
Abstract
Understanding factors that improve patients’ healthcare experiences are essential for healthcare providers (HCPs) caring for older adults (OAs). Previous data supports that effective patient-centered care leads to a better understanding of patients’ experiences, values, and preferences. The aim of this study was to evaluate OAs views of HCPs attributes and communication skills to better understand patient's views about their HCP interactions. Qualitative analysis of the data revealed five key themes that emerged: professionalism, patient rapport, patient-centered care, empathy, and communication. Addressing and optimizing performance in these areas could improve patient experiences and support enhanced training for healthcare students.
Keywords
Introduction
Older adults (OAs) have increased healthcare needs that require healthcare providers (HCPs) to focus on skills needed to improve patient-centered care. Patient-centered care has been recognized by The Institute of Medicine as one of six components of high-quality healthcare.(1) Effective patient-centered care and communication assist providers in better understanding patients’ experiences, values, and preferences.(2) Furthermore, empathetic communication has been shown to enhance patient experiences, improve health outcomes, and enhance trust.(3) The importance of patient-centered care and communication in healthcare is well studied,(4,5) Hannawa et al. discusses factors that patients’ value and utilized the Sufficient, Accurate, Clear, Contextualized, and Interpersonally Adaptive communication (SACCIA) evidence-based framework to explore the perspectives of physicians, nurses, and patients’ “good” and “poor” care encounters.(6) While the communication factors that impact effective experiences have been studied, a better understanding of the interplay between providers’ attributes and their communication skills could lead to improved patient-centered care. Thus, the objective of this study was to evaluate OA's views of HCPs’ attributes and communication skills to better understand those interactions and experiences.
Methods
This qualitative study was conducted between January and October 2019 at a large, urban state university and approved by the Institutional Review Board. An integral component of the interprofessional education (IPE) curriculum is the interprofessional team visit (IPTV). This experience involves healthcare students from eight programs: pharmacy, medicine, physician assistant, nursing, occupational therapy, physical therapy, social work, and dental. Interprofessional teams consisting of three to four healthcare students were randomly assigned to an OA 65 years or older. OAs were recruited from the community and provided written informed consent to participate in a home healthcare visit with the student team. Each student chose one of the following three questions to ask the OA: (1a) In your opinion, what qualities does a good provider possess? (1b) What qualities does a bad provider possess? (2) Have you ever had an issue communicating with a HCP? If yes, explain (3) Have you ever observed miscommunication/lack of communication among providers? (3a) How did this impact your health/healthcare? (3b) What recommendations do you have to improve communication? The questions were developed in 2015 by the IPTV program faculty members and have been used for 4 years prior to our study. Students collected OA responses and entered them into an online secure database developed at the university. Two study investigators conducted an inductive thematic analysis to evaluate OA responses utilizing six phases of thematic analysis: (1) familiarize yourself with the data; (2) generate initial codes; (3) search for themes; (4) review themes; ( 5) define and name themes; and (6) produce the report.(7) Investigators completed initial coding and theme searching individually; then met several times and reviewed and discussed themes to generate a clear definition and resolve conflicting opinions.
