1-4). Of 1149 eligible patients, surveys were completed by 925 patients (92% response rate). Mean age was 62 ± 14 years, 40% were female, median vintage was 41 (IQR 19-77) months, and 66% had diabetes. Mean PAM score was 56 ± 13, with 14%, 50%, 25%, and 10% in levels 1 to 4, respectively. In adjusted analysis, older age and having diabetes were associated with lower activation, whereas higher educational levels and female gender were associated with higher scores. Significant variation in activation was observed among participants from different centers even after adjustment for other variables. In conclusion, low activation is common among prevalent HD patients.
Keywords
Introduction
Despite refinements over the last few decades, dialysis care remains a high-cost therapy with suboptimal outcomes. In particular, center hemodialysis (HD) requires costly resources as it consists of people requiring specialist health care for 4 h, 3 times per week. Redesigning this care in a way that is driven by the patient is key to decreasing costs and delivering value-based healthcare (1). Patient driven health care requires patients to be ready, willing and able to manage their own health and healthcare. Patient activation is a construct that measures the knowledge, skills and confidence required to self-manage and has been strongly associated with improved health outcomes (2).
Patient activation has been added as a quality metric in the US Centers for Medicare and Medicaid Services (CMS) Kidney Care Choices model. This model has been implemented to delay the onset of dialysis and to incentivize kidney transplantation (3). Patient activation has been included because of the belief that increased self-management in kidney care patients will contribute to these aims. Thus, there has been an increase in interest in the concept of activation in people with kidney disease by US dialysis providers, funders, clinicians, and patients (4).
Patient activation has been used along with other important concepts such as health literacy, health confidence, and self-efficacy to describe health promoting actions. Patient activation differs from the traditional measurement of health literacy because health literacy has been traditionally conceptualized as a knowledge and skills-based concept used to maintain health through self-management (5), whereas the measurement of patient activation includes confidence, beliefs, and role expectations. Subsequently, patient activation has been found to be a stronger predictor of behaviors and health outcomes than health literacy (6). Health confidence is an easily measured effective proxy for engagement. However, patient activation specifically identifies knowledge, motivation, and skills domains in addition to confidence (7). Patient activation differs from self-efficacy in that activation is not disease- or condition-specific (8), whereas self-efficacy refers to a person’s confidence to carry out specific behaviors to control a specific health condition (9).
Patient activation has been studied extensively in other chronic conditions (10–23). Highly activated patients adopt healthier lifestyles and behaviors, are more adherent to medications (24), have fewer problems with care coordination (10, 25), know how to make use of available services (20), have fewer unplanned emergency room visits (26, 27), lower hospitalization rates (18, 20), and have a more positive experience with their providers (25, 28).
In the dialysis domain, studies from outside the United States revealed that patient activation was low among prevalent HD patients (29–32). There are few studies on patient activation in dialysis patients from the United States. One recent study of 175 HD patients reported the correlation of lower PAM scores with lower levels health literacy and higher levels of depression and anxiety, with no association with treatment adherence (33). This study highlighted the importance for more studies to discern the validity and reliability of the PAM-13 in the United States dialysis context. The United States has significant differences in patient populations and healthcare systems than other nations. In particular, the US multiple payer system contributes to the world’s most expensive healthcare system compared to the single payer universal healthcare systems in comparable countries. The 750 000 people who live with kidney failure are 1% of the US Medicare population but account for roughly 7% of the Medicare budget. One contributor to this is the low self-care and home dialysis rates in United States reflecting a culture of low activation. Given the high costs and high activity, further evaluation of the self-care and status of patient activation among prevalent dialysis patients in the US healthcare system is required to address the low self-care prevalence.
Increased evidenced-based knowledge to increase our understanding of patient activation measure related to dialysis is necessary in, and for the planning and development of, interventions to improve delivery of self-care leading to more uptake of home dialysis modalities and transplantation. In this study, we aimed to explore the status and correlates of activation among prevalent HD patients in the United States.
