
Abstract
Knee osteoarthritis (KOA) is the most common type of arthritis affecting people of older age. The study assessed the effectiveness of nurse-led intervention on quality of life (QOL) of patients with KOA. A quasi-experimental pretest–posttest control group research design was adopted. Data was collected from 200 patients with KOA. The pre- and post-interventional QOL were assessed on the 15th day, 30th day, 60th day, and 90th day with a 36-item short-form health survey. A remarkable statistically significant improvement in QOL of patients with KOA in the study group was found in the IV test conducted on the 90th day (P < .001). The study concluded that a 12 weeks’ nurse-led intervention has resulted in significant improvement in the QOL of patients with KOA.
What do We Already Know About This Topic?
Previous literature reported that exercises for hamstring and quadriceps muscles and isometric exercises helped in pain reduction, strengthened the muscles, and improved the QOL in patients with knee osteoarthritis (KOA). However, very limited information is available on the effectiveness of isometric exercise and counseling on the QOL of patients with KOA.
How Does Your Research Contribute to the Field?
The novelty of the study finding is that the study found that a 12 weeks’ nurse-led intervention has resulted in significant improvement in the QOL of patients with KOA. Therefore, the study concluded that the nurse-led intervention comprising isometric exercise and counseling should be a part of regular nursing care in patients with KOA, which would be beneficial in the improvement of their QOL. This information will add new information to the field of nursing.
What are Your Research's Implications Toward Theory, Practice, or Policy?
As the study concluded that 12 weeks’ nurse-led intervention has resulted in significant improvement in the QOL of patients with KOA, this information shall be communicated to the educational policymakers to add this evidence-based information to the nursing curriculum. Moreover, this information shall be communicated to the hospital administrators to add it as a best practice guideline to be followed while caring for the patients with KOA.
Introduction
Osteoarthritis (OA) is the most common type of arthritis and one of the disabling diseases worldwide. Globally, the age-standardized point prevalence and annual incidence rate of OA in 2017 were 3,754.2 (95% uncertainty interval [UI] 3,389.4 to 4,187.6) and 181.2 (95% UI 162.6 to 202.4) per 100,000. The global prevalence was higher in women and increased with age, peaking at the >95 age group among women and men in 2017 (1). World Health Organization (WHO) reported that OA affects 9.6% and 18% of men and women, respectively, worldwide, especially those in the age group of 60 and above (2). OA is the second most common rheumatologic problem with a prevalence of 22% to 39% in India (3). The recently reported prevalence of OA in India is 21.6% (4). OA accounts for 2.4% of all years lived with disability (YLD) and is the tenth leading contributor to global YLDs. Worldwide, a whopping 240 million people are believed to be suffering from hip and knee OA (KOA) leading to 13 million YLDs (5).
OA affecting the knee joints often becomes painful, stiff, and swollen significantly depriving the patients of their routine activities (6). Patients with KOA experience severe disability and the global prevalence of KOA was 16% among individuals aged 15 years or over and 22.9% among those aged 40 years or over. Furthermore, approximately 654.1 million individuals worldwide had knee OA in 2020. The ratios of prevalence and incidence of KOA in women and men were 1.69 and 1.39, respectively. Of these patients, around 80% of them experience a reduction in their movement and 25% find it difficult to engage in their day-to-day activities (7). In India, the people of old age are vulnerable to be affected by KOA and it has been found that 28.7% of people are diagnosed to have KOA. It is estimated that age, obesity, and a sedentary lifestyle would be the cause of a 40% increase in KOA in 2025 (8).
Since the impact of the disease is significant, KOA besides causing pain and disturbing the normal activities of an individual causes changes in the morphology of subchondral bones, degeneration of cartilage, and damage to the soft tissues surrounding the cartilage. Furthermore, the less involved joints due to limited exercise force the people of old age to lose their muscle tone and strength. The feeling of pain, compelled by the absence of social contact and reduced earning capacity can lead to emotional imbalance (9). Apart from the physiological and functional disabilities the KOA causes, there are a number of factors including social interactions, and psychological and emotional outlook that does change the quality of life (QOL) of patients with KOA (10). As KOA is associated with pain and functional disability, it affects the QOL in these patients (11).
OA in general and KOA in specific are chronic conditions. There are many successful surgical, pharmacological, and non-pharmacological interventions available to manage the condition. In particular, many patients prefer non-surgical and non-pharmacological treatment and approaches considering the pain and other consequences associated with the surgery. Therefore, surgical treatment should be delayed as much as possible to avoid the need for revision surgeries. On the other hand, non-surgical and non-pharmacological nurse-led interventions can be planned in an individualized manner according to the patient's needs and preferences which is undeniably extremely significant will retain the QOL intact (12).
