
Abstract
Family members often act as surrogate decision makers for patients in the intensive care unit (ICU). The use of printed prompts may assist with families feeling empowered to fulfill this role. Prospective, randomized controlled trial in 3 ICUs in Western Australia. In the intervention arm, families received the Choosing Wisely 5 questions as printed prompts prior to a family meeting, and the control arm did not receive prompts. The primary outcome was family perceived involvement in decision-making. Outcomes were measured using a survey. Sixty families participated in the study. The majority of families (87.1% control, 79.3% intervention; P = .334) reported feeling “very included” in decision-making. There was no difference in secondary outcomes, including minimal uptake of the questions by the intervention arm. This has been the first randomized trial evaluating the use of a decision-making tool for families in the ICU. Despite ceiling effects in outcome measures, these results suggest room for future study of the Choosing Wisely 5 questions in the ICU.
Introduction
The intensive care unit (ICU) patient is unique in that they often cannot engage in effective communication with ICU staff and make decisions regarding their own health. Families commonly act as surrogate decision makers for the ICU patient and will frequently meet with the ICU staff to receive updates and information, discuss the trajectory and goals of treatment, and relay information regarding the patient's wishes.
During a stressful time, families may struggle to process the technical information being delivered to them while also trying to integrate the ICU patient's values and wishes into their decision-making (1). It has been shown that communication with families in this setting has much room for improvement, with over half of ICU patients’ families displaying poor comprehension of the patient's diagnosis, prognosis, and treatment (2). Communication with ICU patients’ families often occurs during a family meeting with the ICU doctor and nurse. Family satisfaction with meetings is improved by allowing family members more time and opportunity to speak during the meeting (3). Family interaction and involvement has been advocated as an important aspect of effective communication during these meetings (4–6). Despite a number of studies identifying the needs and preferences of families and surrogate decision makers in the ICU, these needs are not universally met and ongoing focus in this area is paramount to improving family satisfaction (7,8). There remains to be room for improvement in the communication of ICU staff with families and how they provide information and emotional support (9,10).
A number of strategies have been employed in ICUs to improve communication during family meetings, including family information leaflets, guidelines for doctors leading the meetings, timed care bundles, nursing-led family discussions, and training in family communication (11–21). Of those studies that did focus on family members, the use of family information leaflets was found to improve family comprehension (11,13,14). However, family involvement in decision-making was not evaluated (11,13,14). To date, there has not been a randomized trial investigating an intervention that targets the family in the ICU and tests their perceived involvement in surrogate decision-making.
The Choosing Wisely campaign promotes consumers and healthcare professionals working together to enable the consumers, in this case, the families of patients, to make informed decisions that suit their preferences and personal circumstances (22). The Choosing Wisely 5 questions (see Online Appendix 1) allow patients or their families to question the care planned or being implemented (23). The simplicity and readability of the Choosing Wisely 5 questions make them suitable for all levels of health literacy. The questions appear easily adaptable to the ICU context, related to issues that commonly arise in the ICU family meeting and have crossover with a question list identified in the literature that suggests 21 questions that are considered important by both families and doctors (24).
The primary aim of this study is to determine whether the use of the Choosing Wisely 5 questions in family meetings in the ICU improves the level of family perceived involvement in decision-making.
Methods
Trial Design
This is a 2-arm, prospective, randomized controlled trial.
Participants and Setting
Participants were families acting as surrogate decision makers on behalf of ICU patients from 3 ICUs in Perth, Western Australia. Medical and nursing staff involved in the family meeting in question were also participants in the study.
The inclusion criterion was any family member/s who were to attend and participate in a family meeting with the ICU doctor. The family member who was most likely to act as the patient's surrogate decision maker was asked to complete the post-family meeting survey.
The exclusion criterion was family member or patient age less than 18 years. Families were identified as potential participants if the ICU doctor was planning to have a family meeting with them that day. Family member/s were approached by an ICU doctor and invited to participate in the study prior to commencing the family meeting.
Intervention
On agreeing to participate, the family member/s received an envelope containing documents that allocated them to either the control or intervention group. The envelopes were prepared by the study lead author who was independent of the family meeting and did not attend the family meeting.
Intervention participants were given the Choosing Wisely 5 questions and an explanation of how to use them as prereading (see Online Appendix 2). The family member/s were able to take the prereading document into the family meeting to refer to if they wished. The control group was given a document stating that they had no prereading to complete and that they would participate in the family meeting as per usual operating practices (see Online Appendix 3). There was no specified duration for the pre-reading. The ICU doctors were advised to allow families adequate time to complete their prereading. They allowed the families to complete the reading at their own pace and were available for questions if required.
