
Abstract
Fifteen patients between 35 and 50 years of age, with a body mass index (BMI) over 35 with knee osteoarthritis participated in small group, facilitator-guided, interactive discussions (experience groups). Using initial inductive coding followed by deductive classification, 2 coders identified themes related to outcomes including difficulty engaging in meaningful work and social isolation in the capability realm, feelings of depression in the comfort realm, and desiring small achievable goals and consistent support in the calm realm. Themes regarding gaps in care included lack of roadmap and inadequate support. The obstacles to health were debilitating pain, despair due to isolation and stigmatization, hopelessness regarding treatment, perceived lack of clinician empathy and distrust, and frustration with the association of knee osteoarthritis with aging. Effective musculoskeletal specialty care can anticipate these patient needs, particularly for circumstances where nonoperative, accommodative health strategies are favored.
Keywords
Introduction
Background
Knee osteoarthritis is an expected aspect of human aging with no disease-modifying treatments.1,2 People that are unsatisfied with nonoperative treatments and other accommodative strategies for alleviating symptoms related to knee osteoarthritis might consider knee arthroplasty. During knee arthroplasty, the native anatomy is replaced with a metal and plastic prosthesis. The prosthesis has a limited lifespan of a few decades. Up to 20% of people develop knee osteoarthritis before age 50. 3 It is unwise to perform arthroplasty in people younger than age 50 who have a life expectancy much longer than the durability of the prosthesis. The most effective and appropriate options in this age group may be a healthy weight, exercises, and a healthy mindset and circumstances to bolster accommodation.4-6 Obesity is associated with higher levels of discomfort and incapability related to knee osteoarthritis 7 and may accelerate deterioration of the arthritic knee.8-10 As an additional consideration, even a technically sound knee arthroplasty does not result in satisfactory levels of comfort and capability for up to 1 in 5 people. 11 This suggests that current care strategies may be incomplete.
Rationale
Patients living with a given condition are arguably the most important source of knowledge about what is working and what can be improved in current health and care strategies. 12 Prior qualitative studies among people living with knee osteoarthritis identified themes of struggle to adapt to normal routines, lack of accessible information for future planning, limited understanding of osteoarthritis pathology, frustration, and anxiety managing the disease among younger patients, and an experience of social stigma such as walking aids marking them as someone who is impaired.13-17 Many of these themes apply equally to relatively young patients of any weight. We sought to better understand the specific experience of relatively young, obese people seeking care for knee osteoarthritis, one of the most challenging demographics given the issues related to arthroplasty in younger patients and the benefits of a healthy weight in the accommodation of symptoms.
Experience groups are a specific type of focus group that emphasizes interaction between the participants over interaction with the moderator. Discussions catalyzed by shared experiences of people living with a disease have the potential to uncover themes that might remain dormant with the central authority of the moderator.
The goal of health strategies for relatively young, obese adults with knee osteoarthritis is enhanced alleviation of discomfort and incapability and a good experience of care. The capability, comfort, and calm framework introduced by Teisberg and Wallace emphasizes these key aspects of health and care. An analysis of experience group findings in this framework has the potential to inform the care of people with uniquely challenging illnesses such as knee osteoarthritis.
Questions
We facilitated conversations among people with KOA (experience groups) aged 35 to 50 years with a body mass index (BMI) over 35, identified themes using the capability, comfort, and calm framework and sought to better understand: What matters most, based on lived experience, to people aged 35 to 50 with a BMI over 35 seeking care for knee osteoarthritis? What are the gaps in care? What are the obstacles to health?
Methods
Study Design
This study was approved by our Institutional Review Board. Experience Group sessions are a qualitative research method designed to gather insights from patients who share specific medical and life circumstances. Experience Groups are a type of focus group where facilitators generate discussion of shared experiences among the participants, as opposed to more typical focus groups where the attention is often on the moderator.
