
Abstract
KUDOS Statement
During the COVID-19 pandemic, both patients and clinicians experienced extreme challenges in providing and receiving sarcoidosis care. Further, patients with sarcoidosis had a unique experience of living in the COVID-19 pandemic as a vulnerable population.
In order to better understand and improve the quality of healthcare delivery and living, we convened a multi-national research team consisting of patient leaders, physicians, nurses, and therapists. We interviewed 28 patients recruited through sarcoidosis patient organizations in the 3 hardest impacted English-speaking cities during the early COVID-19 pandemic: London, New Orleans, and New York. The majority of participants had a multi-organ systems and severe sarcoidosis.
A great deal was learned to guide future healthcare delivery, disease management, and education. Among the many concepts expressed by the participants, there was great similarity across the 3 groups. The differences between the groups were in an expression of spirituality as well as in details of government and health systems.
Race, gender, and disability (including people with sarcoidosis) were voiced as inequities in healthcare access and intervention, societal respect, as well as disproportional COVID-19 exposure and contraction, with the expressed concern that these groups were at higher risk during the pandemic. There was clear agreement among all groups that there was an extreme disruption in care and communication and great concern that their diagnosis created survival disadvantage because of the disease biology and because they are less likely to receive life-saving treatment. These were thought to be true pre-COVID-19 but became overt during the pandemic.
The participants noted many crossover concepts between sarcoidosis and COVID-19. Some concepts related to whether COVID-19 infection could increase sarcoidosis disease activity or trigger new sarcoidosis cases, other concepts related to the biologic similarity of both being systemic multi-organ diseases mostly recognized for lung involvement. Many participants expressed struggles related to future health uncertainty, and lack of health professional knowledge.
Another similarity was that having sarcoidosis before the COVID-19 pandemic provided patients with experience to cope with the pandemic better than the general public. Many thought that the experience of people with sarcoidosis could help those living with multi-systemic effects of COVID-19.
Take-Home Message
People with sarcoidosis expressed infrastructural and scientific concepts that warrant close attention. There is perceived disparity in pre- and intra-pandemic of equity in healthcare access and in chance for survival. The pre- and intra-pandemic expressed needs of sarcoidosis patients may provide similar agency for other serious health conditions.
Introduction
Sarcoidosis is a systemic disease of granulomatous formation and aggregation in single or multiple organs, conferring a wide spectrum of multiple and diverse manifestations, symptoms, and severity. Disease burden is driven by inflammation which, if not self-limited or pharmacologically quelled, results in progressive, life-threatening damage, and fibrosis. The destructive capacity of sarcoidosis varies depending on the volume of granulomatous burden, organ/s involved, and location. For example, moderate granulomatous burden in cardiac muscle may be “clinically silent,” whereas miniscule aggregates crossing conduction pathways can cause fatal arrhythmias. Pulmonary, cutaneous, and ocular involvement are commonly recognized; while cardiac, neurological, gastrointestinal, and osseous manifestations are likely under-reported.
Several antigenic triggers are associated with sarcoidosis including mold, infectious and chemical exposures, with yet unknown influence on phenotype, genotypic interactions, or prognosis (1). The systemic inflammatory nature of active sarcoidosis can cause fever, fatigue/malaise, arthralgia/arthritis, atypical cutaneous, and other diffuse nonspecific manifestations challenging the ability to distinguish between active sarcoidosis and other concomitant diseases. Disease burden, immunosuppressive treatment, infection, and poor access to care worsen health outcomes.
COVID-19 is a mild to severe respiratory and multi-system illness transmitted chiefly by infectious respiratory droplets. COVID-19 is commonly characterized by fever, cough, and shortness of breath potentially progressing to respiratory failure. However, both in COVID-19's acute and chronic forms, multiple organ systems may be involved resulting in cutaneous, articular, neurological, cardiac, gastrointestinal, and hematological manifestations. The chronic form may be related to immune activation, long recovery, persistent residual damage to organ tissue as with sarcoidosis.
At the time of this publication, the literature lacks an investigation of sarcoidosis as experienced by patients in the COVID-19 pandemic. The stark initial challenges encountered by patients and clinicians in the early COVID-19 pandemic predominantly expressed through international, national, and local online support groups inspired this study. This study examines the experience of living with sarcoidosis in three of the hardest impacted regions during the early COVID-19 pandemic: London, New Orleans, and New York.
Methods
The impact of the COVID-19 pandemic on people living with sarcoidosis was examined in three global English-speaking areas with the highest COVID-19 incidence and death per capita during April 2020: London, UK; New Orleans, USA; New York City, USA (2,3). Three geographically distinct focus groups (FGs) with an a priori decision of 5 to 12 attendees per group based on the response, were conducted in April/May 2020 (Figures 1 and 2). The study protocol was approved, implemented, and with all participants consented according to Institutional Review Board #743566. Potential participants self-referred to the project after viewing sarcoidosis support group email or social media announcements, and were accepted on a first-come basis.
