
Abstract
There is little information on patients’ medication adherence experiences at community-based clinics in Ghana. This study investigated adherence to antiretroviral medication among people living with HIV (PLHIV) attending a community-based HIV clinic. PLHIV (N = 349) completed a questionnaire battery on medication adherence, doctor–patient communication, HIV stigma, patient general self-efficacy, perceived social support, and on patient spirituality. Linear Regression was used to analyze the data. Results showed that doctor–patient communication (β = .38, 95% CI [0.09, 0.18], P <.001) and social support from significant others (β = .46, 95% CI [0.18, 0.67], P <.001) were positively associated with medication adherence in this sample. In contrast, HIV stigma (β = –.16, 95% CI [–0.58, −0.09], P <.01), patient spirituality (β = –.22, 95% CI [–0.44, −0.00], P <.05), and patient general self-efficacy (β = –.14, 95% CI [–0.17, −0.02], P <.01) were negatively associated with medication adherence. There is a need for educational interventions targeted at enhancing doctor–patient communication and social support while reducing stigma among PLHIV in Ghana.
Introduction
Adherence to antiretroviral therapy (ART) is crucial to HIV/AIDS clinical care outcomes. Antiretroviral drugs (ARVs) are known to have decreased disability, death, and transmissibility of HIV in people living with HIV (1–3). Ghana has a generalized HIV status (ie, most new HIV infections are primarily among the general population). There were about 350 000 adults and children living with HIV as of 2020 in Ghana, with new HIV infections among adults, youths, and children in 2020 alone reaching 19 000 (4). Of this number, 63% of adults aged 15 years and older were receiving antiretroviral therapy as at 2020. As part of efforts to reduce mortality rates among people living with HIV (PLHIV), Ghana has adopted and is implementing the option B + (ie, lifelong ARV treatment irrespective of the patient's CD4 count) and the new 95-95-95 HIV target which requires that 95% of individuals with HIV know their status, 95% of the HIV-infected be placed on ARVs, and 95% of those on ARVs should achieve viral suppression by the year 2030 (5,6). Ghana's HIV response also aligns well with the African Union's Agenda 2063 health strategy, aimed at ending AIDS by 2030 and at strengthening healthcare systems (7,8). Implementation of the lifelong ARV treatment and the 95-95-95 target has driven a scale-up of ART medication in Ghana (4,9). Despite this, there is less than optimal adherence to ART in PLHIV in Ghana (10,11).
Numerous studies have reported on positive associations between adherence to ARVs and improved quality of life of PLHIV (12,13), decrease in the incidence of opportunistic infections (14), decrease in hospital readmissions, (15) and decrease in treatment cost (16).
Available ART adherence research in Ghana has largely been conducted at hospitals in urban townships. Data from HIV patients recruited in the Upper West Regional Hospital, Ghana found overall lifetime ART adherence to be 62.2% (17). The authors observed that adherence was positively associated with immunological success whereas nonadherence was associated with immunological failure. Other work among PLHIV who accessed HIV services at the Cape Coast Teaching Hospital reported that most patients complained of waiting time and financial cost (18). A study among PLHIV attending antiretroviral clinics at Kintampo and Techiman South Municipalities, Ghana, found that transportation cost was an important factor preventing HIV patients from accessing ART treatment (19). ART adherence research among 384 HIV patients at Oti and Volta regional hospitals, Ghana, reported that only 26% experienced viral load suppression (10). The researchers noted that most patients expressed dissatisfaction with the length of time spent with the health provider.
There is, however, limited ART adherence research in rural communities in Ghana.
Information on ART adherence in rural Ghana can help tailor healthcare to improve clinical outcomes in HIV-infected persons. Systematic reviews have demonstrated that community-based ART programs are effective in scaling up adherence in sub-Saharan Africa (20,21). The reviews have shown that community-based ART delivery services can have the potential to make treatment more accessible and affordable, decongest metropolitan and municipal health facilities, improve ART coverage, and to boost the retention of patients on ART. Relatedly, other researchers, working independently, found strong evidence suggesting that decentralization and task-shifting are effective strategies in ART delivery services (22,23). Consequently, there is a need for ART programs in Ghana to expand to rural communities to enhance access and retention. Community-based HIV care services can strengthen Ghana's health care system by reducing the inflow of community dwellers seeking HIV care in urban hospitals. Understanding barriers to and facilitators of ART adherence for community-based clinics in rural Ghana can provide useful information for the design of targeted interventions for rural community settings. The aim of the present study was to examine factors associated with ART adherence at a community-based HIV clinic in Ghana.