Outcomes
Outcome measures were assessed via completion of surveys by a representative of the family, the most senior medical representative involved in the meeting, and a nurse participating in the meeting (where applicable) (see Appendices 4-8). All 3 surveys were assigned a study number enabling them to be linked for statistical analysis.
The survey questions were adapted from the Family Satisfaction with Care in the Intensive Care Unit (FS-ICU 24) survey (25). This is a validated tool for assessing various markers of family satisfaction with regard to patient care in the ICU. The family survey included 4 questions from the “Process of Making Decisions” section of the FS-ICU 24 (25). The primary outcome was measured with the survey question “did you feel included in the decision making process?”. Responses were scored from one to 5 on a scale ranging from “I felt excluded” to “I felt very included.”
The secondary outcomes were: how well supported families felt (5-point scale); whether families felt they received an explanation/s that they understood (5-point scale); and whether families felt they had adequate time for decision-making (2-point scale).
The ICU doctors and nurses were asked to report on the uptake of the Choosing Wisely 5 questions, whether the use of the questions was helpful and whether the use of the questions slowed the meeting. The ICU staff were also asked to report on whether or not a goals-of-care discussion had taken place and form had been completed.
The participant families, ICU doctors, and nurses were all asked to detail what they believed to be the most important message communicated in the family meeting and to provide any additional comments that they felt were relevant.
Sample Size
It was hypothesized that for the primary outcome, perceived involvement in decision-making by surrogate decision makers in the ICU, the intervention would improve the baseline level from 50% to 80%. This statistical improvement was derived from previous studies (11,12). With an α level of .05, and power of .8, this gave a sample size of 72 patients (2-sample comparison of proportions). The baseline level of 50% is based on the Azoulay et al study in 2000 which described that only 50% of families in the ICU experience adequate communication with ICU physicians (2).
Randomization
Randomization of participants was via a computer-generated random number generator on Microsoft Excel. Participants were allocated by simple randomization. The allocation of the family member/s was concealed from the ICU doctor recruiting the family. The study prereading and post-family meeting surveys were contained within a sealed envelope that did not reveal study allocation on the outside. The contents of the envelopes were only revealed once the family had agreed and consented to participate in the study. Families provided written consent. Given their high levels of health literacy, thorough understanding of research and previous involvement in survey studies, willingness to complete the survey was deemed implied consent for the ICU doctors and nurses participating in the study.
Blinding
The ICU doctor and nurse participating in the family meeting were blinded to study allocation prior to the family meeting commencing. The family, however, was able to take the prereading into the meeting to refer to. Therefore, no one was blinded to allocation once the meeting had begun.
Statistical Methods
Data were summarized using frequency distributions for categorical variables and means (standard deviations) for continuous demographic variables. Categorical group comparisons were made using χ2 or Fisher exact tests, as appropriate for low cell counts, and t tests for continuous group comparisons. Stata version 16.0 (StataCorp) was used for data analysis. The qualitative data provided by study participants were grouped into themes and summarized using frequency distributions.
Results
Participant Flow
Of the 72 families who were approached to participate in the study, 12 did not complete the documentation and consent. Therefore, 60 families were included in the final dataset. Given that the study had completed data collection and moved on to the data analysis stage, data collection was not repeated to recruit a further 12 families. All study participants received the intended intervention.
Recruitment
The majority of participants (71.0% control and 79.3% intervention) were recruited from a tertiary ICU in metropolitan Perth. Data were collected over a 19-month period, from May 2019 to December 2020. Thirteen ICU doctors with experience conducting research were involved in recruitment for this study, including the lead author and 2 coauthors (AD, MA, BW). All ICU doctors received training in recruitment procedures, including suggestions for standardized wording to support recruitment and consent, and were able to contact the lead author at any time during the consent process if required. Recruitment rates varied between ICU doctors, with 45% recruitment completed by study authors and 55% by nonstudy author ICU doctors.
Baseline Data
The demographic characteristics of the patients for whom the families were acting as surrogate decision makers were collected and are listed in Table 1. There were no significant differences between the control and intervention groups in baseline demographics.
Characteristics of ICU Patients.
