
Abstract
Introduction
The patient–clinician relationship is evolving from physician directives (paternalism) toward a partnership between patients and clinicians.1–3 There is evidence that patient involvement helps create health strategies that are both better aligned with preferences and values3,4 and also associated with greater treatment adherence resulting in improved outcomes.5–7 There is also evidence that patient involvement is associated with better patient experience. For instance, a study of 130 patients with nontraumatic painful upper extremity conditions addressed 8 shared decision-making elements including the agreement on an action plan found that 22% of the variation in patient satisfaction was determined by the shared decision-making element of “identifying choice” and lower health anxiety. 8
Rationale
Other factors may account for part of the association between participation in decision and satisfaction with care (mediations) or they might accentuate or attenuate the association (moderation). For instance, there is evidence that more limited health literacy is associated with greater dissatisfaction and lower adherence to treatment.9,10 And greater symptoms of depression are associated with more limited activation (involvement in care),11,12 adherence, and satisfaction with care.6,13 Finally, the availability of practical, emotional, and informational support 14 from family, friends, healthcare providers, and community resources can help patients navigate health challenges and enhance their well-being.15–18 Given these relationships, it is plausible that the relationship between greater perceived involvement in decisions and greater satisfaction with care might be mediated (partially explained) or moderated (accentuated or attenuated) by greater health literacy or informational support, and fewer symptoms of depression. A finding of mediation or moderation could lead to strategies for improved patient experience by addressing health literacy, information support, or symptoms of depression. A finding of no mediation or moderation might direct efforts to improve patient experience away from these factors.
Among a cohort of people seeking musculoskeletal specialty care, we analyzed the moderation and mediation effects of health literacy, informational support, and symptoms of depression on the relationship between patient-rated involvement in decisions and satisfaction with care. Our primary null hypothesis was that health literacy does not mediate or moderate the relationship between patient-rated shared decision-making and satisfaction, controlling for other factors. In secondary analyses, we sought mediation and moderation effects of informational support and symptoms of depression.
Materials and Methods
Study Design and Setting
Upon obtaining Institutional Review Board approval for this cross-sectional cohort study, we prospectively enrolled consecutive 130 new adult patients presenting to 3 private practice orthopedic specialty offices in a large urban area over a 4-month period across a range of orthopedic subspecialties. The pace of enrollment was determined by the availability of researchers and priority of other studies. We included all new English-speaking patients between 18 and 89 years old, who were fluent in English, and who were able to provide informed consent. Patients with cognitive deficiencies that would preclude the completion of questionnaires were excluded. We did not collect identifying information. After a new patient office visit, potential subjects were invited to complete a survey by a research assistant not involved in care; completion of the survey implied informed consent.
Among the 130 study subjects, 81 were women (62%) with an average age of 56 years (Appendix 1). Twenty-three of 130 patients (18%) had potentially limited health literacy and 5 had a high likelihood of limited health literacy.
Measures
After their visit, patients completed the 21-item Medical Interview Satisfaction Scale (MISS-21), the 9-item Shared Decision-Making Questionnaire (SDM-Q-9), the Patient-Reported Outcomes Measurement Information Scale (PROMIS) Depression Computerized Adaptive Test (CAT), the PROMIS Informational Support, the Newest Vital Sign (NVS), and a survey of demographic information (eg, age, sex, race, and insurance type). The MISS-21 is a 21-item measure of satisfaction with an office visit and treatment plan.19,20 The questionnaire includes both positively and negatively worded statements, such as “The doctor seemed warm and friendly to me” and “The doctor did not really understand my main reason for coming.” The 21 items are scored on a 7-point Likert scale ranging from “Very strongly disagree” to “Very strongly agree” resulting in scores ranging from 21 to 147, with higher scores indicating greater satisfaction. The raw scores were converted to a percentage.
