
Abstract
Background
Effective patient–doctor communication about complementary and integrative health (CIH) is crucial to coordinate multimodal treatment for complex conditions. While rates of patient disclosure of CIH use to physicians have increased in the United States over the last 30 years, many patients still do not disclose these facts. Integrating CIH approaches within academic medical centers may enhance the communication, but this has not been explicitly studied.
Objective
To examine rates of patient disclosure of CIH to physicians and reasons for nondisclosure.
Methods
We surveyed 1177 patients at an academic center’s CIH clinic regarding their CIH use and disclosure of CIH use to their physician.
Results
Of the 1067 who responded to the disclosure questions, 80.1% had discussed their CIH use with their physician, while 19.9% did not. Of those who did not disclose, lack of physician inquiry was reported by 58% as the principal reason.
Discussion
Within an academic center, there is still a need to improve communication about CIH use. Possible strategies might include continued education of both patients and physicians about CIH and communication skills and integration of CIH disclosure into routine patient health questionnaires.
Keywords
Introduction
Given the increasing use of complementary and integrative health (CIH) approaches in the United States and worldwide,1,2 it is essential for physicians to discuss CIH use with their patients. Higher levels of patient disclosure of CIH use inform optimal and integrated patient-centered care and minimizes the chance for adverse interactions with other therapies. According to the 2012 National Health Interview Survey, about one third of U.S. adults used at least one CIH modality in the past 12 months, including natural products, chiropractic, and mind–body therapies. However, only 57% of those surveyed discussed their CIH use with their conventional provider. 1 While reported levels of disclosure in 2012 were notably higher than those reported in earlier national surveys (eg, 38.5% and 39.1% in 1997 and 2002, respectively),3,4 there remains a gap between patient use and discussion of CIH, with the absence of physician inquiry about CIH use remaining a primary reason for lack of disclosure. 1
Integrating CIH approaches within academic medical centers has been suggested as a way to increase communication but has not been evaluated in terms of the effect of such integration on patient disclosure of CIH use. We report the results of a survey of new patients at an CIH medical clinic in an academic medical center regarding their disclosure of CIH use and reasons for nondisclosure.
Methods
This study took place at the Osher Clinical Center (OCC) for Complementary and Integrative Medicine at Brigham and Women’s Hospital (BWH) and was approved by the Partners Healthcare Institutional Review Board. The OCC was begun in 2007 and is located within the Ambulatory Care Center of BWH in Boston, a Harvard Medical School-affiliated hospital. In the OCC, all CIH therapies take place alongside conventional care and the OCC team is trained to deliver coordinated care. 5 This study was conducted from May 16, 2011 through October 22, 2014. Each new patient to the OCC was sent a survey to complete before their first visit.
The survey included 23 questions about prior CIH use, main reason for coming to the OCC, referral source, and communication about their CIH use. Patterns of communication and reasons for not discussing CIH use were summarized only for respondents who indicated having used CIH within the past 12 months. Respondents were asked whether they “discussed all or most,” “discussed some,” or “did not discuss” their past 12-month CIH use with their conventional provider. For this analysis, answers for “discussed all or most” and “discussed some” were combined. Those who answered “did not discuss” were asked to indicate all the reasons why they did not disclose their CIH use.
Results
A total of 1537 patients were seen for the first time in the OCC during the study period; 1509 of these (98%) completed the survey. Of these, 1177 patients indicated having used CIH within the past 12 months and formed the basis of the analysis. As shown in Table 1, the study population was mostly female with higher socioeconomic status. One half of the participants were referred to the OCC by a conventional provider, and the main reasons for coming to the OCC were back and neck pain and other musculoskeletal concerns.
Characteristics and Disclosure Patterns of OCC Patient Population.
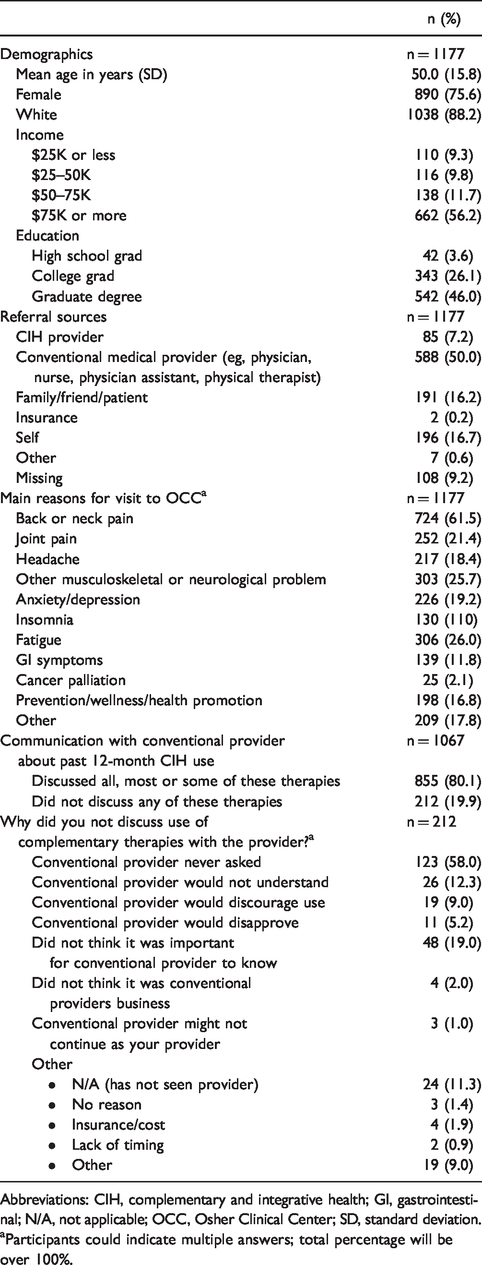
Abbreviations: CIH, complementary and integrative health; GI, gastrointestinal; N/A, not applicable; OCC, Osher Clinical Center; SD, standard deviation.