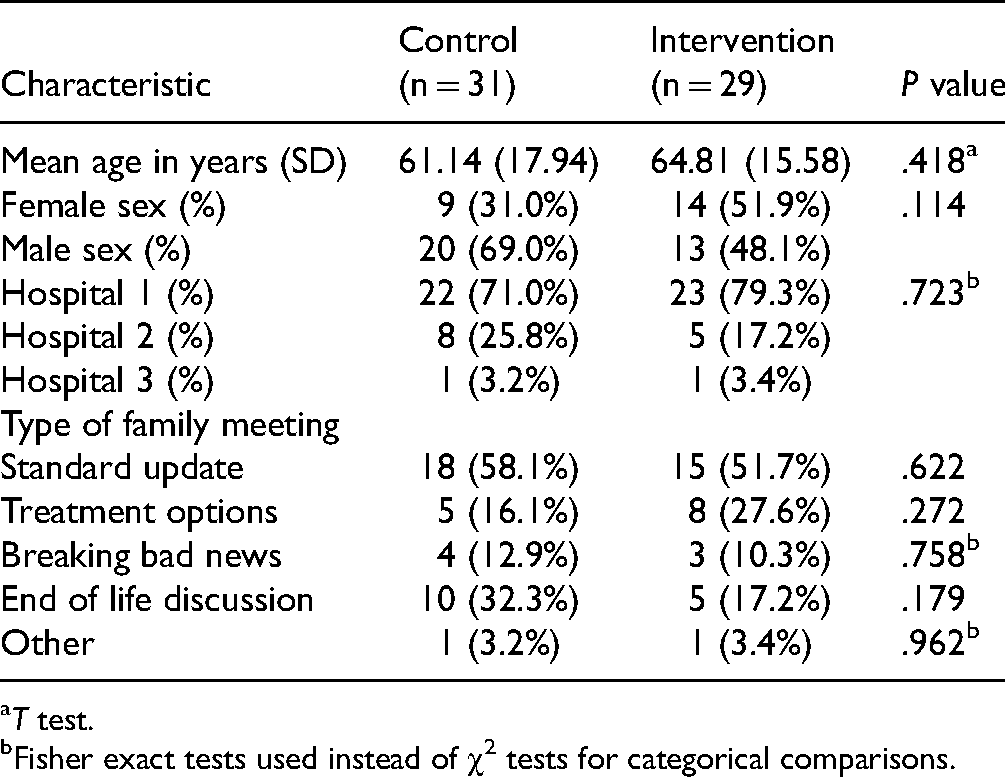
T test.
Fisher exact tests used instead of χ2 tests for categorical comparisons.
Outcomes
The results from the surveys completed by family members are listed in Table 2. The majority of families (87.1% control, 79.3% intervention; χ2 (3, N = 60) = 3.40, P = .334) reported feeling “very included” in decision-making during their family meeting, with no significant difference between intervention and control groups. All families reported that they had adequate time spent on their concerns and questions during the meetings (χ2 (1, N = 60) = 0.43, P = .514).
Responses to Family Survey.

Fisher exact tests used instead of χ2 tests for categorical comparisons.
Across intervention groups, both the ICU doctors (χ2 (4, N = 60) = 7.80, P = .099) and nurses (χ2 (4, N = 60) = 5.56, P = .234) reported that the majority of families were included in the decision-making process (see Table 3).
Responses to Medical and Nurse Surveys.

Fisher exact tests used instead of χ2 tests for categorical comparisons.
The Choosing Wisely 5 questions specific survey responses from ICU doctors and nurses are listed in Table 4. There was a low uptake of the use of the Choosing Wisely 5 questions by families allocated to the intervention group. The ICU doctors reported that 24 families (82.8%) and the nurses reported that 17 families (68.0%) did not utilize the questions from the prereading in the family meeting. The ICU doctors and nurses both reported that family use of the questions did not alter the duration of the meeting.