The SDM-Q-9 is a psychometrically valid measure of perceived patient involvement in decisions. It consists of 9 statements which can be rated on a 6-point scale from “Completely disagree” to “Completely agree”. 21 It contains statements such as “My doctor and I thoroughly weighed the different treatment options” and “My doctor and I selected a treatment option together.” Adding the 9 items results in a raw score ranging from 0 and 45, which were converted to a percentage. Higher scores indicate greater perceived involvement in decisions. It is important to note that no items overlapped between the satisfaction (MISS-21) and the decision measures (SDM-Q-9).
The PROMIS Depression and Informational Support use item response theory as part of a CAT. 22 PROMIS Depression measures symptoms of depression with higher scores indicating greater symptom intensity. PROMIS Informational Support measures the perceived availability of helpful information or advice, asking patients to rate agreement with statements (eg, “I have someone to give me information if I need it”). Both PROMIS questionnaires are scaled to the general US population with a T-score of 50 representing the population mean, and each 10 points away from the mean representing one standard deviation.
The NVS is a reliable, interviewer-administered screening tool for measuring health literacy.23,24 Health literacy is defined as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions. 25 ” The NVS is based on the nutrition label of an ice cream container and consists of 6 questions that test the subject's understanding of health-related information and assesses both literacy and numeracy. The score ranges from 0 to 6, with a score from 4 to 6 indicating adequate health literacy, a score between 2 and 3 indicating the possibility of limited health literacy, and a score below 2 indicating a high likelihood of limited health literacy. 26
Statistical Analysis
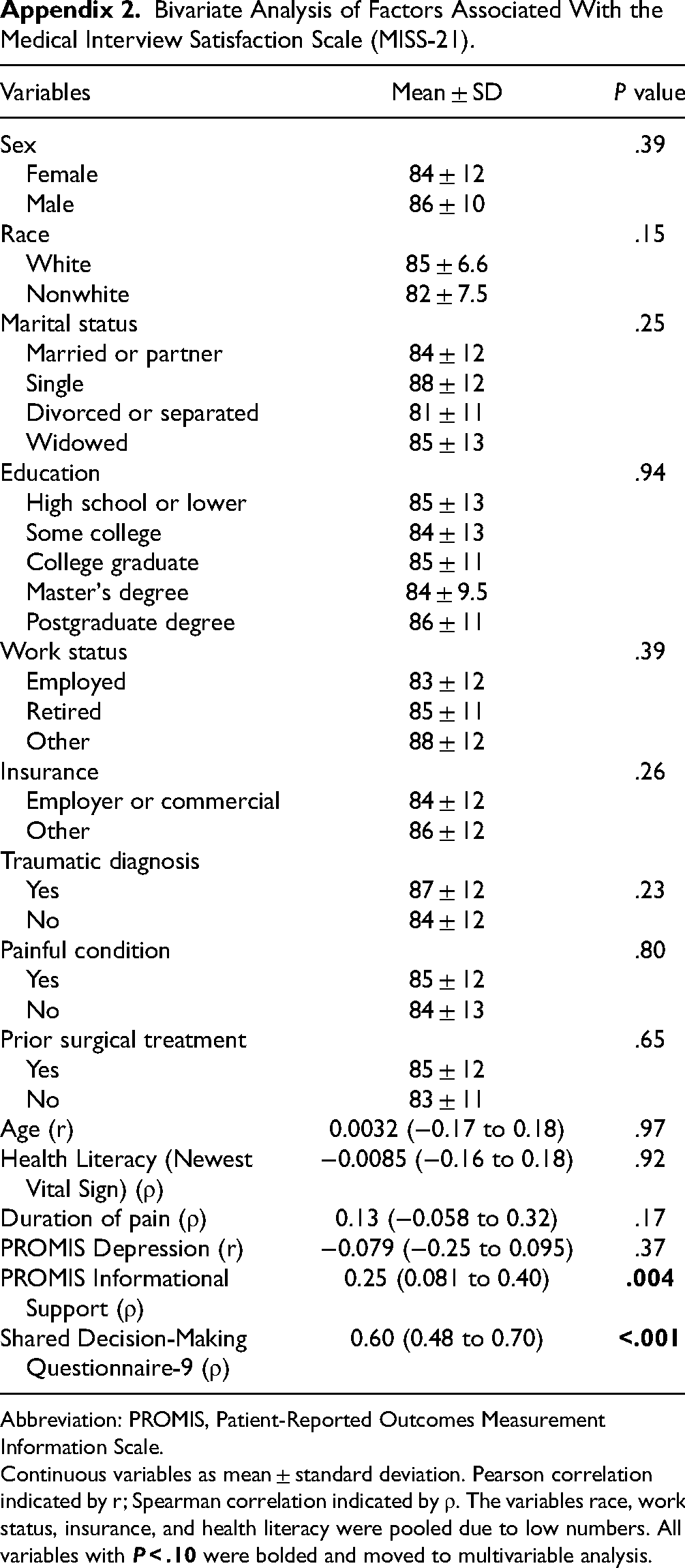