Method
Study Design
This study used a cross-sectional survey design.
Study Setting
The study was conducted at Agogo township in the Asante Akim North District in the Ashanti Region. The District is home to about 85 788 people with 48.96% and 51.04% being males and females, respectively (24). The District has a youthful population with more than half (50.6%) below 20 years of age. About half of the population lives in rural communities. The major occupations of the people are agriculture, forestry, sales, and service work, with approximately 72% of inhabitants being self-employed. The District has a literacy rate of 79.2% among inhabitants aged 11 years and older (25).
Participants
A total of 349 participants (n = 173, male; n = 176, female) aged between 18 and 45 years old provided data for the current analysis.
Recruitment and Patient Consent
Participants were recruited at a community HIV clinic at Agogo, under the management and supervision of the Agogo Presbyterian Hospital. The Agogo Presbyterian Hospital is a collaborating research center for the School of Public Health, University of Ghana. The hospital is also a designated training center for housemanship (https://agogopresbyhospital.org/main/). The HIV clinic has a large number of registered patients. These characteristics facilitated the choice of this clinic for the present study. Participants were recruited using a purposive sampling technique with the help of clinic staff. Potential participants were approached by the research team at the HIV clinic.
The aims of the study were explained to them and those who showed a willingness to participate were recruited. Patients who had been diagnosed with HIV-1 and HIV-2 and were receiving highly active antiretroviral therapy (HAART) were included in the study. HAART treatment uses a combination of 3 or more drugs, sometimes referred to as combination antiretroviral therapy (cART). Some patients were on a class of ART known as non-nucleoside reverse transcriptase inhibitors (NNRTIs), whereas others were on a protease inhibitor combined with tenofovir, a nucleoside reverse transcriptase inhibitor (NRTI). A total of 378 patients were contacted but 349 provided data, indicating a response rate of 92.3%. They were briefed on steps taken to ensure their confidentiality and anonymity and were asked to sign consent forms.
The inclusion criteria included being diagnosed with HIV-1 or HIV-2, receiving ART, being 18 years of age or older, and willingness to participate in the study. The exclusion criteria included being diagnosed with HIV co-infection (co-morbidity), not being in a stable health condition following the initiation of ART, and being below 18 years of age. A total of 29 participants (8 = co-morbidity, 16 = unstable health condition, 5 = < 18 years old) did not meet the inclusion criteria and were excluded from the study. Participants completed a paper-and-pencil survey on ART medication adherence, doctor–patient communication, patient spirituality, self-efficacy, HIV stigma, and social support during clinic days. The survey was administered by the research team over a period of 1 month at the convenience of patients. The survey was completed in English language. Some (n = 13) participants who were not literate in the English language were assisted to complete the survey by the research team.
Permission to conduct the study was granted by the Internal Management Committee of Agogo Presbyterian Hospital which manages and supervises the HIV clinic. All of the study participants provided written informed consent, including consent for publication.
Research Ethics
This study was approved by the Ethics Committee for the Humanities (Protocol Number; ECH042/18-19), University of Ghana (details edited out for blind review). All procedures performed in the study followed the ethical standards of the Committee for the Humanities and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Measures
A 71-item survey questionnaire was constructed that included measures on doctor–patient communication, patient spirituality, self-efficacy, HIV stigma, social support, ART adherence and patient demographics (age, gender, employment, education, marital status, and religious affiliation).
Doctor–patient communication. Doctor-patient communication was assessed by the Communication Assessment Tool (CAT) (26). CAT is a 15-item scale rated on a 5-point Likert scale ranging from 1 (poor) to 5 (excellent). Higher scores indicate better doctor–patient communication. It assesses patients’ views of a physician's communication and interpersonal skills regarding their illness. Cronbach's alpha of .96 was reported for the scale (26). Cronbach's alpha reliability for the scale in this study is .97.