Results
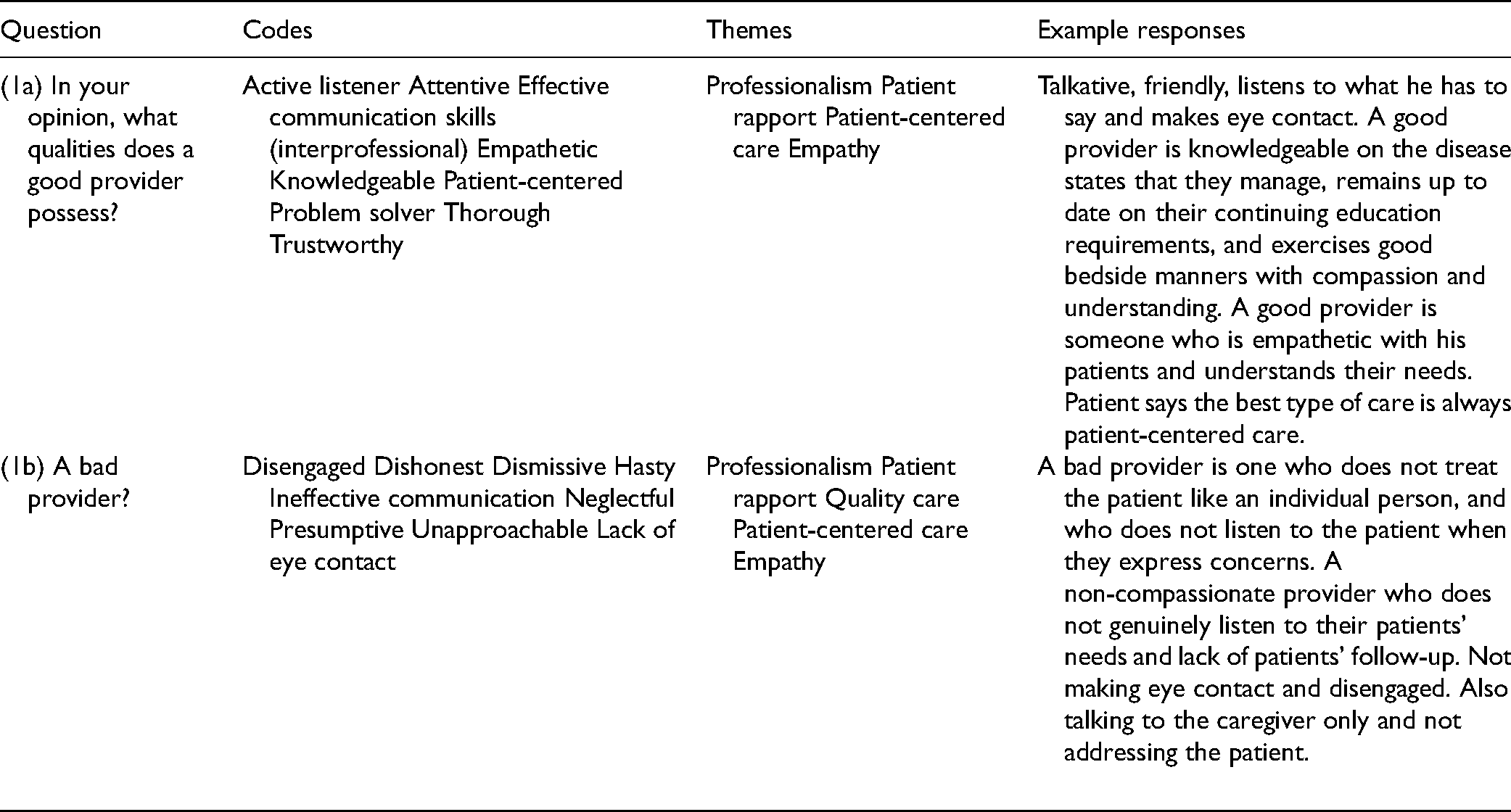
Ninety-five participant responses were collected between January and October 2019. Participant ethnicity included African American (37%) and Caucasian (61%). Data were coded and five themes emerged from questions one to three relating to HCP attributes and communication skills: professionalism, patient rapport, patient-centered care, empathy, and communication (Tables 1 and 2). Data pertaining to question (3b) (recommendations to improve provider communication) were coded into the following themes: professionalism, communication, and patient-centered care and example OA responses include:
“Having good intercommunication between providers is important,”
Provider Qualities.
Provider Communication Skills.

“Understand the patient is the center of care and including them in all decision making,” “…keep good notes of all the conditions as well as what patient says during their doctor visit,”
“Health care professionals should encourage patients to advocate for themselves…and take responsibility for their health.”
Based on OA responses, study investigators derived recommendations aimed to improve patient-centered care, medical documentation, face-to-face and interprofessional communication, patient education, patient empowerment, and electronic communication. Study investigators quantified the frequency of responses yet did not observe any significant difference.
Discussion
This study provides insights related to patient experiences and to our knowledge this is the only qualitative study to report OA views of HCP attributes and communication skills derived from an interprofessional healthcare student activity. The themes in our study are all salient to improving patient-centered care and HCP communication skills. Furthermore, our study suggests that ineffective provider communication skills, poor patient-centered care, and lack of professionalism can lead to OAs reporting delays in care, confusion, and negative health outcomes.