Exercise therapy, one of the non-pharmacological methods is found to be appropriate to help patients with KOA to delay the disease progression, reduce the pain and ensure better functioning of the knees (13). Strengthening exercise for quadriceps and hamstring muscles reduces subjective knee pain, increases the range of motion (ROM), and decreases the limitation of functional performance (14). An 8-week strengthening exercise for quadriceps and hamstring muscles could improve not only the QOL of patients with KOA, but also reduces the pain besides enhancing the functional activities (15). In addition to muscle strengthening exercises, counseling the patients with health education on KOA would improve their QOL. In previous studies, therapeutic health education and functional re-adaptation were found helping patients with KOA in improving their QOL (16). Moreover, it is recommended that an individualized management approach with health teaching is essential to improve QOL of patients with KOA (17).
Patients with KOA attending the orthopedic outpatient department (OPD) in the hospitals have prerogative need to develop their awareness about KOA and also about the remedial measures to lessen the degree of effect of the disease by following the exercise schedule, keeping the knee joint posture while engaging in physical activities, besides precautionary measures against obesity. Nurses play an important role in educating the patients on KOA and demonstrating effective exercises to reduce the pain and to improve the QOL through nurse-led intervention programs. Very little information is known about the efficacy of nurse-led interventions including exercise and education on the QOL of patients with KOA in India. Therefore, this study aimed at evaluating the effectiveness of nurse-led Intervention on QOL of patients with KOA (Figure 1).
Effect of nurse-led intervention on QOL of patients with KOA in the study group.
Methods
Design
The study adopted a quantitative research approach and a quasi-experimental pretest–posttest control group research design.
Setting
The study was conducted in two different settings, MIOT hospital, Madurai, Tamil Nadu, India as control group and Devadoss hospital, Madurai, Tamil Nadu, India as study group. The patients selected in this study were attending the orthopedic OPD of these hospitals. These hospitals were chosen as the patient characteristics and the type of care provided was similar in both the hospitals.
Hypothesis
The study assumed that there will be significant difference between the pre- and post-interventional level of QOL of patients with KOA before and after the nurse-led Intervention.
Sample
The investigator randomly allocated the study and control group. After random allocation, a total of 100 eligible samples each in the study and control group were selected by using a non-probability purposive sampling technique. In both groups, the participants were matched for age and sex. In both the study and control groups, the participants and the person who was assessing the outcomes were blinded. The sample included patients with grades I, II, and III KOA seeking health service from the orthopedic OPD of two large hospitals. The study was conducted over a period of one year.
Sample Size
The sample size was calculated based on pilot study results. The health-related QOL baseline score was 350 and it is expected to improve after the intervention to at least 380 scores with 50 SD. So the sample size was calculated using the 30 improvement score and meaningful difference score, with α and β errors are 1% and 5%. The calculated sample size was 99 per group.
Required information:
Anticipated common SD = σ Level of significance = 100 (1 − α) % Power of the test = 100 (1 − β) % Medically meaningful difference = d
σ = 50 α = 2.58 (1% level of error) β = 1.65 (95% power of the test) d = 30
Hence, 100 patients with KOA were selected for the study and control group and the total sample of the study was 200.
Inclusion and Exclusion Criteria
The inclusion criteria included patients confirmed having KOA, patients with radiological evidence of primary KOA of grades I, II, and III on the Kellgren Lawrence scale, aged between 45 and 65 years, both males and females, and patients having unilateral or bilateral involvement. Patients with other inflammatory joint diseases, critically ill patients, patients with a history of malalignment of the knee including varus/valgus, having any other comorbid diseases, having major psychiatric disorders, patients who had the plan to undergo joint replacement surgery, patients receiving a steroid injection, patients who had knee arthroplasty, and the patients who were undergoing physiotherapy in the past 6 months were excluded from the study.
Ethical Considerations
Before the initiation of the study, the institutional ethical approval was obtained from the research and ethics committee of XXXX, Tamil Nadu, India. The permission for data collection was sought from two large private hospitals, Tamil Nadu, India. Following a detailed description of the research procedures, written informed consent was signed by the participants. In addition, it was explained that their participation was voluntary and that they could leave the research at any moment without giving a reason. There were no risks or harm involved in participating in the study.
Study Instruments
QOL was assessed using a 36-item short-form (SF-36) health survey tool (18). The SF-36 scale was categorized under 8 domains including physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. All the domains were grouped under two components, namely physical component and mental component, and have a different number of items. The physical component includes physical function (10), role physical (4), pain (2), and general health (6). The mental component includes role emotional (3), vitality (4), emotional well-being (5), and social functioning (2). Each item was scored on a 0 to 100 range scale. The items in the same scale were averaged together to create the 8 domain scores based on the obtained score. The scores were arbitrarily grouped into 4 categories, low (0-200), moderate (201-400), high (401-600), and very high (601-800) QOL, respectively. The overall Cronbach's alpha coefficient of the SF-36 questionnaire was .791. The SF-36 questionnaire is reliable and valid (19). The study was found to be suitable for use in India (20).