We tested whether or not the following factors were associated with satisfaction with the visit in bivariate analyses: age, gender, race, marital status, education level, work status, insurance type, and presence of a traumatic diagnosis, painful condition (yes or no), duration of pain (if painful), and prior surgical treatment (Appendix 2). We used unpaired t tests and 1-way analysis of variance for categorical variables, Pearson correlation, and Spearman rank correlation continuous variables. All variables with P < .10 in bivariate analysis were included in a multivariable linear regression analysis. We created 3 multivariable linear regression models, testing for moderating effects of (1) health literacy, (2) informational support, and (3) depression on the relationship between patient perception of involvement in decisions and satisfaction by including interaction terms (Appendices). In addition, we used Structural Equation Modeling to assess for potential mediation effects of health literacy, informational support, and depression (Figure 1A). P values below .05 were considered statistically significant. 27

Diagram of a mediation analysis: both direct and indirect effects of relationships between variables are measured.
An a priori sample size calculation demonstrated that 119 patients would provide 95% statistical power to detect a difference of 1.8% in satisfaction based on a multivariable linear regression model with α set at .05 and 3 independent variables (SDM-Q-9, the candidate mediator, and the interaction term). Accounting for 10% incomplete responses, we aimed to enroll 130 patients.
Results
Accounting for potential confounding in multivariable linear regression analysis, there was a notable association between greater patient perception of involvement in decisions and greater satisfaction with care, but there was no moderating effect of health literacy (Table 1; Appendix 3). In the structural equation model, health literacy did not mediate the relationship between patient-rated shared decision-making and satisfaction (Figures 2 and 3A).