Materials and Methods
Settings and Study Population
We conducted a cross-sectional survey using the validated PAM-13 instrument (US English and US Spanish language versions). The survey is comprised of 13 questions (34) with additional demographic information collected from the provider’s electronic medical records database. The study complies with the STROBE Checklist for observational cross-sectional studies (35) (Supplemental Table 1).
We targeted a convenience sample of 10 HD centers, spread across California, Texas, and Tennessee, representative of the geographic distribution of centers under the management of a non-profit dialysis organization. All patients at participating centers, 18 years or older and receiving HD for at least 3 months (prevalent HD patients) were included in the study. Individuals were excluded if they were unable to understand English or Spanish, unable to complete the survey as assessed by dialysis staff because of cognitive impairment or an active psychological condition, participating in a competing study, in a self-care program, or were receiving in-center nocturnal HD or temporary dialysis. The survey was conducted between November 2019 and March 2020. Trained research coordinators, who underwent PAM-13 training from the licensed PAM-13 providers (36), invited patients in person during dialysis at participating centers to participate in the study by completing the survey. Waiver of consent was sought because of the risk of biasing the sample if patients with low activation chose not to participate and on the bases of low risk to participants. Ethical approval, including the granting of a waiver of consent, was conducted and approved by Aspire Independent Review Board (Protocol Reference Number 520190129).
Baseline Socio-Demographic and Clinical Characteristics
Patient socio-demographics and clinical characteristics were extracted from the dialysis provider’s electronic health record system. Socio-demographic characteristics collected were age, gender, race, ethnicity, and educational level. Clinical characteristics collected were dialysis vintage (months on dialysis), primary cause of kidney disease, and co-morbid conditions.
Patient Activation Measure
The PAM-13 survey instrument is a 13-item, with 4 response options for each item in a Likert scale from strongly disagree to strongly agree with no neutral option. A fifth, not applicable response, is also offered. The instrument measures 4 constructs: (1) the belief that active role is important (items 1, 2); (2) the level of confidence and knowledge to take action (items 3-8); (3) the ability to take action (items 9-11), and (4) the ability to stay the course under stress (items 12-13). The final score is a score from 0 to 100, with higher scores indicating higher activation (37).
Scores correspond to 4 levels, 1 to 4: Level 1 (score 0-47.0) indicating not believing activation is important, Level 2 (47.1-55.1) indicating a lack of confidence and knowledge to take action; Level 3 (55.2-72.4) indicating beginning to take action, and Level 4 (72.5-100) indicating already taking action.
Surveyors explained the study and the survey to patients and obtained verbal consent prior to completing the survey. Hard copy paper surveys were provided to patients by researchers whilst patients were receiving dialysis. Assistance to complete the questionnaire was offered to participants, adhering strictly to the PAM-13 instruction guide (36), with each PAM question read exactly as it appeared on the survey.
Statistical Analyses
Socio-demographic and clinical characteristics were reported as counts and proportions for categorical variables, and means and standard deviations (SD) or medians and interquartile ranges (IQR) for continuous variables. Analysis of variance (ANOVA) was used to test the significance of score differences in the following subgroups, based on subject matter experts and previously published literature (4). The sub-groups were age groups (less than 55 years, 55 to less than 65 years, 65 to less than 75 years, and 75 years or older), female gender (vs male), Black race (vs non-Black), Hispanic/Latinx ethnicity (vs non-Hispanic, non-Latinx), diabetes mellitus (vs no diabetes), presence versus absence of comorbid conditions (diabetes, hypertension, cardiac disease, cerebrovascular disease, and peripheral vascular disease), educational level (less than high school, high school, and college or trade school graduate), and dialysis center assignment (the dialysis center with largest number of participants was chosen as reference group for this variable). The significance of differences in distribution of PAM levels among subgroups was tested using the Chi square test.
Linear regression analyses were conducted to examine the association of activation scores as a dependent variable with variables that were found to have an association with PAM scores in the ANOVA analysis with a P value of less than 0.15 were included as independent variables.
Statistical analyses were conducted using R version 4.0.0 (The R Foundation for Statistical Computing).