WOMAC scale was used to assess the level of pain of the patients with KOA (21). It is a 5-point Likert scale and had 24 items. The level of pain was assessed under three dimensions, namely pain, stiffness, and physical function. The maximum score was 4 and the minimum score was 0 for each item. Based on the total score obtained, the level of pain was classified as 0: no pain; 1: mild pain; 2: moderate pain; 3: severe pain; and 4: extreme pain. “0” indicated no pain; 1-24 mild pain; 25-48 moderate pain; 49-72 severe pain; and 73-96 extreme pain. The pain was assessed on the 15th, 30th, 60th, and 90th day in both study and control groups.
Nurse-Led Intervention (Counseling and Isometric Exercise)
Counseling
Individualized counseling was given to the participants of a study group in six sessions for 6 days using flashcards and PowerPoint presentations. The topics included; protecting joints from knee pain, role of body weight on knee pain, relaxation techniques, and prevention of complications. The counseling session lasted for 20 min. The participants were encouraged to express their difficulties and their doubts were clarified. The exercise sessions took place after all the educational counseling sessions were completed.
Isometric Exercise
The isometric exercise was demonstrated to the patients by the investigator and a return demonstration was done by the patients for six days for 40 min each day. On day 1, the patients were demonstrated with a warm-up isometric exercise for toe raise, heel raise, knee lift, leg bend, and lift. On day 2, the patients practiced and return and demonstrated the warm-up isometric exercise. The investigator demonstrated isometric quadriceps and adduction (pillow squeeze) exercises. On day 3, a return demonstration of warm-up exercise, isometric quadriceps, and adduction was performed by the participants. The investigator demonstrated an isometric hamstring set and tangle exercise (ankle cross). The patients were clarified if they had any doubts and were asked to continue the isometric exercise at home.
Isometric Quadriceps Exercise
The patients were instructed to lie in a supine position. A rolled-up towel was put beneath the knee. The patients were asked to pull their toes back and push the leg down to squeeze the towel and hold it for 10 s and then relax. The patients repeated it 10 times and 3 times a day. They were instructed to maximally activate their thigh muscle to strengthen the knee. This exercise is aimed to strengthen the quadriceps muscle.
Isometric Adduction (Pillow Squeeze)
The patients were instructed to sit up straight on a chair at the edge with both the knees flexed or lie on the floor with both legs flexed. A small pillow was positioned between the knees and asked to press the pillow until they could feel the quadriceps muscles contraction. They were asked to hold it for 3 to 7 s and relax. They were asked to repeat it 10 times, thrice a day. This exercise helps to strengthen the adductor muscle.
Isometric Hamstring Set
The patients were placed in a sitting position with knee bend and toes up. They were asked to keep their hands behind for support and instructed to dig their heels into the ground and pull back up to 45° without sliding heels. They also were instructed to hold for 10 s and repeat it up to 10 times thrice a day. This exercise helps to strengthen the hamstring muscles.
Knee Tangle Exercise
The patients were instructed to sit comfortably in a chair with the hip and knees at 90° of flexion, with ankles crossed. The ankles are pressed against each other to contract the quadriceps and contralateral hamstrings for a series of contractions. After 10 repetitions, the ankles are crossed in reverse fashion, and the opposing quadriceps and hamstrings are contracted. This exercise helps to strengthen the quadriceps and hamstring muscles.
On day 4, patients practiced the isometric exercise at home in the presence of the investigator. Patients practiced the isometric exercise at home in the presence of the investigator and the investigator distributed the validated and pretested pamphlets showing the photographs of the exercise including instructions. The patients also were provided with a home exercise adherence log which included the type and frequency of exercise performed each day during day 5. Finally, on day 6, the investigator assessed the patients’ performance of isometric exercise, the exercise log was reviewed, and mistakes while doing exercise were corrected. The patients were insisted to attend the follow-up sessions. All the participants were encouraged to continue to do home-based isometric exercise 3 times a day for 12 weeks.
Further reinforcement to do the exercise was given when the patient visited the orthopedic OPD during their subsequent visit. Their exercise log was verified and they were motivated to continue the exercises, besides their doubts were clarified. No attrition of participants was observed in the study. At the end of the data collection, pre-validated exercise pamphlets and counseling booklets were given to the participants of the control group. The pamphlets and booklets were validated by content and subject experts and were certified as valid to be provided to the participants of the study.