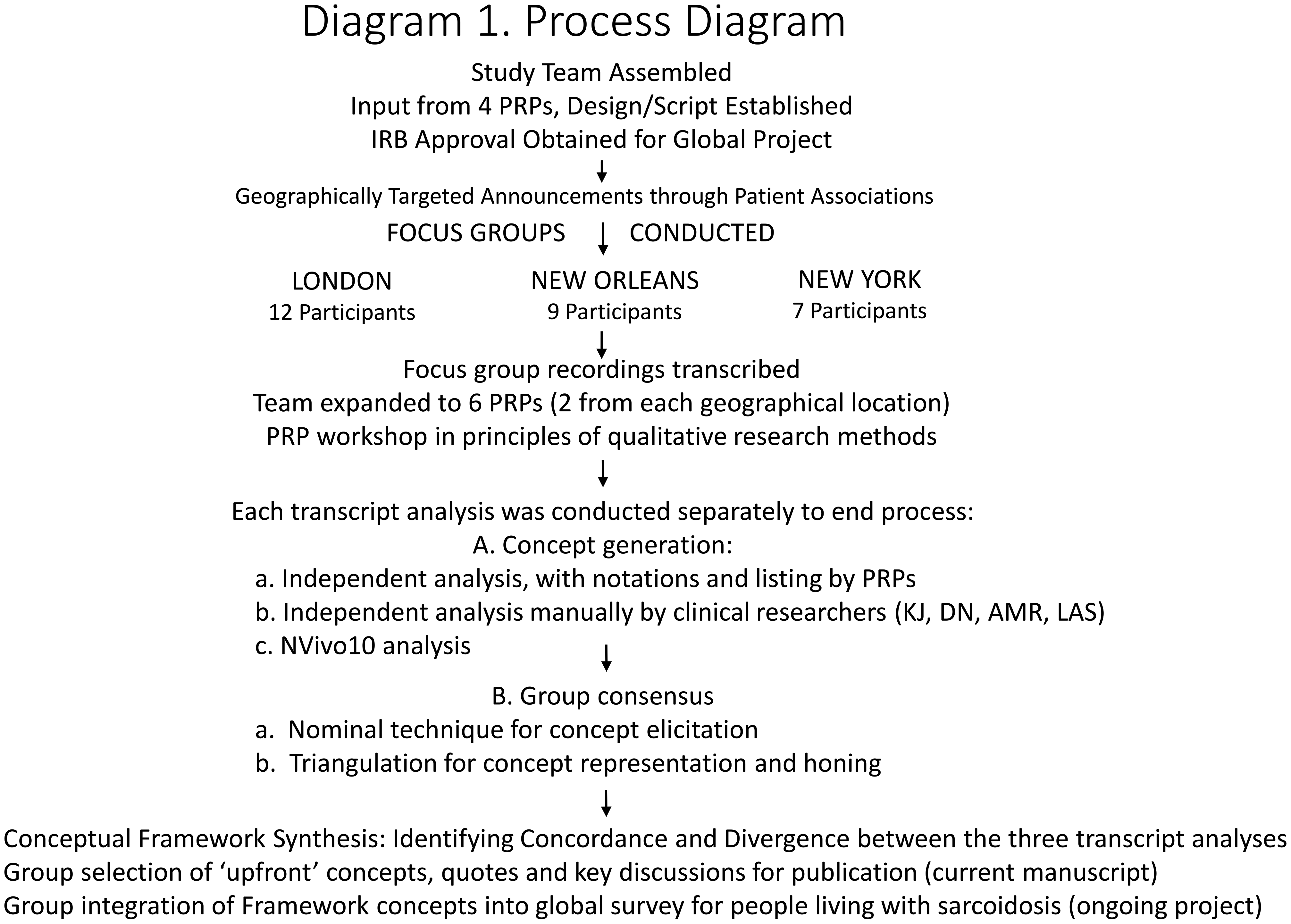
Process diagram.

CONSORT diagram of enrollment.
Face-to-face FG interviews via Zoom.us were closed to nonparticipants, planned for 90 to 120 min, led by AMR and LAS with an open interview framework relying upon patient-driven discussion for the content of COVID-19 related topics. FGs began with interviewer and participant introductions. Participants were invited to state their first name, the duration, degree of organ involvement, and treatment of sarcoidosis, along with a history of COVID-19 exposure or infection. Two questions drove the FG discussions: (1) “Thinking back to just before COVID-19 emerged, and then thinking about now, how has COVID-19 impacted your life as a person living with sarcoidosis?” (2) “Thinking back to prior to COVID-19 and then now, how has your health-related to sarcoidosis changed since COVID-19 emergence?.” During the discussion, intuitive interviewer probes delved for further detail or to check for a collective agreement. FGs were audio-recorded with concomitant field notes and transcribed verbatim. Participants were aware of the interviewers’ backgrounds and openly informed of the project's goals and motivations.