aParticipants could indicate multiple answers; total percentage will be over 100%.
Of the 1067 patients who responded to the questions about CIH use disclosure, 80.1% reported that they had discussed and 19.9% reported that they had not discussed their CIH use with their conventional care provider. Of those who did not disclose (n = 212), more than half indicated their main reason for nondisclosure was that the provider never asked (58.0%). Additional reasons included that they did not think it was important for provider to know (19.0%), provider would not understand (12.3%), and that they have not seen a provider yet (11.3%). Patients referred by a conventional provider tended to disclose more to their provider than those referred by other sources including self, family, friends, other patients, CIH providers, and insurance providers (79.6% and 66.5%, respectively).
Discussion
These data address disclosure of CIH use among patients presenting at an academic medical center. Our survey, based at an academic center’s integrative medicine (IM) clinic, found rates of disclosure (80.1%) higher than those reported in the most recent national survey (57% in 2012). Whether this observation of increasing disclosure is due to the location of the OCC within an academic center, to differences in population of the 2 surveys, or to changes over time cannot be determined by this study. In addition to in national surveys, disclosure patterns have also been reported in studies at primary care centers6,7 and in specific patient populations, 8 such as low-income diabetes patients, 9 and women with HIV, 10 with varying rates of disclosure reported. Since our study at an integrative medical center differed from prior studies examining national, local, or targeted patient populations, our findings are difficult to compare directly. Findings of surveys conducted across a range of IM clinics based in academic centers are needed to evaluate possible benefits to disclosure rates due to colocating CIH and conventional programs.
However, there continues to be a substantial percentage of patients who utilize but do not disclose their CIH use to their providers (19.9%), and the reasons for nondisclosure, particularly lack of physician inquiry, remain the same as previous surveys. 1 Multiple initiatives have been in place since 1990 at Harvard Medical School and its affiliated hospitals related to CIH education, research, and care, yet patients continue to report that their doctor is not asking, or they believe CIH use is not important to discuss with their conventional providers.
In order to recommend appropriate patients for CIH and avoid potential adverse events, it is critical for physicians to be knowledgeable of any potential risk factors for a given therapy. For example, St. John’s Wort, which is a commonly recommended nutritional supplement used to treat mild depression and anxiety, is known to reduce the effects of oral contraceptives and warfarin.11,12 Conditions such as osteoporosis may present a relative or absolute contraindication to certain types of high-velocity spinal manipulative therapies. 13 Increased communication between physicians and patients could also lead to more optimal care that integrates CIH modalities into multimodal therapeutic approaches. For example, clinical trials support integrating acupuncture into the management of cancer-related pain and nausea 14 and chronic musculoskeletal pain treatment, 15 and observational studies suggest that chiropractic care may complement conventional care for migraine headache. 16 Lack of communication could lead to missed opportunities for physicians to advise on CIH safety or to develop an integrated care plan.
To further assure safe and optimal patient care, we encourage continued training for physicians to inquire about CIH use and to integrate these discussions as part of routine care. Many medical schools have introduced curricula for their students to increase exposure to CIH modalities, and some hold regular CIH-related grand rounds and seminars. Knowledge obtained in these programs may encourage discussion about CIH and enhance patient–provider interactions. Including questions about CIH products and modalities in patient health questionnaires may also encourage patients to discuss their CIH use and remind physicians to ask about CIH use without increasing burden on time constraints.
In terms of limitations, this survey was not able to specify to which doctor or when patients disclosed their CIH use, nor which CIH modalities were disclosed. Additionally, generalizability about patient disclosure of CIH use is limited by the focus of this study within an academic IM clinic and the high prevalence of females with higher socioeconomic status in the study population. Finally, half of the patients in the study were referred by a conventional provider, which may have contributed to higher disclosure. However, the structure of the survey did not allow us to examine to which provider patients disclosed the use of CIH. These limitations highlight needs for further research regarding CIH disclosure including communication about specific CIH modalities and the effect of patient and provider demographics on disclosure.
In conclusion, while disclosure of CIH use has increased nationally over time, there is still a need for improved communication. By encouraging physicians to inquire about CIH use and educating both patients and physicians about CIH and communication skills, patient–provider communication about CIH may increase. Such an approach holds promise to make patient care safer, more effective, and more aligned with patient goals and values.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NIH R01-AT005065 and K24-AT009282 from the National Center for Complementary and Integrative Health at the National Institutes of Health.