Data Collection Procedure
Socio-demographic variables included age, gender, education, occupation, type of work, marital status, number of children, family type, and monthly income. The clinical variables comprised 14 items to assess the duration of pain, knee site, moving pain, resting pain, movement limitation, joint stiffness, crepitus, radiation score, whether treatment was taken, duration of treatment, current treatment, attainment of menopause, age at attainment of menopause, and family history of osteoarthritis. Socio-demographic information and clinical profile were assessed using the tools prepared by the investigators of the study. The patients were assessed for anthropometric measurement using the stadiometer and digital weighing scale and the body mass index (BMI) was calculated. The socio-demographic and clinical variable information was collected from the patients. The current treatment and radiation scores of the KOA were retrieved from their medical records.
WOMAC scale was used to assess the level of pain of the patients with KOA. The pain was assessed on the 15th, 30th, 60th, and 90th day in both study and control group. QOL was assessed by using SF-36 for both groups. The patients were given the data collection instruments and their responses were marked on the instruments. It took 30 to 35 min to collect the pretest data from each sample. After the pretest, routine care was provided to the patients with KOA in the control group and the participants of the study group received the nurse-led intervention comprising counseling and isometric exercise along with the routine care. Posttest was carried out on day 15, day 30, day 60, and day 90 in both the study and control groups.
Data Analysis Procedure
Frequency, percentage, mean, and standard deviation were used as descriptive statistics to analyze the data. A repeated measure of analysis of variance (ANOVA) was used to compare the pain in both groups with four assessments. Normality checks were carried out on the residuals, which were approximately normally distributed. Sphericity is tested with Mauchly's test. Study data had not met the assumption of sphericity, so we used one of the alternative univariate tests—Greenhouse-Geisser correction. So repeated measures of ANOVA with a Greenhouse-Geisser correction were used in this study. Unpaired′ test and paired′ test were used to compare the mean of the variables in the independent and dependent samples. A chi-square test was conducted to compare the distribution of demographic variables and anthropometric measures that were similar to the group. Percentage with 95% confidence interval (CI) and mean difference with 95% CI were used to find the differences between pretest and posttest scores. A P-value <.05 was considered statistically significant.
Results
The current study determined the effectiveness of a nurse-led intervention on QOL of patients with KOA. With regard to the demographic variables, clinical variables, and anthropometric measurements, both the study and control groups were statistically significantly similar (Table 1). The majority of patients in both the groups belonged to the age group of 45 to 50 years. More than half of them were females. With regard to educational status, most of them in both groups had middle school education. Most of the patients in both the study and control groups were private employees. More than half of the patients in the study and control group were moderate workers. A large number of patients in both groups were married. The majority in both groups had 1 to 2 children. In relation to family type, the majority of them were in living nuclear families in both groups. Regarding the family income, 53% in the study group and 38% in the control group had an income above INR Rs. 9,000, which indicates that they belong to the upper-middle and upper class in their economic status based on the modified Kuppusamy scale (2007) (22).
Demographic Variables of Patients With KOA in Study and Control Group.

Abbreviations: KOA, knee osteoarthritis; DF, degrees of freedom; NS, not significant;.
Regarding menopause, 39% and 33% of women in the study and control group had menopause in 41 to 45 years. Regarding moving pain, all the patients in both groups had moving pain. With regard to resting pain, a large number of participants in both groups had resting pain. Regarding limitation of movement, a vast majority of them in the study and control group had limitations of movement. In terms of crepitus, 87% and 84% of them in the study and control group had crepitus. Among the participants, more than half of them in the study and control group had attained menopause. Of the samples, 32% in the study group and 38% in the control group had a family history of KOA. Most of them in the study and control group had heights ranging between 151 and 160 cm. Of the participants, 34% of them in the study and 29% of them in the control group weighed between 61 and 70 kg. With regard to BMI, 47% of them in the study group and 48% of them in the control group had a BMI of more than 30 (Table 2).
Clinical Variables of the Patients with KOA in Study and Control Group.

Abbreviations: KOA, knee osteoarthritis; NSAID, nonsteroidal anti-inflammatory drug; OA, osteoarthritis; DF, degrees of freedom; NS, not significant.
In this study, the majority of patients in both groups had a duration of pain between 7 months and 1 year. With regard to the site of knee pain, the patients in the study had pain in the right knee and patients in the control group had pain in both the knees. Regarding joint stiffness, all of them in both groups had joint stiffness of <30 min. In the radiological score of KOA, majority of them in both groups were found to be in stage II. More than half of the patients in both groups had taken treatment for 1-4 months. In both groups, all the participants were under the treatment with a nonsteroidal anti-inflammatory drug (NSAID; Table 3).
Level of Pain on 15th, 30th, 60th, and 90th day in Patients with KOA in Study and Control Group.