Patient spirituality. Patient spirituality was assessed by the Spirituality Scale (SS) (27). The SS is a 22-item scale rated on a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). Of the 22 items, 18 items were used in the current study. Higher scores indicate greater spirituality. SS is made up of 3 subscales: self-discovery, relationships, and eco-awareness. Previous research reported the following Cronbach's alpha coefficients for the 3 subscales: self-discovery (.81), relationships (.84), and eco-awareness (.94) (27). Cronbach's alpha reliabilities for the subscales in this study are self-discovery (.93), relationships (.94), and eco-awareness (.97).
General self-efficacy. Patient self-efficacy was assessed by the General Self-Efficacy Scale (GSE) (28,29). The GSE is a 10-item scale that assesses the belief in one's capabilities to cope with a broad range of stressful or challenging situations. The GSE is rated on a 4-point Likert scale ranging from 1 (not at all true) to 4 (exactly true). Higher scores indicate higher levels of perceived self-efficacy. Previous research reported the Cronbach's alpha coefficients of .93 and .89 for the scale (28,29). Cronbach's alpha reliability for the scale in this study is .94.
HIV stigma. HIV-related stigma was assessed by the HIV Stigma Scale (HSS) (30). HSS is a 12-item scale rated on a 4-point Likert scale ranging from (strongly disagree) to (strongly agree). Higher scores indicate higher levels of perceived stigma. HSS is a multidimensional scale with 4 subscales; personalized stigma, disclosure concerns, concerns about public attitudes, and negative self-image. Previous research reported Cronbach's alpha coefficients ranging from .80 to .88 for the 4 subscales (30). Cronbach's alpha reliabilities for the subscales in this study are personalized stigma (.78), disclosure concerns (.87), concerns about public attitudes (.84), and negative self-image (.85).
Social support. Social support was assessed by the Multidimensional Scale of Perceived Social Support (MSPSS) (31). MSPSS is a 12-item scale rated on a 7-point Likert scale ranging from 1 (very strongly disagree) to 7 (very strongly agree). Higher scores indicate higher levels of perceived social support. MSPSS has 3 subscales; family, friends, and significant other. Previous research reported the following Cronbach's alpha coefficients for the 3 subscales: family (.91), friends (.87), and significant other (.85) (31). Cronbach's alpha reliabilities for the subscales in this study are family (.93), friend (.92), and significant other (.93).
ART adherence. Antiretroviral medication adherence was assessed by 4 items selected from the Medication Adherence Rating Scale (32,33). The items were slightly modified and validated for this study. In this study, we rated all of the items on a 5-point Likert scale ranging from 1 (very untrue of me) to 5 (very true of me). Sample items are “I sometimes forget to take my antiretroviral medicine,” and “I sometimes stop taking my antiretroviral medicine when I feel worse.” The items were reverse-scored such that higher scores indicate higher levels of medication adherence. In this study, Cronbach's alpha reliability for the 4 items is .98.
Statistical Analysis
We examined the main study variables for correspondence with normality assumptions of parametric tests. The distribution of scores was checked against skewness and kurtosis cut-off index of ± 2 (34). Following this, mean, standard deviation, and range of scores were calculated. To assess the construct dimensionality of the main study variables, we conducted exploratory factor analyses (EFAs) on each of them. We calculated separate EFAs on each subscale of all multidimensional scales in this study. The principal component factor extraction method was used throughout. Items were retained if they loaded > .40 (35). We requested a one-factor solution with oblique rotation for each subscale of a multidimensional scale following the scale developer's manual. Following this, we requested Cronbach's alphas for all multi-item scales. Then, we computed total scale scores for the main variables and calculated bivariate correlations. Finally, the hypotheses were tested with Hierarchical Linear Regression in 2 steps. At Step 1, we entered the demographic variables into the equation as control variables. At Step 2, we added the predictors of medication adherence to the equation. Differences between men and women in medication adherence were tested with Independent Samples t-test. All of the analyses were undertaken in SPSS (v25).