The study team consisted of 4 experienced qualitative researchers (AMR, DN, KJ, LAS) an RN/PhD and psychometrician, an MSc/PhD and 2 MD/MPHs, and 6 patient research partners (PRPs), a male and female from each geographic area, nationally recognized peer leaders with prior exposure to collaborative research (4). This resulted in 10 coders for each transcript. PRPs were trained on practical aspects of grounded theory (5,6) which guided transcript analyses, concept generation, triangulation, theme emergence, and framework production.
PRPs’ individual and group analyses provided the initial concept generation for each transcript, which was then merged with the iterative in-depth manual and Nvivo10 software-generated analyses by the professional researchers. A sequential nominal group approach facilitated all collective concept generation, agreement, and framework production (7,8). PRPs were restricted to observing the initial consensus exercises of their own FG's transcript but responsible for review and feedback on the team's analysis.
Results
A total of 28 interviewees (Table 1) participated without attrition. The median FG duration of 2.83 h and was driven by patient contributions and enthusiasm. Each FG member received their group's transcript for feedback, without further commentary.
Patients and Characteristics.
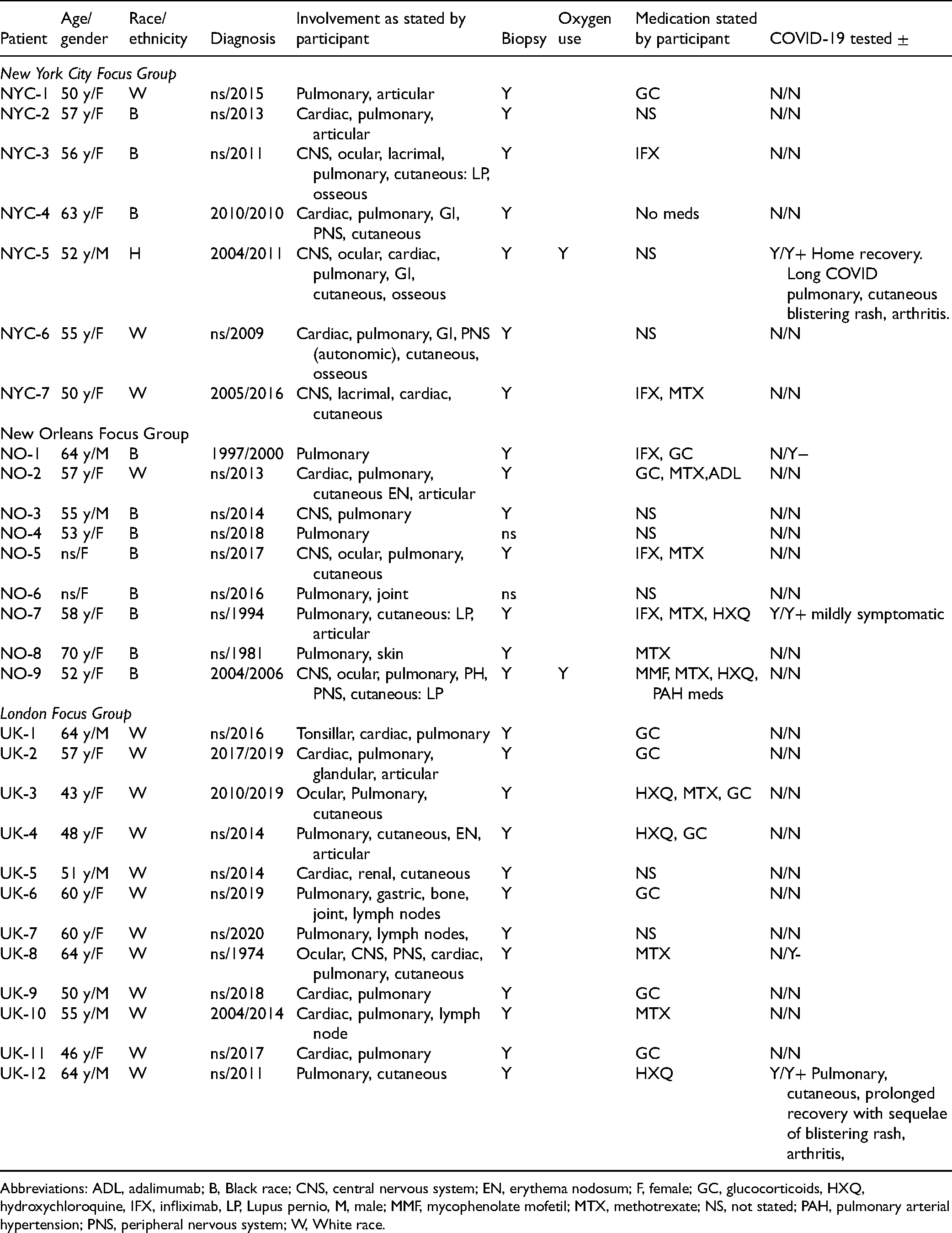
Abbreviations: ADL, adalimumab; B, Black race; CNS, central nervous system; EN, erythema nodosum; F, female; GC, glucocorticoids, HXQ, hydroxychloroquine, IFX, infliximab, LP, Lupus pernio, M, male; MMF, mycophenolate mofetil; MTX, methotrexate; NS, not stated; PAH, pulmonary arterial hypertension; PNS, peripheral nervous system; W, White race.