Abbreviations: KOA, knee osteoarthritis; S, significant; NS, not significant. *Significant, ***Highly significant.
QOL of patients with KOA in study and control groups before the intervention showed that none of them had a very high level of QOL in the pretest. Fifty-five percent of them in the study group and 57% of them in the control group had low QOL and 41% of them in the study group and 40% of them in the control group had moderate QOL. Only 4% of them in the study group and 3% of them in the control group had high QOL. The results showed no statistically significant difference in QOL between the study group and the control group in the pretest (χ2 = 0.19, P = .90).
The QOL scores were found to be low in all domains. Likewise, the mean role physical score of 24.96 with SD 24.16 in the study group and 24.11 with SD 23.01 in the control group also had a very low score than other domains. With regard to overall physical health, the mean score in the study group was 37.53, with SD 9.17 and in the control group, the mean score was 37.14, with SD 9.05. Regarding the overall mental health, the mean score was 49.63, with SD 5.88 in the study group, and the mean score in the control group was 49.40, with SD 5.90. These findings revealed that the overall physical health was affected more than the mental health in both groups. The mean score of different domains was found to be almost similar and comparable. This data is presented in Table 4.
Mean and Standard Deviation of QOL of Patients with KOA in Study and Control Groups Before Intervention.
(N = 200).

Abbreviations: QOL, quality of life; KOA, knee osteoarthritis; NS, not significant.
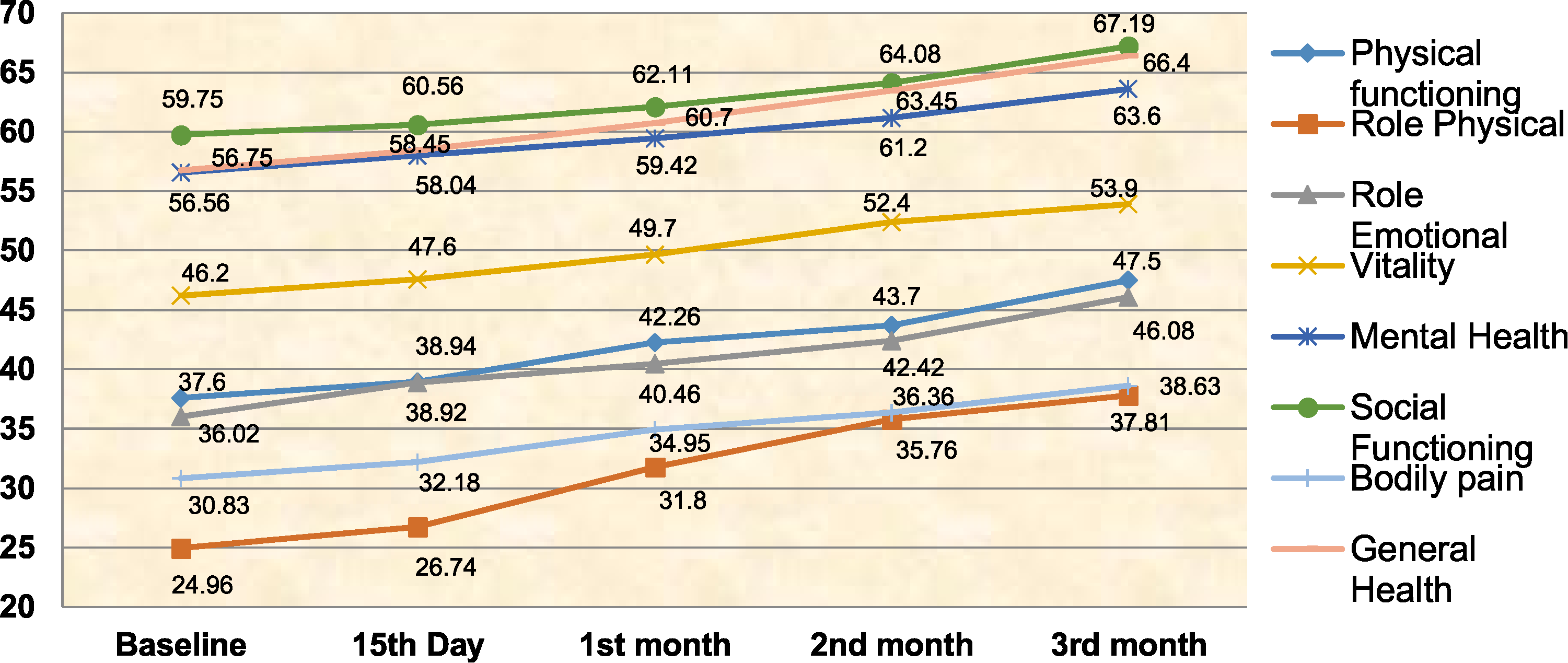
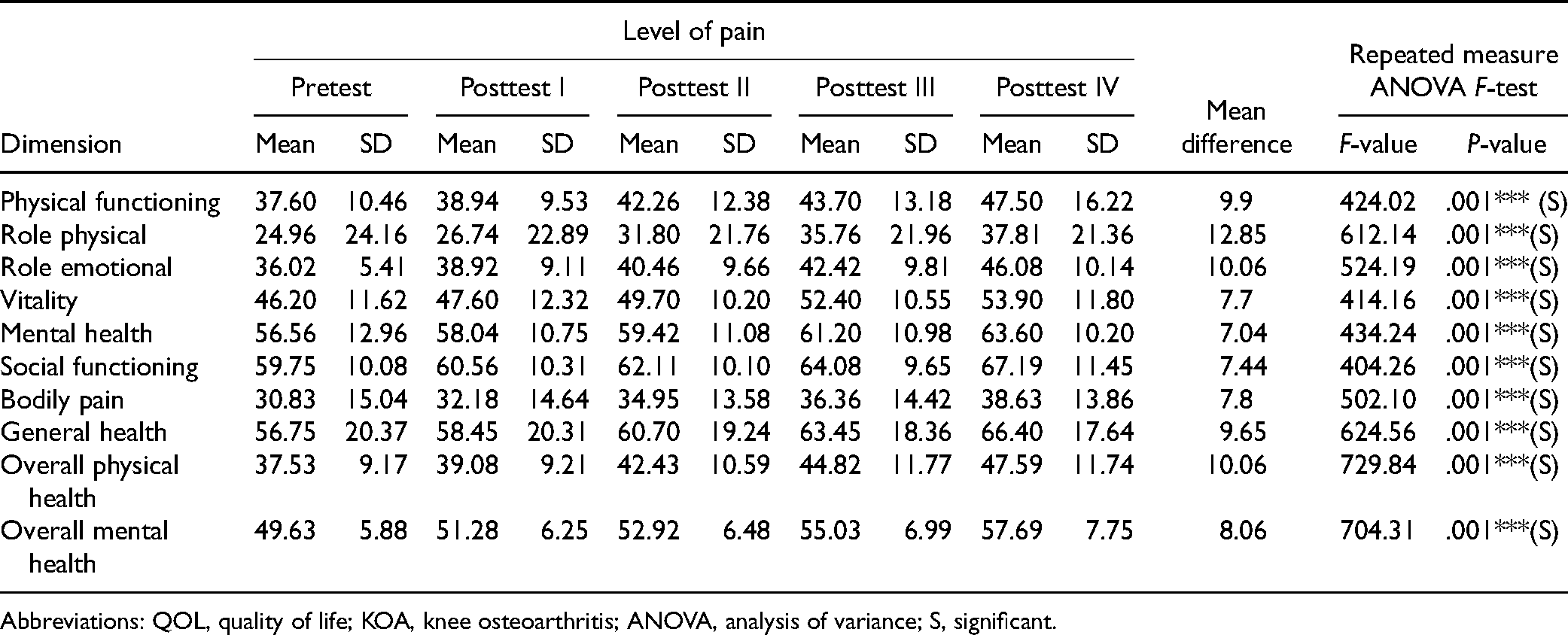
The result of the present study revealed that the mean score of physical functioning increased from 37.60 in the pretest to 47.50 in the posttest IV, and the mean difference was 9.9 after the intervention. The calculated ‘F’ ratio was 424.02 at the P < .001 level. The mean score of role physical increased from 24.96 in the pretest to 37.81 in the posttest IV, and the mean difference was 12.85 after the intervention. The calculated ‘F’ ratio was 612.14 at the P < .001 level. The mean score of role emotional increased from 36.02 in the pretest to 46.08 in the posttest IV, and the mean difference was 10.06 after the intervention. The calculated ‘F’ ratio was 524.19 at the P < .001 level. The mean score of vitality increased from 46.20 in the pretest to 53.90 in the posttest IV, and the mean difference was 7.7 after the intervention. The calculated ‘F’ ratio was 414.16 at the P < .001 level. The mean score of mental health increased from 56.56 in the pretest to 63.60 in the posttest IV, and the mean difference was 7.04 after the intervention. The calculated ‘F’ ratio was 434.24 at the P < .001 level. The mean score of social functioning increased, from 59.75 in the pretest to 67.19 in the posttest IV, and the mean difference was 7.44 after the intervention. The calculated ‘F’ ratio was 404.26 at the P < .001 level.