Results
Table 1 presents the sociodemographic characteristics of the participants. As can be seen in Table 1, half (50.4%) of the sample is female. On average, participants reported being on antiretroviral treatment for almost 4 years. The majority of the participants were between 26 and 35 years of age (45.6%).
Sociodemographic Characteristics of Study Participants (N = 349).
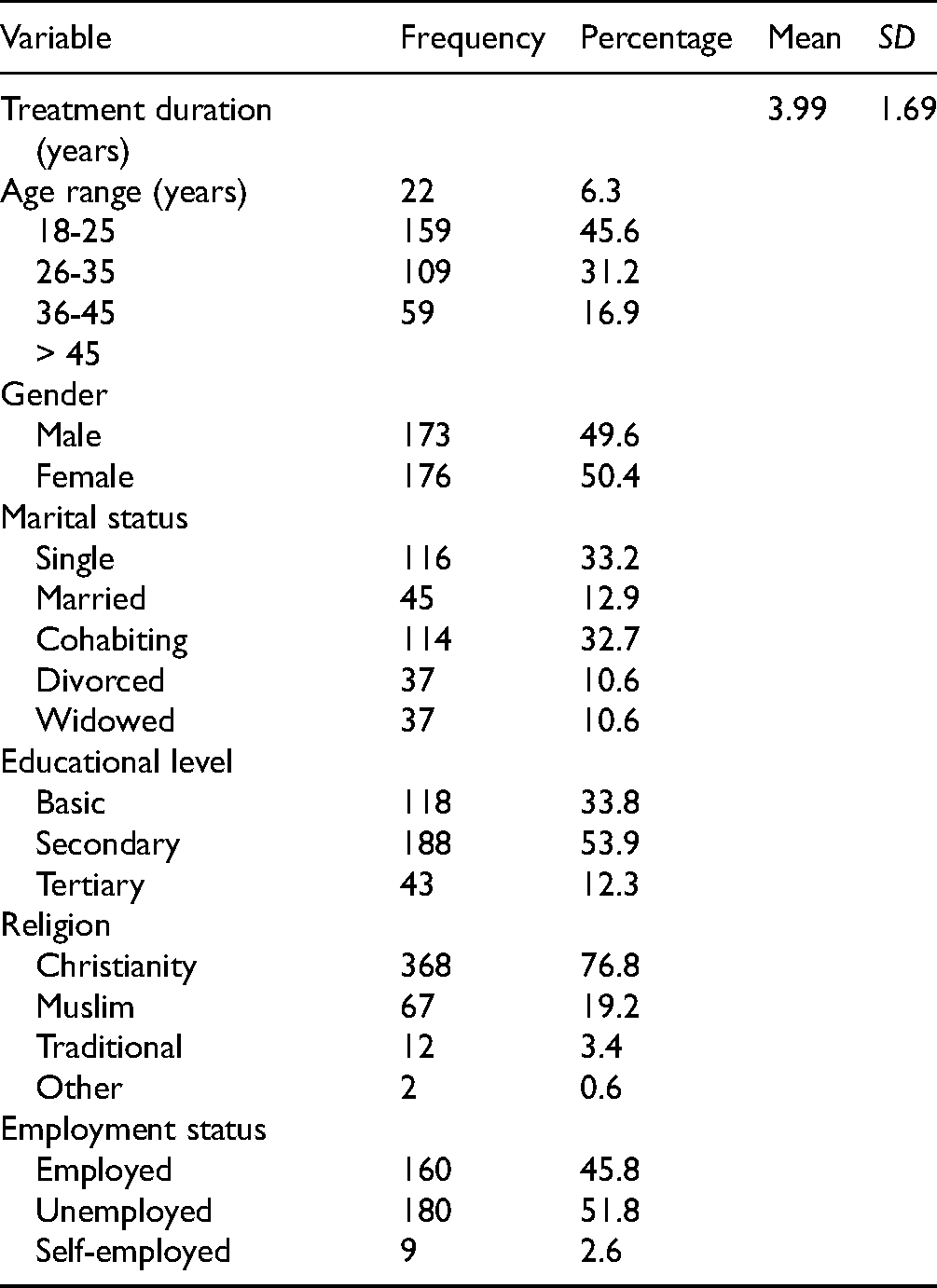
Table 2 presents the intercorrelations among the variables together with the descriptive statistics. Most of the variables are moderately intercorrelated (see Table 2).