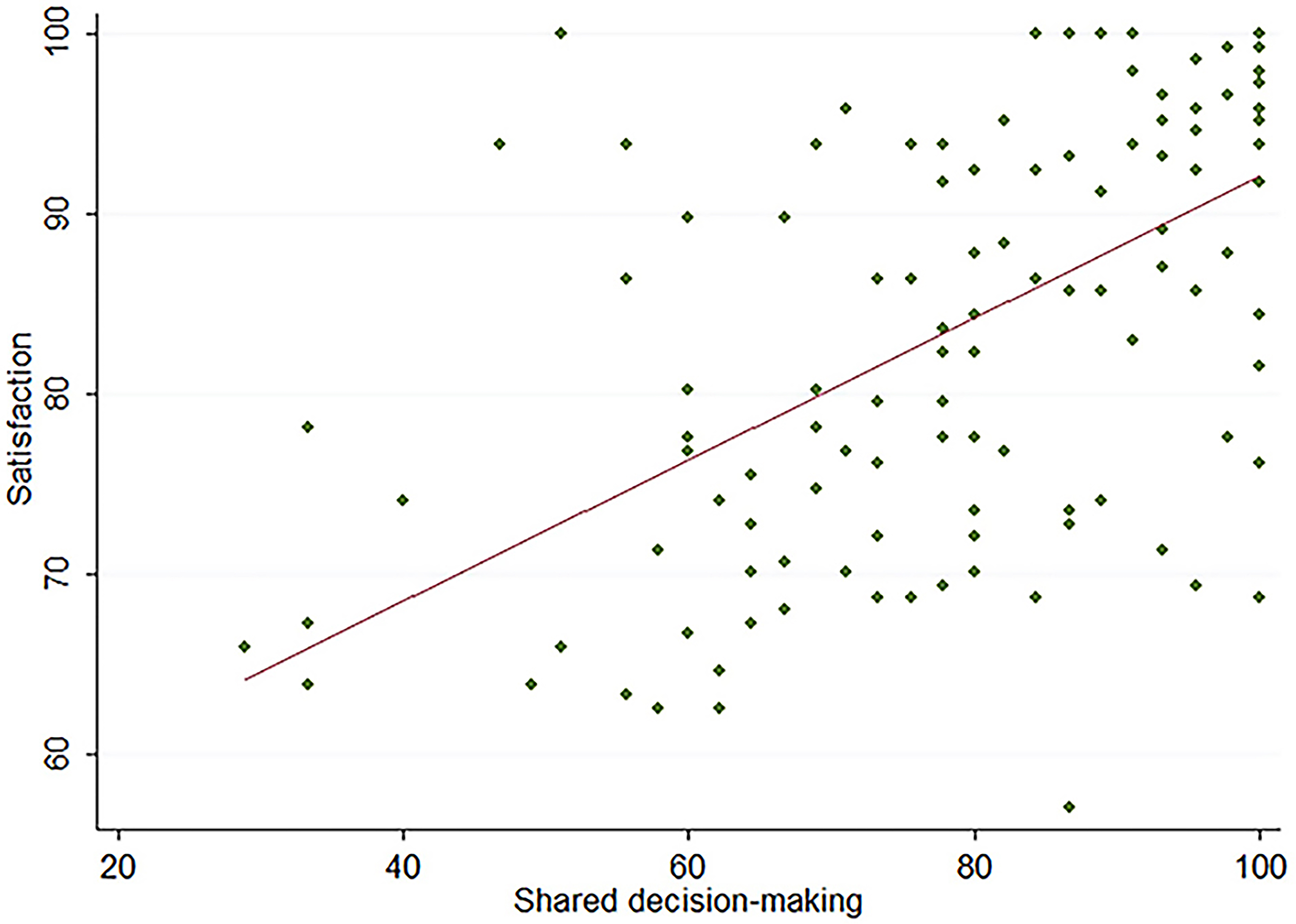
Diagram of a moderation analysis: the effect a third variable (moderator) on the relationship between variables is measured.

Scatter plot of the bivariate association between shared decision-making and satisfaction. Substantial ceiling effects were noted.
Multivariable Linear Regression Analysis, Testing for a Moderating Effect of Health Literacy, Informational Support, and Depression in the Relationship Between Shared Decision-Making and the Medical Interview Satisfaction Scale (MISS-21).a

Abbreviations: SDM-Q-9, Shared Decision-Making Questionnaire-9; NVS, Newest Vital Sign (health literacy); PROMIS, Patient-Reported Outcomes Measurement Information Scale.
Bold indicates statistical significance, P < .05.
Using similar analyses, there was no moderating effect on perceived availability of information and guidance (Table 1, Figure 3C). And there was no mediating effect of either variable (Appendices 4 and 5; Figure 3B). Higher PROMIS Informational Support was associated with greater satisfaction in multivariable linear regression: for every 5-point increase in PROMIS Informational Support, satisfaction increased by 1%, irrespective of patient-rated shared decision-making (Appendix 4).
Discussion
There is evidence that health literacy, informational support, and symptoms of depression have relationships with patient experience and well-being. If these factors partially account for (mediate) or accentuate/attenuate (moderate), the relationship between perceived involvement in decisions and satisfaction with care, strategies to address them might have the potential to improve the patient experience. The finding of a strong correlation between patient-rated shared decision-making and greater satisfaction that was independent of health literacy, perceived social support, and symptoms of depression points us to investigate other modifiable factors in our efforts to improve the experience.