Those insights typically center on the health outcomes that matter most to the patients, and the gaps or obstacles that may impede achievement of those outcomes. The sessions are designed to collect information on 3 dimensions of health: capability (ability to perform one's daily tasks and to achieve one's goals), comfort (alleviation of physical or mental symptoms), and calm (limitation of inconvenience and stress related to receiving care).5,18
Patients aged 35 to 50 years, with a body mass index of 35 or greater, diagnosed with KOA who visited our specialty unit within the prior year were identified using billing and medical records. The diagnosis of knee osteoarthritis was made based on interview and examination and confirmed with radiographs. Identifiable health information was limited and maintained on password-protected servers. We used purposive sampling, identifying people matching the inclusion criteria, and invited eligible participants via phone calls but did not track those who declined participation. We recruited 15 people with diverse backgrounds willing to participate, 4 of whom spoke Spanish. English speakers participated in 3 sessions and 2 individual interviews. Four Spanish speakers participated in one Experience Group session. We did not collect detailed demographic data such as age, gender, race and ethnicity, income, education, or comorbidities, as the Experience Group methodology emphasizes the shared lived experiences of participants over categorical demographic distinctions. The aim was to understand common patients’ narratives that may be overlooked in more conventional data-driven or clinician-centered approaches.
In small group sessions lasting between 60- and 90-min, people with a similar medical condition have a moderated conversation regarding daily experiences, concerns, hopes, and goals. For this study, 2 PhD-educated, trained facilitators encouraged discussion among the group regarding their experiences of care and life in general with their condition. The focus was on the daily experiences that are typically less observed by clinicians. Spanish language experience groups were facilitated and coded by a PhD researcher and bilingual native Spanish speaker.
An established methodology was used to foster conversation in the group, intending to bring to light issues of concern that may not be raised in clinical encounters. A facilitator used a semi-structured interview guide to introduce specific topics for discussion, in the form of open-ended questions or possible discussion themes. Facilitators were not previously known to participants and were not directly involved in their care, which encouraged open sharing and reduced the influence of perceived clinical hierarchy. The facilitators focused on enabling participants to self-select the moments and experiences they found most meaningful, allowing new or unarticulated concerns, experiences, and themes to surface naturally. This Experience Group was designed for groups of participants to speak with one another, rather than primarily responding to a moderator, and ultimately create comfort and validation through shared experiences. Notes were taken and the sessions were audio-recorded and transcribed verbatim. Participants did not review the transcripts.
Analysis
The transcripts of the sessions and interviews were coded by 2 researchers using NVivo (QSR International; Melbourne, Australia) identifying themes and subthemes inductively. The themes were analyzed in the context of the Capability, Comfort, and Calm framework to better understand unmet needs and obstacles to health. 18 Discrepancies interpreting the themes were resolved in discussion by the researchers, including the principle investigators.
Results
Living with Knee Osteoarthritis
Capability
One theme that emerged was that patients expressed a deep desire engage in work in a meaningful way (Table 1). They sought productive work in order to feel useful.
Representative Quotes—Living With Osteoarthritis of the Knee.

A second theme was having a rich social life. Patients see success as regaining their youthfulness and engaging socially with friends and family.
The third theme was moving freely with less pain. Patients want to go about their lives completing ordinary tasks without feeling excruciating pain.
Comfort
There was one theme in the comfort domain (Table 1). Participants reported that feelings of despair (depression) characterized the condition of KOA as much as the physical pain. They long to look to the future with hope.
Calm
Patients with knee osteoarthritis seek care that has clear and achievable health goals (Table 1). They desire concrete solutions and short-term benchmarks that seem attainable.
Many participants also expressed desire for a plan that provided consistent support and hands-on care that was incremental enough to seem achievable.
Obstacles to Health
Several themes regarding challenges that keep people from achieving health were identified (Table 2). Key themes are that the pain of knee osteoarthritis can be excruciating and that some patients are hesitant to use pain medication. There are patients who state that they want opioids but feel judged. Other themes are that social isolation increases despair, that patients feel hopeless about the treatment, and that there is a perceived lack of empathy from clinicians. Additionally, the association of osteoarthritis with age can lead to feelings of frustration, such as always hearing, “you’re young to have arthritis.” Other themes are that healthy living seems too expensive and some distrust of physicians.
Representative Quotes—Obstacles to Health.