Descriptive Statistics and Intercorrelations among the Study Variables (N = 349).
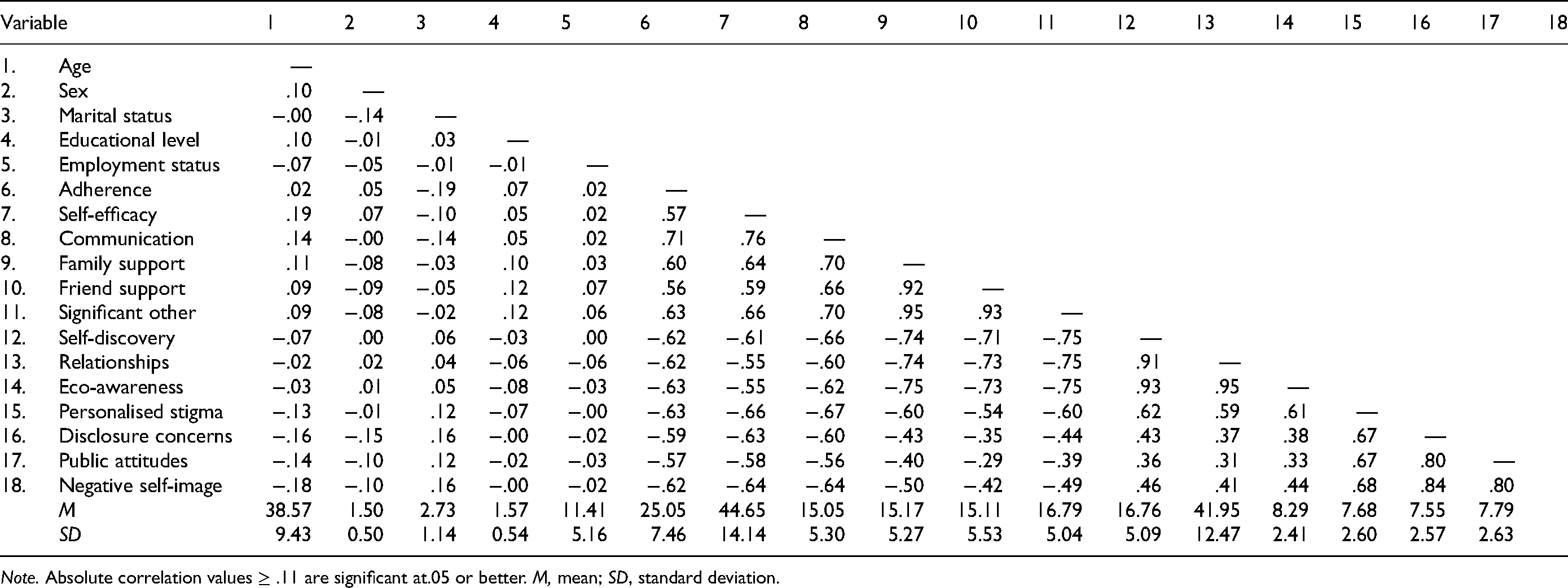
Note. Absolute correlation values ≥ .11 are significant at.05 or better. M, mean; SD, standard deviation.
Table 3 presents the results of the Hierarchical Linear Regression analysis. The model at Step 1 (demographic variables) was statistically significant, accounting for a 4.8% variance in ART adherence (see Table 3). Specifically, the results showed that only patient marital status (β = –.19, 95% CI [–1.36, −0.42], P <.001) was significantly negatively associated with ART adherence.
Multiple Regression Model Predicting Antiretroviral Medication Adherence from Self-Efficacy, Doctor–Patient Communication, Social Support, Patient Spirituality, and HIV Stigma.

Note. Age (quantitative data); gender (1, male, 2, female); educational level (1, basic, 2, secondary, 3, tertiary); marital status (1, married, 2, single, 3, cohabiting, 4, divorced, 5, widowed); employment status (1, employed, 2, unemployed, 3, self-employed).