Results
Out of 1374 individuals receiving dialysis at the 10 participating centers, there were 1149 eligible patients (198 patients ineligible). Of those, 142 were not available to survey. Research coordinators invited 1007 patients to participate. A total of 925 individuals completed the survey (82 declined; 92% response rate). All surveys generated complete responses, and none were excluded. The median number of participants from a center was 84 patients (IQR: 72-108). The sample comprised a large proportion of participants from California centers (63%), with smaller proportions from Texas (29%) and Tennessee (8%). A breakdown of reasons for ineligibility and unavailability is included in the study flow diagram (Figure 1).
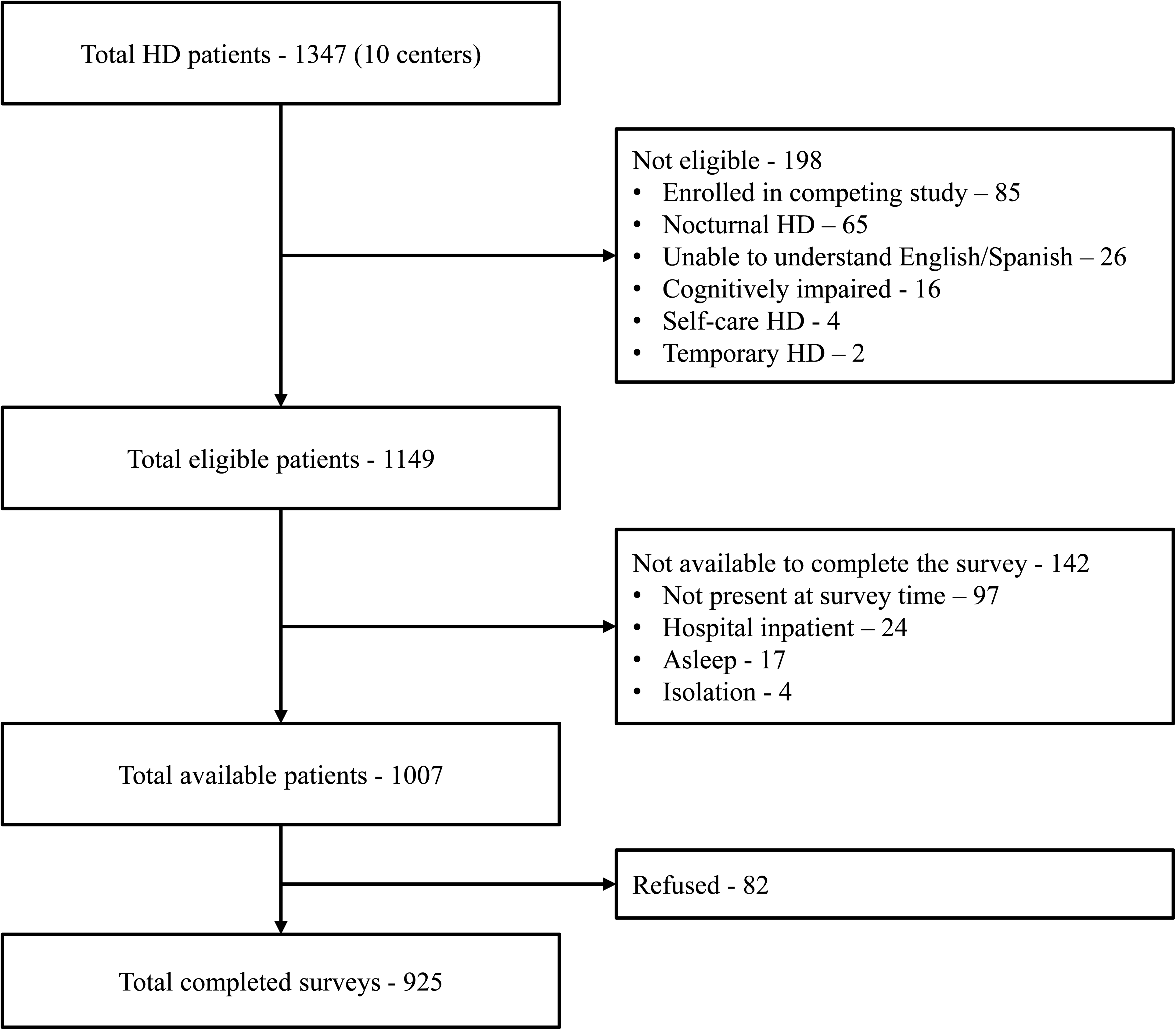
Participant flow chart.