This study should be read with the following limitations in mind. First, there were relatively few patients who were racial or ethnic minorities, few patients who were not college educated, and few patients with limited or lower health literacy, which may reflect the relatively advantaged socioeconomic status of the patients enrolled. However, the correlation between health literacy and satisfaction was negligible, and it is deemed unlikely that large mediation or moderation effects would be identified in different populations. Second, due to low numbers in some of the explanatory variables such as race/ethnicity, work status, and insurance status, had to be pooled. Therefore, we could not detect minor differences between these subgroups, making our findings less specific. Third, the addition of interaction terms in the moderation models introduces some collinearity, pushing PROMIS Informational support out of statistical significance. Therefore, readers should consider the multivariable models without interaction term more applicable. Fourth, it is possible that our clinicians were particularly good at tailoring expertise transfer to account for a patient's health literacy, thereby neutralizing its mediation or moderation effects, but that seems unlikely. More likely satisfaction and patient-rated shared decision-making are relatively independent of health literacy. Moreover, a cross-sectional analysis establishes association, but not direction. Fifth, these data were collected from several private-practice offices in a wide range of orthopedic subspecialties, but the exact number of providers is unknown, and could not be accounted for in the analysis.
The observation that there was no moderation or mediation effect of health literacy on the relationship between patient perception of involvement indecisions and satisfaction suggests that involvement in one's health strategy is satisfying at all levels of health literacy. The fact that a prior study of patients with upper extremity illness found no relationship between observer-rated informed shared decision-making and satisfaction is in notable contrast with the strong correlation of self-rated involvement in decision-making and satisfaction in this study and suggests there may be important differences between patient-rated and observer-rated involvement in decision-making. 28 Although it is important to tailor expertise transfer to account for a patient's health-related knowledge level and confirm all information is understandable, people may perceive involvement in decision-making independent of the relative success of that process. Although it is tempting to think that our clinicians are all very good at expertise transfer with people of various levels of health literacy, the more likely scenario is that measures of patient-rated shared decision-making and satisfaction with care are both acting as PREMs and measuring the quality of the patient–clinician relationship rather than the degree to which clinicians actually involve their patients in developing the health strategy.
The observation of no moderation or mediation effect of informational support suggests that the influence of shared decision-making on satisfaction is not affected by the perceived availability of information. Given the direct association observed between informational support and satisfaction, it may have an association that is independent of perceived involvement in decisions. To our knowledge, there are no prior studies that tested the effects of informational support on satisfaction with an (orthopedic) office visit. Informational support is a subtype of social support, and lower social support correlated with lower satisfaction with an office visit in prior studies.16,29
The observation that symptoms of depression did not moderate or mediate the relationship between patient-rated shared decision-making and satisfaction might suggest that symptoms of depression affect both patient-rated shared decision-making and satisfaction equally, which neutralizes its influence as a mediator or moderator. This possibility is supported by prior studies that patient satisfaction has small correlations with symptoms of depression,13,30,31 although depression was not associated with satisfaction in our current study. Given the evidence that lower mood is associated with less patient activation,11,12 attention to healthy mood might help motivate patients to participate in care.32–34 Patient-rated shared decision-making was a statistically significant predictor of satisfaction in the models accounting for health literacy and informational support, the addition of symptoms of depression pushes shared decision-making out of significance. This finding is likely caused by collinearity due to the interaction term; a linear regression model without an interaction term confirmed that depression was not associated with satisfaction.