Gaps in Care
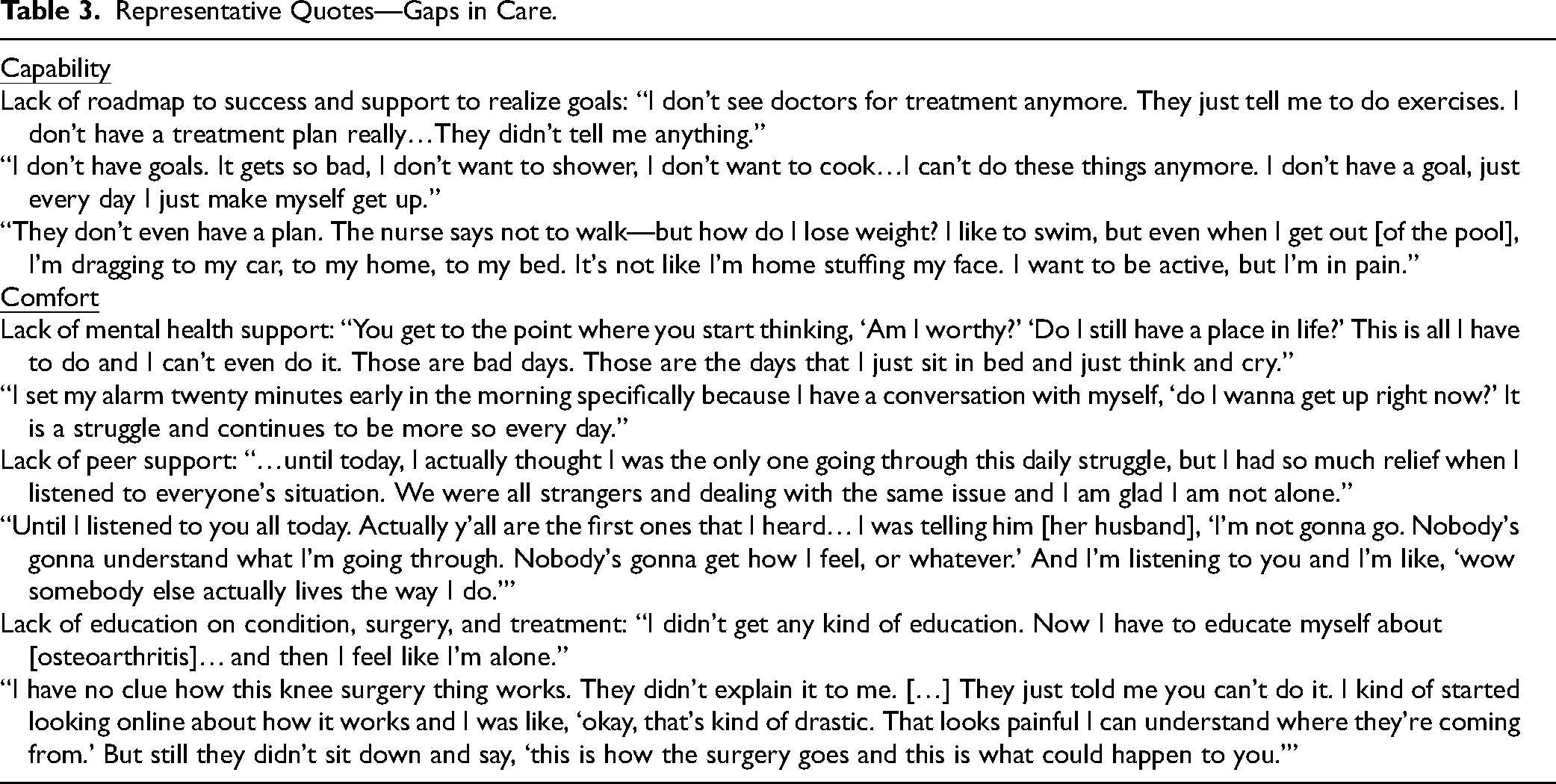
Some of the Experience Group participants said the care they received did not include a roadmap to success and support to realize goals, mental health support, peer support, or education on the condition and treatments (Table 3).
Representative Quotes—Gaps in Care.
Discussion
A study of patient experience and priorities can be used to tailor effective and soothing care. People with a shared illness may, together, elucidate their desired outcomes and the unmet needs in realizing these outcomes. Care teams can use this information to consider improvements in strategies, collaboration, and coordination. For relatively young, obese patients with KOA, the themes identified may be underappreciated in musculoskeletal specialty care: meaningful work, community, direction, and hope.