The mean age of survey participants was 62 ± 14 years, and 40% of respondents were female. Black race comprised 22% of the sample, while about half the participants (47%) identified their ethnicity as Hispanic or Latinx. The median dialysis vintage was 41 months (IQR 19-77). The main comorbid conditions reported were hypertension (89%), diabetes (66%), and cardiac disease (30%). The proportion of participants who completed college or trade school, completed high school, or had less than high school education was 24%, 41%, and 34%, respectively. Table 1 details the breakdown of the sample by subgroups of socio-demographic and clinical variables.
Participant Characteristics (n = 925).

Abbreviations: SD, standard deviation; IQR, interquartile range; ESKD, end-stage kidney disease.
Patient Activation Among Prevalent HD Patients
The mean PAM score of study participants was 56 ± 13, with 14%, 50%, 25%, and 10% in levels 1 to 4, respectively. Significantly higher PAM scores were observed among younger participants, Blacks, non-Hispanic, or Latinx, and those with higher levels of education, while significantly lower PAM scores were observed among those with diabetes or cardiac disease. PAM scores varied significantly between participants from different centers. Subgroup distribution of PAM scores and PAM levels are shown in Table 2 and Figure 2, respectively.

Patient activation levels among prevalent hemodialysis patients—overall and subgroup distributions.
Patient Activation Scores in Prevalent Hemodialysis Patients (n = 925).

* P-value from ANOVA test.
Variables Associated With Patient Activation Scores
Table 3 shows results of linear regression of examined socio-demographic and clinical variables with PAM scores. In unadjusted and adjusted analyses, older age and having diabetes were associated with lower activation scores, while higher levels of education were associated with higher scores. Female gender was associated with higher scores only after adjustment for other covariates. The unadjusted association of scores with race, ethnicity, and cardiac disease disappeared in the adjusted analysis. Significant variation in activation scores were observed between participants from different centers, and these remained significant in the adjusted analysis.
Linear Regression Analysis.

Discussion
This is the largest study to date to focus on the status of activation among prevalent HD patients in the United States. More than two-thirds of participants were found to have low activation levels (combined levels of 1 and 2). This finding underscores an opportunity to modify management of patients based on their activation levels and to adopt strategies to improve patient activation among this group of highly medicalized patients.
We report a larger proportion of patients with low activation levels than a recent US study who reported only 37% of dialysis patients in levels 1 and 2 (33) compared to 64% of patients with low activation levels (levels 1 and 2) in our study. Potential differences may be explained by our waiver of consent which assisted in a high response rate (92%) and potentially less biased sample. It is possible that our larger ethnic variations and low education levels may explain these lower activation levels, stimulating the question of the importance of different individual patient characteristics when addressing patient activation and self-management.
The mean activation score reported in prior non-US studies ranged between 51 and 56 (29–32), and the proportion of HD patients with low activation (levels 1 and 2) was 73% and 53% in studies from Belgium and England, respectively (29, 30). Importantly, these studies were all performed in universal healthcare systems that are vastly different from the US healthcare model. The only study from the US included 19 HD patients among a total population of 84 patients with chronic kidney disease. This study did not report activation scores or levels for the subgroup on HD, but reported that patients with more advanced kidney disease had lower activation (38).
The high prevalence of low activation may be a reflection of the nature of delivery of in-center HD care, which is optimized for rapid turn-over of patients between shifts, focusing on care delivered by staff, with the patient being a passive recipient of care (39, 40). Given the upcoming introduction of the PAM-13 CMS reimbursement-related metric (4), the challenge for US providers is to apply activation-increasing interventions to contribute to improved health outcomes for people with kidney disease. Although the Kidney Care Choices models aim to increase self-care and home dialysis, the realities of high patient-to-staff ratios, expected efficient dialysis chair usage, and increasing patient co-morbidity present a challenge to support HD patients’ activation. Suggestions that higher patient activation increases adherence (41) and improves intradialytic volume management (42) are yet to be proven.