CI, confidence interval **P <.01, ***P <.001.
In addition, the model at Step 2 was statistically significant, with all of the predictors accounting for 61% incremental variance in ART adherence (ΔR2 = .610, P <.001). Specifically, results showed that doctor-patient communication (β = .38, 95% CI [0.09, 0.18], P <.001) and social support from significant others (β = .46, 95% CI [0.18, 0.67], P <.001) were significantly positively associated with ART adherence. In contrast, personal spirituality (β = −.22, 95% CI [−0.44, −0.00], P <.05), HIV stigma (β = −.16, 95% CI [−0.58, −0.09], P <.01), and patient self-efficacy (β = −.14, 95% CI [−0.17, −0.02], P <.01) were significantly negatively associated with ART adherence. Other analysis indicated that men and women did not differ significantly in ART adherence, t(347) = −1.00, P = .316 (2-tailed). In summary, the regression model explained a total of 65.8% variance in ART medication adherence (see Table 3).
Discussion
The results of the present study demonstrated that doctor–patient communication and social support from significant others were positively associated with ART adherence in this sample. These results suggest that our participants perceive favorable communication between healthcare workers and patients as well as social support from significant others, including physicians, as facilitators of ART adherence. Other work has found that quality information flow between healthcare workers and patients as well as supportive relationships help to retain PLHIV on ART (36).
In addition, various authors have reported a positive relationship between social support and medication adherence. There is evidence that social support tends to improve the health of HIV patients on ART (37,38). A study among HIV-positive heterosexual men found that patients who reported higher levels of social support experienced optimal ART adherence than those who reported lower levels of social support (39). This result suggests that social support has an important role to play in ART adherence among PLHIV.
However, in this study, social support from family and friends was not associated with ART adherence in this sample. This result is consistent with previous work in Ghana which found that, due to affiliate stigma, family and friends tend to provide less than optimal support to patients, compared with support from significant others (40,41). It is, thus, probable that PLHIV in the Asante Akim North District do not seem to receive the support they need from family and friends because of affiliate stigma.
The finding regarding the positive relationship between doctor–patient communication and medication adherence is supported by previous research among PLHIV in Ghana, which found that health workers’ general, positive attitudes and behavior towards HIV patients during clinical encounters, including supporting patients financially and empathizing with them, were helpful for ART adherence (42). Good doctor-patient communication is held to be vital for adherence to drug therapies. A meta-analytic work has shown that warm communication between healthcare workers and patients in clinical care enhances patients' adherence to medication and treatment (43). Earlier research found that quality communication between healthcare workers and patients had a positive impact on medication adherence (44).
Moreover, we found that in this study patient spirituality was negatively associated with ART adherence. In other words, as patients’ spirituality increases, their adherence to ART medication decreases. This result is consistent with that of an earlier research on medication adherence in Ghana among patients with hypertension (45). Patient spirituality/religiosity has long been shown to impact coping behavior (46,47). Ghana is considered a religious country (48), where census data show that 71.2% of Ghanaians are Christians, 17.6% are Muslims, 5.2% are Traditionalists, and 5.3% are unaffiliated (Ghana Statistical Service, 2012). Consequently, it is possible that the present sample relied heavily on their spiritual resources to cope with their illness rather than follow their drug regimen. That is, our patients’ spirituality seems to override their motivations to take their medication.
A second possible explanation for the results on patient spirituality being negatively associated with ART adherence could arise from the large/high stigma associated with a sexually induced disease (which would lower adherence to the medication given the high stigma). Relatedly, a systematic review has reported that the relationship between patient spirituality and medication adherence is less than clear (49). Of the 33 studies reviewed, the author found that 24 studies reported positive associations between spirituality and adherence regarding clinical health outcomes, whereas 12 studies found a negative association between the 2 variables. The study concluded that more studies are needed to clarify the spirituality–medication adherence relationship (49).