Responses From ICU Doctors and Nurses Regarding Family Use of the Choosing Wisely 5 Question by Families in the Intervention Group. a
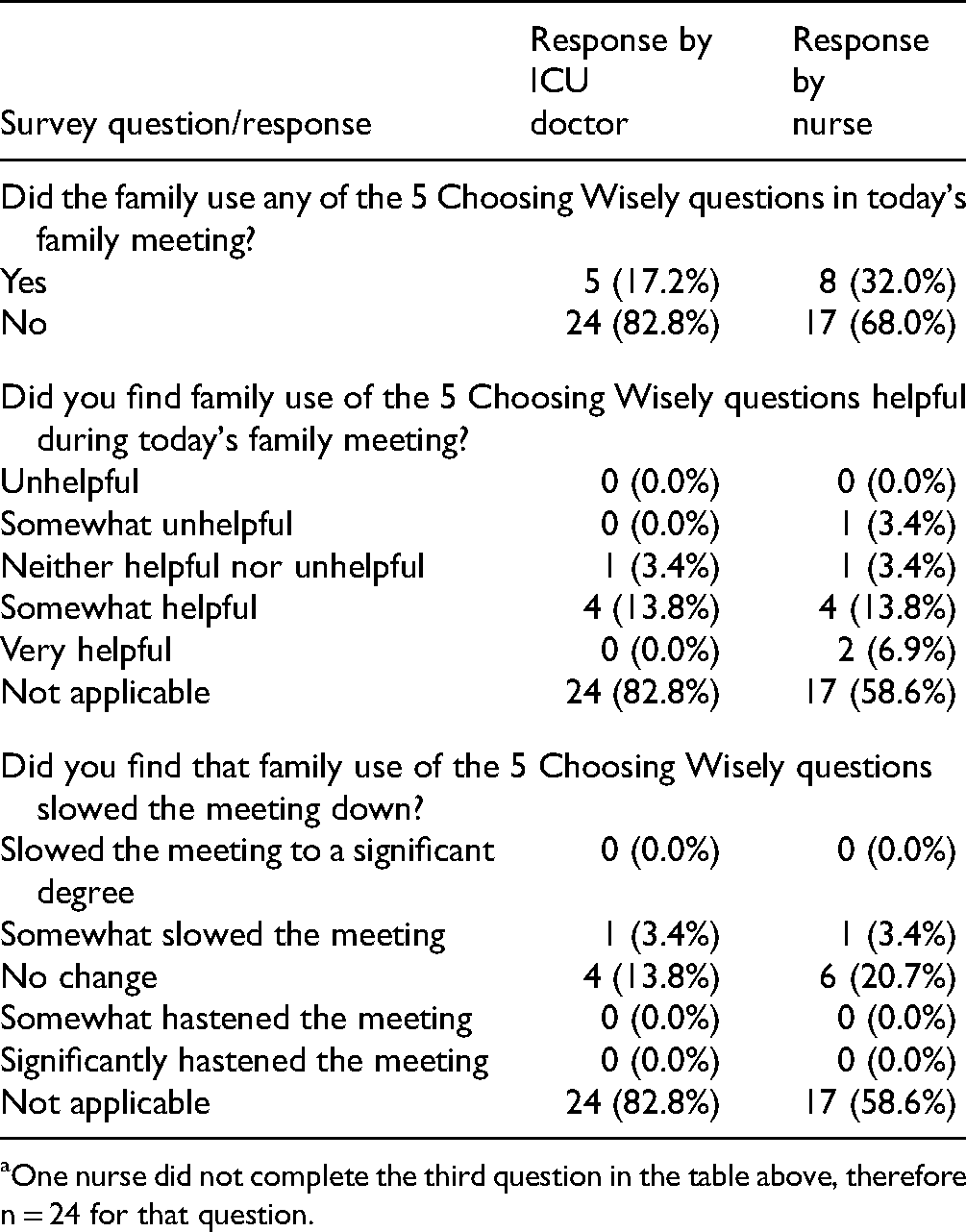
One nurse did not complete the third question in the table above, therefore n = 24 for that question.
The “free text” questions were answered by a minority of participants (36.67% for “what do you think the most important message was from today's family meeting?” and 5.00% for “comments”). Of the participants who provided answers to the qualitative questions, the most important messages conveyed were regarding short-term prognosis and plans, long-term prognosis and plans, reassurance and support for the family, and information on the patient's current status. A minority of families responded that the most important message was regarding the ICU patient's values and wishes being addressed, ability for the family to ask questions, and the patient's goals of care.
Discussion
Study Findings
This is the first randomized controlled trial to assess the utility of the Choosing Wisely 5 questions in the intensive care setting. The provision of the Choosing Wisely 5 questions as prereading, as compared to no prereading, was not associated with any significant change in the families’ perceived involvement in decision-making. Despite this, families gave positive feedback regarding the meetings and the majority felt very included in the decision-making process.
The findings from this study are in line with the results of previous research that showed no difference in family satisfaction with the introduction of question lists prior to family meetings (12). It may be that communication and provision of information to families by ICU doctors in the units studied are already of a high standard. This supposition is reflected by the presence of a nurse in most family meetings, a quality metric of family meetings in the ICU itself (26). There were also high levels of family inclusion in the family meetings and almost all families felt that they had adequate time spent with them during the meetings. As such, this study may have been underpowered to reflect a significant difference between the intervention and control groups.
The lack of significant differences between groups is also likely influenced by the low uptake of the Choosing Wisely 5 questions by families in the intervention arm. The questions may have been underused if the families felt that the information covered in the family meeting was sufficient and they did not need to ask further questions. This is reflected in the positive responses from participants regarding the quality of communication within the family meetings. The families may, however, have benefited from an ICU staff member guiding them through the prereading to ensure comprehension to optimize uptake. There is also a possibility that ICU doctors and nurses underestimated prereading of the Choosing Wisely questions by families, particularly if the family worded their questions and concerns differently. Future studies in this area could consider audio recording family meetings to accurately gauge the use of specific questions by families.