We found that older age was associated with lower activation. This was consistent with findings from other studies (29–31), and maybe related to older patients having lower confidence in maintaining health behaviors or being more adept to paternalistic medicine (30, 43). Diabetes mellitus was a common comorbidity and the most frequent cause of primary kidney disease in our population. Presence of diabetes was associated with lower PAM scores. This finding is likely to be related to the prolonged nature of illness, multiple complications associated with diabetes, and the demand it brings on the patient for self-management (11, 44). The finding that higher education was associated with activation was expected given that knowledge, skills, and confidence are likely promoted through advanced education (19). In the adjusted analysis, female gender was associated with higher PAM scores. This is consistent with the observed differences between men and women in seeking medical advice, following preventive actions and general health behaviors (45, 46), and their behavior changes in response to education (47).
Significant variations in activation scores were observed between participants from different centers. These remained significant following adjustment for other variables, indicating the presence of unmeasured factors contributing to activation. All participating centers had the same protocols and were under management of one organization, with similar staff-to-patient ratios, and all were located in urban areas. We could not readily identify any factors that may have contributed to this variability. Further investigation of patient-related factors, the associations between patient activation and HD center practice patterns, health access, system and policy variables are highly recommended for future studies.
Obtaining patient activation scores on patients can be utilized in multiple ways. Patients with low activation are high-risk patients in need for more surveillance and need an integrated approach to improve their activation. To influence a meaningful and sustainable change in dialysis care that improves patient activation, we will need an integrated approach that involves people on dialysis, their healthcare team, dialysis providers, and policy makers (48, 49). Interventions that can be considered include health coaching, peer mentoring, and involving patients more in their dialysis care (50–53). It is likely that one isolated specific individual strategy may not be sufficient to increase patient activation with a combination of the following strategies required. A combination of individualized care plans; scenario-based education, health coaching with motivational interviewing; goal setting with a systematic follow up to assist patients to improve the skills to maintain life changes needed and handle health-related complications; and tailored coaching by peers to help patients building confidence in how to follow healthcare recommendations may increase patient activation (54).
This study has several limitations and strengths. Limitations include the observational, cross-sectional design, which does not permit investigations concerning causality or changes over time. To improve the response rate, we limited the survey size and the number of variables we collected from patients, including patient level socioeconomic status, health access variables and health system variables and did not collect demographic and clinical characteristics of refusals. These limitations are counterbalanced by several strengths. This is the first large cohort US study to measure patient activation in a large cohort from English- and Spanish-speaking patients. Although center selection was by convenience sampling, it included 10 centers from 3 states. To limit selection bias, we targeted (and achieved) a high response rate.
In conclusion, we found that patient activation, the measure of knowledge, skills, and confidence that enable a person to manage their own healthcare, was low in a large proportion of individuals receiving in-center HD. Older age and having diabetes were associated with lower activation, whereas female sex and having higher educational levels were associated with higher activation. Further research is required to understand center-related activation factors, trajectories of activation over time, and the effectiveness of tailored patient activation interventions on health-related and patient-related outcome measures.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221112220 - Supplemental material for Patient Activation Among Prevalent Hemodialysis Patients: An Observational Cross-Sectional Study
Supplemental material, sj-docx-1-jpx-10.1177_23743735221112220 for Patient Activation Among Prevalent Hemodialysis Patients: An Observational Cross-Sectional Study by Wael F Hussein, Paul N Bennett, Sumi J Sun, Marc Reiterman, Emily Watson, Ian M Farwell and Brigitte Schiller in Journal of Patient Experience
Footnotes
Acknowledgments
We would like to thank the patients and staff at the participating centers. We wish to thank Jug Atwal for the study management, and survey coordinators Sara Oliver and Anna Carrasco.
Author Contributions
Study idea and design: WH, PB, SS, BS. Data collection and oversight: WH. Data processing and analysis: MR, SS, WH. Interpretation of the data: WH, PB, EW, SS, IF, BS. Manuscript writing: WH, PB. Final development and approval of the manuscript: all authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.