Further, we found that HIV stigma was negatively associated with ART adherence. This finding is consistent with that of a recent study in Ghana which found that HIV stigma, especially from community members, was not only preventing people from disclosing their HIV status but also from assessing healthcare (50). There is substantial empirical evidence linking HIV-related stigma to poor ART adherence and HIV outcomes (50,51). For example, perceived stigma was found to have a greater impact on the disclosure of HIV status, which, in turn, affected ART medication adherence (52). Systematic reviews and meta-analyses have demonstrated that not only does HIV stigma relate negatively to adherence but also it has detrimental effects on various health-related outcomes in PLHIV (53,54). Other research has shown that HIV stigma seems to be persistent among African Americans, thwarting HIV-risk reduction efforts (55).
Patient self-efficacy is crucial in adherence to medication and health behavior (56,57). This is because medication-taking requires beliefs in one's efficacy and the controllability to follow a drug regimen. However, in this study, patient self-efficacy was negatively associated with ART adherence in this sample. Our results contrast with those of an ART medication adherence study among PLHIV in Pretoria, which found a strong positive relationship between medication adherence and adherence self-efficacy (58). The authors concluded that interventions aimed at improving medication adherence should consider adherence self-efficacy. It is possible that our participants do not feel they possess self-efficacy/controllability over ART adherence may be due, in part, to the structure of the ART regimen itself or to other challenges such as financial challenges and travel time. A second possible explanation is that our sample may be experiencing pill burden arising from the combination therapy (cART; about 3 drugs combined), which could reduce patients’ motivation to carry on with the prescribed medication.
Furthermore, there were no gender differences in our sample regarding ART adherence. It would seem that both men and women in the present study consider ART medication adherence to be crucial for their physical well-being in a similar way. In summary, the results of the present study demonstrated that effective doctor–patient communication is considered an essential factor for medication adherence.
Limitations
As with most observational studies, the present study has important limitations to note. The limitations of this study arise primarily from the cross-sectional design and self-report data used. ART adherence takes place over time. Thus cross-sectional data would not provide a clearer picture of adherence because such data cannot be used to examine intra-individual ART adherence change over time. Further, it is well known that self-report data are attended by response bias. We also did not incorporate in the design of the study information on social desirability to help identify socially desirable responding, which is known to affect survey responses. From the foregoing, we advise that interpretation of the results should take these limitations into account. Future research on ART adherence in Ghana would benefit from the use of longitudinal research designs, which would enable researchers to follow patients on ART over time.
Conclusion
The findings of the present study provide opportunities for educational interventions targeted at reducing the barriers to ART medication adherence while enhancing the facilitators of ART adherence in the Asante Akim North District. The results show that quality doctor–patient communication is an important factor in medication adherence, at least, in the present sample. Therefore, hospital and clinic management should organise “open day programs” to give patients and the public opportunities to interact with healthcare workers, particularly physicians and nurses. Physicians and nurses would also benefit from refresher courses aimed at enhancing their communication skills and relationships with patients. There is an urgent need for the Ghana AIDS Commission to liaise with community HIV focal persons to design stigma reduction interventions to target HIV stigma at community settings in rural Ghana. In addition, family and friends of PLHIV require further education on how they can support PLHIV while warding off affiliate stigma. Further, religious congregations should be used as venues to raise awareness about the benefits of medication adherence alongside spirituality. Useful examples of how religious congregations can be utilized in the HIV prevention and care continuum are available elsewhere (59–62).
Footnotes
Research Ethics and Patient Consent
This study was approved by the Ethics Committee for the Humanities (ECH) (Protocol Number: ECH042/18-19), University of Ghana. University of Ghana's ECH complies with the American Psychological Association (APA) Committee on Animal Research Ethics (CARE) as well as the APA Committee on Human Research (CHR). In addition, all procedures performed in the study were in accordance with the ethical standards of the ECH of the University of Ghana and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Permission to conduct the study was granted by the Internal Management Committee of Agogo Hospital, which manages the HIV clinic. All of the study participants provided written informed consent, including consent for publication.
Authors‘ Contributions
ETK, MF, and JSY conceptualized the study. MF collected the data. ETK analyzed the data and interpreted the results. ETK wrote the manuscript and reviewed it for critical intellectual content. All authors read and approved the final manuscript.
Availability of Data
The data on which the article reports are available from the corresponding author on reasonable written request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.