The mean score of bodily pain increased from 30.83 in the pretest to 38.63 in the posttest IV, and the mean difference was 7.8 after the intervention. The calculated ‘F’ ratio was 502.10 at the P < .001 level. The mean score of general health increased from 56.75 in the pretest to 66.40 in the posttest IV, and the mean difference was 9.65 after the intervention. The calculated ‘F’ ratio was 624.56 at the P < .001 level. The mean score of overall physical health increased from 37.53 in the pretest to 47.59 in the posttest IV, and the mean difference was 10.06 after the intervention. The calculated ‘F’ ratio was 729.84 at the P < .001 level. The mean score of overall mental health increased from 49.63 in the pretest to 57.69 in the posttest IV, and the mean difference was 8.06 after the intervention. The calculated ‘F’ ratio was 704.31 at the P < .001 level. The overall results inferred that there was an improvement in the QOL in all domains (physical functioning, role physical, role emotional, vitality, mental health, social functioning, bodily pain, general health, overall physical health, and overall mental health) in the study group after the isometric exercise and counseling. This data could be seen in Table 5.
Effect of Nurse-led Intervention on QOL of Patients with KOA in Study Group.
(N = 100).
Abbreviations: QOL, quality of life; KOA, knee osteoarthritis; ANOVA, analysis of variance; S, significant.
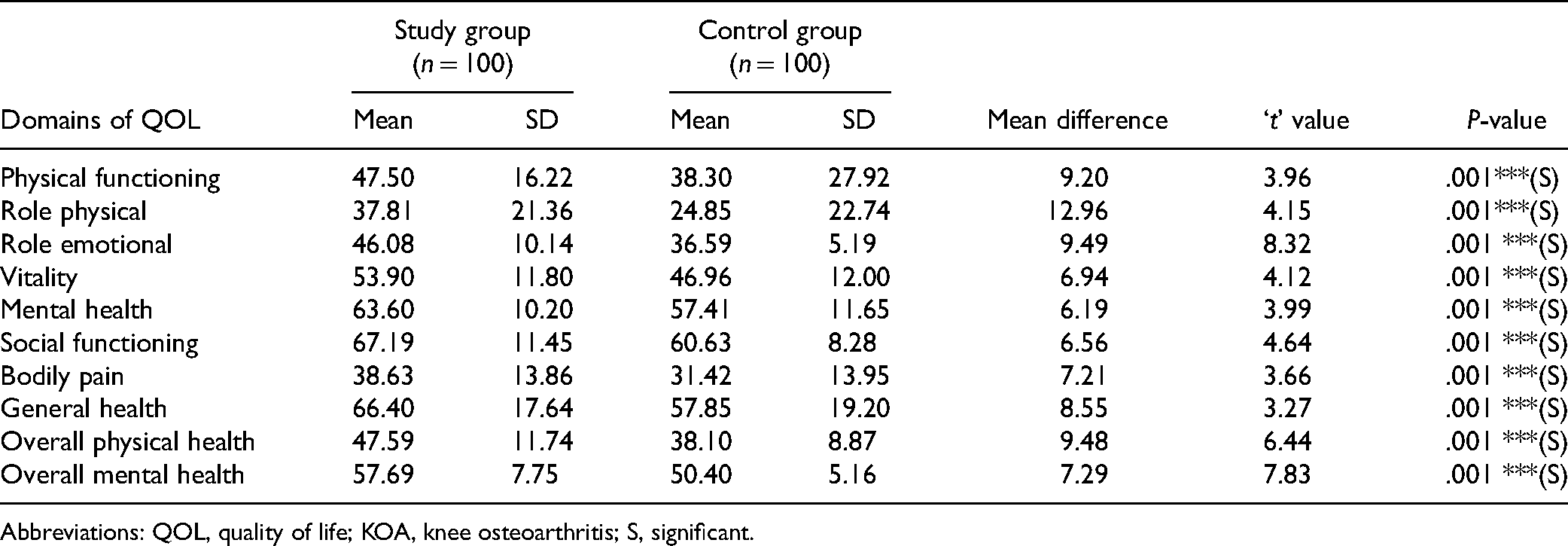
Table 6 shows the comparison of QOL of patients with KOA in the study and control group after the intervention posttest IV (day 90). The mean difference between the study and control groups in terms of “physical functioning” is (9.20, t = 3.96), “role physical” (12.96, t = 4.15), “role emotional” (9.49, t = 8.32), “vitality” (6.94, t = 4.12), “mental health” (6.19, t = 3.99), “social functioning” (6.56, t = 4.64), “bodily pain” (7.21, t = 3.66), “general health” (8.55, t = 3.27), “overall physical health” (9.48, t = 6.44), and “overall mental health” (7.29, t = 7.83). All these domains showed statistically significant improvement at the P < .001 level.
Comparison of QOL of Patients with KOA in Study and Control Group After the Intervention Posttest IV (Day 90)
(N = 200).