There are limitations of this research to consider. First, we depended on people with motivation and time to volunteer. Additional Experience Group sessions to accommodate patients who might not typically participate have the potential to identify additional themes. A qualitative study does not address the prevalence or frequency of themes or their association with capability, comfort, and care-seeking behavior. The frequency of themes is not typically reported in qualitative research because the small sample cannot provide reliable and accurate quantitative evidence. The smaller sample is sufficient to reach theme saturation, but not enough to generalize rates or associations, nor to associate specific themes with specific patient characteristics. However the sentiments and experiences identified have face validity, support from other evidence, and can be considered common and important themes.10,19-21
Living with Knee Osteoarthritis
Themes regarding living with KOA included reduced mobility and difficulty with work and social roles in the capability realm; despair in the comfort realm; and seemingly unachievable goals and lack of support in the calm realm. The theme of interference with social roles and social isolation, identified in 2 other qualitative studies of participants younger than 65 years of age with KOA22,23 emphasizes the central aspect of loss of cherished identities and relationships. One aspect of good health as we age is evolution of our narrative identity and social interactions to match our bodies. The theme of despair, also noted in prior studies—anticipation of progression and confronting the ageing process in particular16,17—highlights how difficult and draining this process can be. There is a need for care strategies to address the whole person. Not just the arthritic knee, but the feelings and thoughts associated with the associated sensations. 16 There is a notable relationship between levels of discomfort and incapability and both levels feelings of despair and insecurity and distorted thinking (common misconceptions) among both people with radiographic knee arthritis the general population, many of whom are not seeking care 2 and, even more strongly, among people seeking specialty care for knee osteoarthritis. 24 Specialists may tend to organize care around the pathophysiology: identify a pathophysiology, direct treatment towards the pathophysiology, assess the alleviation of symptoms, and then consider another treatment directed at the pathophysiology. For instance, we might start with exercises, then move to a corticosteroid injection. Then—even though we know there is no way to slow or reverse osteoarthritis (no disease-modifying treatment)—we may then describe patient dissatisfaction with symptomatic (palliative) treatment as having “failed,” which points to surgery as the ultimate success. 25 Given that we know that arthroplasty is also frequently unsatisfying, this formulation needs to change. 26 Qualitative studies like ours suggest we might prioritize validating a person's story (narrative medicine 4 ); empathetic noticing and legitimizing of patient concerns so that they feel heard and understood (relationship building); and guiding, rather than directing, people to healthier thoughts and feelings about KOA (motivational interviewing techniques). The lack of treatments that can alter the natural history of osteoarthritis can also direct our attention to these tactics for bolstering effective accommodation. These have the potential to improve health with or without a choice for salvage reconstructive surgery in the form of total knee arthroplasty.
Obstacles to Health
The identified barriers to health among people who seek care for KOA—including incapability related to pain avoidance, hopelessness regarding treatment, social isolation that increases despair, perceived lack of clinician empathy, frustration with aging and knee osteoarthritis, high costs of healthy living—suggest a need for more effective communication and care strategies that help rework an unhealthy inner narrative about one's changing body and guide people to new or adjusted roles. The themes related to pain alleviation—as noted in themes such as hesitancy to use pain medication and feeling judged for seeking opioids—may, in our opinion, represent a type of passivity or externalization of health. They may also represent a false hope that aging of the body can be avoided. Both of these possibilities point to important opportunities to guide people to a more active, matter-of-fact approach to their health (Greater Personal Health Agency). 17 Patients may not realize that medication can only alleviate symptoms and that healthier mindsets alone can be an effective pain alleviator. The sense that medication might be disease-modifying and that health lies external to oneself is capture in themes—noted both in this study and by others—of limited medication efficacy, impersonalized care, and lack of motivation to perform therapeutic exercises.19,27 The themes of not wanting to take medications, feeling medications are ineffective, and lack of motivation to do exercises merit additional investigation. It might be a way of saying, “I want this problem fixed,” or “I can’t be myself with knee pain.” Essentially, “I don’t want to alleviate or accommodate this problem. I want to eliminate it.” This is a common unhelpful thought that is notably associated with greater discomfort and incapability.17,20,27-29