Conclusion
We found that patient perception of involvement in decisions is strongly related to satisfaction independent of health literacy, perceived social support, and symptoms of depression. This directs us to consider other potentially modifiable factors associated with patient experience. 35 The quality of the patient–clinician relationship is not limited by understanding or mood and must be determined by other factors.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231171563 - Supplemental material for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction
Supplemental material, sj-docx-1-jpx-10.1177_23743735231171563 for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction by Tom J Crijns, Paxton Segina, Joost T P Kortlever, Jacob E Thomas, David Ring, Lee Reichel, Gregg Vagner and Sina Ramtin in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735231171563 - Supplemental material for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction
Supplemental material, sj-docx-2-jpx-10.1177_23743735231171563 for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction by Tom J Crijns, Paxton Segina, Joost T P Kortlever, Jacob E Thomas, David Ring, Lee Reichel, Gregg Vagner and Sina Ramtin in Journal of Patient Experience
Supplemental Material
sj-docx-3-jpx-10.1177_23743735231171563 - Supplemental material for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction
Supplemental material, sj-docx-3-jpx-10.1177_23743735231171563 for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction by Tom J Crijns, Paxton Segina, Joost T P Kortlever, Jacob E Thomas, David Ring, Lee Reichel, Gregg Vagner and Sina Ramtin in Journal of Patient Experience
Supplemental Material
sj-docx-4-jpx-10.1177_23743735231171563 - Supplemental material for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction
Supplemental material, sj-docx-4-jpx-10.1177_23743735231171563 for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction by Tom J Crijns, Paxton Segina, Joost T P Kortlever, Jacob E Thomas, David Ring, Lee Reichel, Gregg Vagner and Sina Ramtin in Journal of Patient Experience
Supplemental Material
sj-docx-5-jpx-10.1177_23743735231171563 - Supplemental material for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction
Supplemental material, sj-docx-5-jpx-10.1177_23743735231171563 for Moderators and Mediators of the Relationship of Shared Decision-Making and Satisfaction by Tom J Crijns, Paxton Segina, Joost T P Kortlever, Jacob E Thomas, David Ring, Lee Reichel, Gregg Vagner and Sina Ramtin in Journal of Patient Experience
Footnotes
Patient Demographics. Abbreviation: PROMIS, Patient-Reported Outcomes Measurement Information Scale. Continuous variables as mean ± standard deviation or median (interquartile range [IQR]); Discrete variables as percentage (number). Bivariate Analysis of Factors Associated With the Medical Interview Satisfaction Scale (MISS-21). Abbreviation: PROMIS, Patient-Reported Outcomes Measurement Information Scale. Continuous variables as mean ± standard deviation. Pearson correlation indicated by r; Spearman correlation indicated by ρ. The variables race, work status, insurance, and health literacy were pooled due to low numbers. All variables with Multivariable Linear Regression Analysis of Factors Associated With the Medical Interview Satisfaction Scale (MISS-21), Accounting for Health Literacy.a Abbreviations: SDM-Q-9, Shared Decision-Making Questionnaire-9; NVS, Newest Vital Sign (health literacy). Bold indicates statistical significance, P < .05. Multivariable Linear Regression Analysis of Factors Associated With the Medical Interview Satisfaction Scale (MISS-21), Accounting for Informational Support.a Abbreviation: SDM-Q-9, Shared Decision-Making Questionnaire-9; PROMIS, Patient-Reported Outcomes Measurement Information Scale. Bold indicates statistical significance, P < .05. Multivariable Linear Regression Analysis of Factors Associated With the Medical Interview Satisfaction Scale (MISS-21), Accounting for Symptoms of Depression.a Abbreviation: SDM-Q-9, Shared Decision-Making Questionnaire-9; PROMIS, Patient-Reported Outcomes Measurement Information Scale. Bold indicates statistical significance, P < .05.