Like other studies, the themes from our study support improving patient-centered care and communication.(8,9) Huang and colleagues study evaluated how geriatric patients and their caregivers perceive HCP’s communication skills in an inpatient setting. This study illustrates a framework of “How” the healthcare team communicated, “When” they communicated, and “What” they communicated.(8) Our study demonstrates “How” HCPs communicated was important for OAs with responses that included terms such as active listener, attentive, thorough, and empathetic” descriptive of a “good provider”. They provided responses such as disengaged, hasty, neglectful, and lack of eye contact for “bad providers.”
OAs reported that empathy is an important HCP attribute. Empathy and emotional support are critical to satisfying patients’ emotional needs.(5) Increased provider empathy has been associated with improved patient satisfaction with care, better adherence to treatment, and improved health outcomes.(3) Ideally, the optimal provider–patient relationship should meet both informational and emotional needs of the patient. In “Patient-Centered Communication: Basic Skills”, the author provided guidance to HCPs related to the expression of empathy by naming the feeling; communicating understanding, respect, and support; and engaging the patient in their care.(4)
One of the themes highlighted in this study centers around the need to establish patient rapport and trust. An OA reported that “he felt as if the physicians neither valued his opinions nor trusted him regarding his conditions”. Such feelings prohibit active participation in their own care and increase their uncertainty of the care plan. However, providing a space for OAs to communicate their perspectives could empower them and attenuate negative outcomes.(9) Engaging patients in the care plan entails an understanding of the patient's perspective by exploring their feelings, ideas, concerns, and experience regarding the impact of the illness, as well as setting clear expectations with HCPs.(4) Haverfield and colleagues demonstrate that failure to allow the patient the space for self-disclosure and openness makes it difficult for providers to gather information about the patient and fully understand their experience and needs. The authors suggest asking follow-up questions, taking time to confirm a correct understanding of the patient's experience, sharing supplementary information, and acting on provided information as tips for active listening.(10) Similarly, “I Always Feel Like I’m Getting Skipped Over” emphasizes the consequences of HCPs not acknowledging patients’ perspectives leading to medical mistrust and perceived discrimination. These engendered patient dissatisfaction, nonadherence, and underuse of healthcare service.(11)
A noteworthy finding in our study was the impact of interpersonal communication among HCPs. OAs reported witnessing HCPs dismiss each other's contribution to the care plan which left the patient confused, delayed decision-making, and increased their mistrust in the care: “healthcare providers argued about whether my husband should come off dialysis or not. Neither one of them wanted to listen to the recommendations of the other”. “Communications in Health Care Teams” addressed the role of communication as one of the core factors for sustaining safety and quality, especially among health care teams.(12) In fact, communication failures among HCPs are among the leading causes of medical errors and patient harm which resulted in a joint commission patient safety goal committed to improving communication.(13)
Previous studies have shown that IPE develops HCPs skills that can improve patient outcomes through effective communication and teamwork.(14) Effective communication skills training for HCPs has resulted in a more patient-centered care approach.(2) The Interprofessional Education Collaborative made effective communication their third core competency focusing on the need to train HCPs to “communicate with patients, families, communities, and professionals in health and other fields in a responsive and responsible manner that supports a team approach to the promotion and maintenance of health and the prevention and treatment of disease”.(15)
Limitations
Our study involved a convenience sample of African-American and Caucasian participants recruited from Southeast Michigan and may not be generalizable to OAs from other ethnicities and geographic locations. Additionally, we did not collect data on social determinants of health which may impact OA perceptions of HCP attributes. Study questions were not formally validated, and the questions may have created response bias. The study does not directly evaluate the actual interaction between HCPs and OA as it only showed how OA's recall their interactions with HCPs. The healthcare students who asked the OAs questions transcribed their responses into the study database which may have led to response bias. The impact of this study on the students and their education was not reported. Despite these limitations, our study provides insights that may inform health professional students’ education.
In conclusion, understanding patients’ views of HCPs’ attributes such as rapport, patient centeredness, empathy, professionalism, and communication skills could lead to improved patient experiences, patient care, and support enhanced communication skills training for health profession students.
Footnotes
Acknowledgments
The authors would like to thank Wayne State University Research Design and Analysis Unit.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Wayne State University Institutional Review Board.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Wayne State University Institutional Review Board's (IRB# 099410B3X) approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Availability of Data and Materials
The data from this study are available upon request from the corresponding author.