The theme of distrust of physicians may be the most important obstacle to good health given that clinician guidance towards healthier inner narratives and renewed roles might, at times, feel negating or dismissive of the patient's concerns. This linkage of expressed hopelessness regarding treatment, unhelpful fear about the impact of KOA on daily and social life, and dissatisfaction with clinicians was noted by others.30,31
Gaps in Care
The finding that many participants regarded their care as directionless, poorly understood, and lacking support (including mental health and peer support) directs us to develop health strategies based on incrementable, achievable goals to help develop trust, confidence, and collaboration. One potential intervention is easier access to specialty expertise via asynchronous text, email, or medical record-based communication portals, as well as frequent chat, audio, or video check-ins. An increased number of touchpoints with clinicians might help to improve the patient-clinician relationship, and trust in particular, which is often lacking based on the experiences documented herein. Increasing the number and types of access specialty care and making communication more convenient for patients might also help them to feel more cared for and help them process complex health information and build healthier habit incrementally. Another potential intervention, suggested by others, could be group-based exercise programs and peer support to adopt weekly exercise habits and greater personal health agency. 32 Interventions like these could improve social support and reduce feelings of shame. 33 A goal of these and other interventions can a healthier patient regard for KOA and increased perception of useful advice on a treatment plan. 21 Many of the gaps in care noted in the current and in prior studies point to the opportunity of interdisciplinary, team-based care. A team member, such as a physical therapist, health coach, or social worker could be introduced at the first visit and then keep in touch with the patient regularly to support progress.
Key Takeaways
Based on the collective qualitative evidence from this and other studies, we offer the following thoughts about potential evolutions in musculoskeletal specialty care. Given the prevalence of knee osteoarthritis and its successful accommodation documented in population-based studies, 2 it's likely that many people manage without specialty care. Patient-facing information can be crafted to enhance the accommodation of an aging knee and increase personal health agency. For people who do seek specialty care, the existing qualitative evidence suggests that the patient–clinician relationship deserves priority. Validation of frustration and despair and gentle incremental reorientation of common misconceptions are skills that benefit from training and practice that many specialists lack. It may help to guide people to a healthier understanding of KOA in increments, separated by time, providing adequate time to absorb and reflect on information that is unexpected and counterintuitive. For instance, a first visit might describe the anatomy and age-associated changes. Patients might be given something to read or watch to build their understanding and gently correct common misconceptions such as new pains represent injury34-36 and painful activity will make the problem worse. 28 When ready, they can learn a few simple exercises to do on their own. The goal is for the care to feel warm and ongoing. Another check-in a few days later, by phone, video, or in person, could allow people to ask questions, express emotions about what they are learning about their body and reinforce that (painful) exercises are helpful rather than damaging. This approach can guide people away from tests and treatments with low potential for benefit and towards more effective health strategies.
Conclusions
The importance of mental and social health is evident in the perspective of relatively young, relatively obese people seeking specialty care for KOA, a population for whom arthroplasty is unwise, making the need to enhance accommodation of the condition more pressing. The traditional biomedical algorithm of pills, shots, exercises, and surgery may bypass the despair, loss of identity, loneliness, and aimlessness that patients are experiencing. These universal features of human illness represent modifiable factors that can alleviate discomfort and improve capability. The evidence is mounting that these factor merit greater attention in musculoskeletal specialty care.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors certify that they have no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article. David Ring (DR), or a member of their immediate family, has or may receive payments or benefits, in any one year, from Skeletal Dynamics for an internal joint stabilizer elbow in the amount of between 10 000 and 100 000 USD per year, that he (DR) is a Deputy Editor for Clinical Orthopaedics and Related Research® and has received or may receive payments or benefits in the amount of USD 5000 per year. One of the authors certifies that he (DR) received honoraria from various universities, professional associations, and continuing medical education vendors.
Ethical Approval
All procedures in this study were conducted in accordance with our Institutional Review Board's (2018-04-0132) approved protocols. This work was performed at Department of Surgery and Perioperative Care, Dell Medical School at The University of Texas at Austin, Austin, TX, USA 1601 Trinity St., Bldg. B, Stop Z0800 Austin, TX 78712.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with our Institutional Review Board's (2018-04-0132) approved protocols.
Statement of Informed Consent
Verbal informed consent was obtained from the patients for their anonymized information to be published in this article.