Variables
Value
N
130
Age
56 ± 17
Sex
Female
81 (62%)
Male
49 (38%)
Race
White
104 (80%)
Hispanic or Latino
15 (12%)
Black or African American
9 (6.9%)
Other
2 (1.5%)
Marital status
Married or partner
73 (56%)
Single
26 (20%)
Divorced or separated
18 (14%)
Widowed
13 (10%)
Education
High school or lower
19 (15%)
Some college
36 (28%)
College graduate
44 (34%)
Master's degree
17 (13%)
Postgraduate degree
14 (11%)
Work status
Employed
64 (49%)
Retired
46 (35%)
Unemployed
8 (6.2%)
Disabled
6 (4.6%)
Student
6 (4.6%)
Insurance
Employer or commercial
77 (59%)
Medicare
41 (32%)
Medicaid
6 (4.6%)
No insurance
6 (4.6%)
Newest Vital Sign (health literacy)
4-6
107 (82%)
2-3
18 (14%)
0-1
5 (3.9%)
Traumatic diagnosis
33 (25%)
Painful condition
106 (82%)
Duration of pain (median, IQR)
83 (14-180)
Prior surgical treatment
110 (85%)
PROMIS Depression (t-score)
48 ± 9.1
PROMIS Informational Support (median, IQR)
60 (52-65)
Shared Decision-Making Questionnaire-9 (percentage, median, IQR)
82 (69-96)
Medical Interview Satisfaction Scale (percentage)
85 ± 12
Variables
Mean ± SD
P value
Sex
.39
Female
84 ± 12
Male
86 ± 10
Race
.15
White
85 ± 6.6
Nonwhite
82 ± 7.5
Marital status
.25
Married or partner
84 ± 12
Single
88 ± 12
Divorced or separated
81 ± 11
Widowed
85 ± 13
Education
.94
High school or lower
85 ± 13
Some college
84 ± 13
College graduate
85 ± 11
Master's degree
84 ± 9.5
Postgraduate degree
86 ± 11
Work status
.39
Employed
83 ± 12
Retired
85 ± 11
Other
88 ± 12
Insurance
.26
Employer or commercial
84 ± 12
Other
86 ± 12
Traumatic diagnosis
Yes
87 ± 12
.23
No
84 ± 12
Painful condition
.80
Yes
85 ± 12
No
84 ± 13
Prior surgical treatment
.65
Yes
85 ± 12
No
83 ± 11
Age (r)
0.0032 (−0.17 to 0.18)
.97
Health Literacy (Newest Vital Sign) (ρ)
−0.0085 (−0.16 to 0.18)
.92
Duration of pain (ρ)
0.13 (−0.058 to 0.32)
.17
PROMIS Depression (r)
−0.079 (−0.25 to 0.095)
.37
PROMIS Informational Support (ρ)
0.25 (0.081 to 0.40)
Shared Decision-Making Questionnaire-9 (ρ)
0.60 (0.48 to 0.70)

Variables
Regression coefficient
Standard error
P value
Adjusted R2
(95% confidence interval)
0.34
SDMQ-9
0.40 (0.31 to 0.50)
0.049
NVS
2.5 (−0.87 to 5.9)
1.7
.14

Variables
Regression coefficient
Standard error
P value
Adjusted R2
(95% confidence interval)
0.35
SDM-Q-9
0.38 (0.28-0.47)
0.048
PROMIS Informational Support
0.21 (0.022-0.39)
.093

Variables
Regression coefficient
Standard error
P value
Adjusted R2
(95% confidence interval)
0.33
SDM-Q-9
0.39 (0.30 to 0.49)
0.049
PROMIS Depression
0.0036 (−0.18 to 0.19)
0.095
.97
Acknowledgments
The authors would like to acknowledge Casey O’Connor, Yvonne Versluijs, and Mojtaba Talaei-Khoei for their contributions to the study protocol.
Authors’ Note
This work was performed at the Dell Medical School, The University of Texas at Austin.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TC, PS, JK, JT, LR, GV, and SR certify that they have no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article. One of the authors (DR) certifies that he, or a member of his immediate family, has or may receive payment or benefits from Skeletal Dynamics (USD less than 100,000, Wright Medical for elbow implants (USD less than 10,000), Deputy Editor for Clinical Orthopaedics and Related Research, Universities, and Hospitals, and Lawyers outside of the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.