Abbreviations: QOL, quality of life; KOA, knee osteoarthritis; S, significant.
Discussion
The QOL largely depends upon the severity of the disease among patients with KOA who are deprived of their activities, independence in executing their works, and mobility. It is common that those who suffer from KOA develop a sense of helplessness as they get their functional abilities shrunk, besides experiencing poor QOL. QOL has a direct link with functional independence; the more functional independence, the higher QOL (23). Therefore, early diagnosis and proper implementation of intervention can help the patients with KOA to find relief and improve their QOL.
Our study reported that there was an improvement in the QOL (physical functioning, role physical, role emotional, vitality, mental health, social functioning, bodily pain, general health, overall physical health, and overall mental health) of patients with KOA in all domains in the study group after the nurse-led intervention. Consistent results have been reported in a study conducted by Coleman et al (24). The study determined the effectiveness of health care professionals-led self-management education programs on the level of pain and QOL of patients with KOA. The results showed that the health care professionals led self-management education program reduced the pain score and improved QOL in physical function, role physical, body pain, vitality, and social functioning domains, as well as hamstring strength improved in both the legs during the 6-month follow-up. Likewise, Lun et al (25) reported that the isolated hip and leg strengthening exercise programs seemed to reduce knee pain, and improved physical function and QOL of patients with KOA. The study concluded that both hip and leg strengthening exercises need to be incorporated into the exercise prescription of patients with KOA. This shows that the isometric exercise and self-management health education program improves the QOL in patients with KOA.
In order to increase the functional capacity of the patients with KOA, Al-Johani et al (15) suggested that the adaptation of strengthening exercises for hamstring and quadriceps muscles could lessen the knee pain, retain the patients’ mobility, and all other activities and ensure the QOL of the patients with KOA. Carmona-Terés et al (26) reported that a 20 h health-coaching program helps the patients with KOA in weight reduction, improving their physical activities, and maintaining a pain-free life normally. The results of our study also showed that there was a significant improvement in the QOL of patients with KOA by practicing 12-week home-based isometric exercise and counseling. Furthermore, another study performed by Akodu et al (27) also supported our study findings in which pilates and isometric exercise training for 8 weeks reduced the pain and improved the QOL in patients with KOA.
In the current study, after the intervention, the mean gain score was high in all domains of QOL in the study group at (95% CI) at posttest I, posttest II (day 30), posttest III (day 60), and posttest IV (day 90). The pretest mean was 348.67 and after the intervention, the mean was 421.11. The percentage of the mean score was 43.6 in the pretest and after the intervention, the percentage of the mean score was 52.6, and the mean difference was 72.44 in the study group, whereas in the control group, the pretest mean was 346.14 and after the intervention, the mean was 354.01. The percentage of mean score was 43.3 in the pretest and after the intervention, the percentage of mean score was 44.3, and the mean difference was 7.87. It showed that the gain score in QOL was higher in the study group than in the control group.
Our study findings are again supported by another study conducted by Yilmaz et al (28). The study adopted a home-based exercise program for hamstring and quadriceps based on isotonic and isometric exercises along with an active ROM. It was found that the home-based exercises have benefited the patients with KOA in the functional activities and improved the QOL as they felt a reduction of pain. Our study results could be generalized as a few more studies support our study findings, which increases the possibility of adopting isometric exercise and counseling in routine patient care. Saleki et al (29) observed that a 4 weeks’ acupuncture and isometric exercises program showed a beneficial effect on reduction of pain and improvement in QOL. In addition, Shakoor et al (30) reported that an 8-week home-based exercise program to strengthen the quadriceps muscles showed remarkable results in reduction of pain and increased muscle strength when assessed with an isokinetic system at the end of the treatment. Also, it improved the QOL of patients with KOA.
Osteoarthritis Research Society International recommends that a structured exercise program along with the dietary management for weight reduction could give great relief to the patients with KOA. Therefore, self-care is an important strategy including regular exercise and weight reduction which will help the patients to minimize their physical discomfort and to improve their QOL (31). The authors therefore strongly recommend the integration of isometric exercise and counseling in the routine care of patients with KOA, which will improve the functional ability and QOL of patients.
Limitation
The study limits the generalizability as the study was conducted only in two settings.
Conclusion
Nurse-led intervention including home-based isometric exercise and education increases the functional level and improves QOL in patients with KOA. This intervention requires no assistance, is home-based, cost-effective, and easily adaptable for elderly patients with KOA. Considering the benefits of isometric exercise, the elderly with KOA should regularly practice the isometric exercise to improve their functional status and QOL.
Footnotes
Acknowledgments
All the patients with KOA who volunteered to participate in this study are sincerely acknowledged.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.