Reassuringly, the majority of families felt that they had adequate time during the meeting to have their needs addressed. Future work in this space could explore the proportion of family speech, number of questions asked, quality of doctors’ answers to family questions, and how the doctor imparts information as important outcomes in this context (27).
Strengths and Limitations of the Study
There are several factors to consider in interpreting the results of this study. Anecdotally, some ICU doctors reported that when they were perhaps embarking on a “difficult” family meeting (due to preexisting conflict, language barriers, or family disharmony), the added burden of consenting the family for the study may have been a barrier to recruitment. Furthermore, when the work environment was busy and clinicians felt rushed this may have precluded them from remembering to recruit. Paradoxically, perhaps these “difficult” meetings may be those that would benefit more from a communication tool beforehand. This element of the recruitment phase contributes selection bias to this study. Without randomization, this might not have occurred. However, the methodology would not have been as robust.
This selection bias is reflected in the long time taken (19 months) for 3 ICUs to recruit 72 families to the study, despite the study taking place in busy units that likely had frequent family meetings. In addition, the study did not actually reach its planned statistical power, as not all the enrolled patients completed all the surveys and consent forms, and the power calculation may have been optimistic given the overall high satisfaction in the control arm with family involvement.
Bias may also have been introduced by ICU doctors performing the family meetings with regard to their survey responses. The doctors are unlikely to be completely impartial in their responses given that they are providing feedback, albeit anonymous, on their own performance when answering, “did you feel the family were included in the decision making process?.”
Future Work
An ideal tool for future research in this area would be an on-site research coordinator who could fulfill the roles of approaching all families and therefore ensuring unbiased recruitment, optimizing completion of consent forms, guiding the families through the prereading to ensure comprehension, timing the prereading period, timing the family meeting, and encouraging completion of the post-meeting survey or completing a post-meeting interview.
Given the ceiling effect of the findings, it would also be helpful to obtain specific information from ICU families prior to introducing a targeted intervention. Interviews or free-text surveys may reveal precise areas where ICUs can improve communication during these crucial family meetings, allowing an intervention that hones in on such areas.
Despite this study not producing significant findings with regard to the Choosing Wisely 5 questions in the ICU family meeting context, the study biases mean that future researchers should not infer that the 5 questions were unhelpful. Unmeasured baseline demographics, such as socioeconomic status, education and health literacy, as well as unmeasured outcomes, such as duration of family meetings, number of meetings, type of decision-making required, and emotional support required may all add important nuance to this field.
Conclusion
Provision of the Choosing Wisely 5 questions, adapted to the ICU setting, to families prior to a family meeting did not improve participant, doctor, or nurse perceived family involvement in decision-making. Families with access to the premeeting reading did not report improved levels of support by the ICU staff, better explanation/s, or time spent with them during the meeting. A number of study limitations, namely selection bias, may explain these findings.
Despite these findings, there is certainly an opportunity for further study in this area. It is anticipated that future work may need to question Australian families of ICU patients regarding their needs and wants following family meetings and tailor interventions/s from there. The overarching goal remains unchanged—to improve communication with families and support them during their time as surrogate decision makers on behalf of our ICU patients.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221092623 - Supplemental material for Integrating the Choosing Wisely 5 Questions into Family Meetings in the Intensive Care Unit: A Randomized Controlled Trial Investigating the Effect on Family Perceived Involvement in Decision-Making
Supplemental material, sj-docx-1-jpx-10.1177_23743735221092623 for Integrating the Choosing Wisely 5 Questions into Family Meetings in the Intensive Care Unit: A Randomized Controlled Trial Investigating the Effect on Family Perceived Involvement in Decision-Making by Ashleigh Drury, Danielle M Muscat, Bradley Wibrow, Angela Jacques, Matthew Anstey in Journal of Patient Experience
Footnotes
Authors’ Note
This study was approved by the Quality Improvement Head of Department at the North Metropolitan Area Health Service (GEKO # 32792) and the St John of God Health Care Human Research Ethics Committee (# 1631). All procedures in this study were conducted in accordance with the Quality Improvement Head of Department at the North Metropolitan Area Health Service and the St John of God Health Care Human Research Ethics Committee approved protocols. Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article. The datasets generated and analyzed during this study are available from the corresponding author on reasonable request. The code utilized by this study is available from the corresponding author on reasonable request. Written informed consent was obtained from all participants included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.