Data saturation for each focus group was cross-checked by concept occurrences in the other 2, concept consistency prevailed between groups except in areas of spirituality and regional particulars. No repeat interviews or follow-up questions occurred.
Overarching Themes (OTs)
Three overarching themes (
Overarching Themes.
“
“
“
Selected Quotes From Online Supplemental Material.

Sarcoidosis Survival Ecology (OT1)
“Sarcoidosis Survival Ecology” (OT1)
defined by its main themes, “Interconnections” and “Personal Evolution and Emergence,” reflect themes of multi-faceted, iterative, interdependent actions, and experiential personal growth while living with sarcoidosis describing identity, knowledge, and learned-COVID-19/crisis preparedness.
Networks, Activism, and Healing
A clear distinction was made between support groups and focus groups. Both created a sense of “belonging,” “support,” and “validation,” but support groups facilitated bi-directional knowledge sharing, peer mentorship in navigating healthcare, resources, and expectations. Focus groups stimulated pragmatism, relating to research, education, and health systems policy needs for standardized information.
Divergence
All participants of the New Orleans group were strongly and normatively declarative in spirituality and faith, which did not occur in other groups.
Self-Advocacy and Growth
Participants unanimously confirmed a trajectory of being initially devastated by a sarcoidosis diagnosis and the multi-relational experience of uncertainty and the subsequent gathering of motivation to become knowledgeable about the disease, health systems, and coping. Beyond the fear and dread of COVID-19, there was agreement that wisdom gained from living with sarcoidosis put them in a place of preparedness to protect against COVID-19, such as the early self-imposed implementation of family/self-isolation, and coping with the complex uncertainties associated with COVID-19.
Self-advocacy and self-protection were perceived as sometimes creating a hardship on personal and professional relationships during COVID-19. It placed additional work or restrictive burdens on others; including forcing patients to share the seriousness of their health status with others when they would have otherwise elected not to, e.g. employers, visitors, etc.
Credible Information
Participants initially were heavily involved with COVID-19-related news several hours daily, and subsequently restricted their exposure to less than an hour to protect psychological and emotional well-being, productivity, and engagement in more fulfilling life activities.
Discussions persisted around the credibility of COVID-19 information. Most participants distilled information from several sources; with reliance on scientists from governmental or international organizations such as Centers for Disease Control (CDC) or World Health Organization (WHO) or National Health Service (NHS). Widely expressed was that the presentation of information was misused and misrepresented for political, self-interested gain and by the media for “shock value.”
COVID-19—Sarcoidosis Interactions and Similarities (OT2)
“COVID-19—Sarcoidosis Interactions and Similarities” (OT2)
addresses the repeated voicings related to the myriad colliding facets between the respiratory and multi-organ system nature of sarcoidosis and of COVID-19; as well as questions regarding the viral triggering of inflammatory diseases.
Disease Behaviors
Clinical guidance was confused by similar symptomatology and manifestations between sarcoidosis flaring and COVID-19, i.e. sarcoidosis activity versus COVID-19 infection versus both occuring simultaneously; and made more complicated by COVID-19 testing/re-testing's questionable utility and reliability. Participants reported having to rely upon clinicians without experience in sarcoidosis to answer complex questions. This included addressing sarcoidosis flares, whether to continue sarcoidosis treatment and confusion over sarcoidosis versus COVID-19 symptoms. Further, in the United Kingdom, this became especially problematic when relying upon GP diagnosis for the attainment of COVID-19 protective status for vulnerable people (9,10).
These uncertainties led to a lack of confidence in COVID-19 screening, as well as diagnostic interpretations and treatment plans. Additionally confounding was the potential of immune-modulating sarcoidosis medications to increase vulnerability to infection, potentially conferr a protective effect or even be effectice in the treatment of COVID-19. Concern over the potential of potential pathogenic interactions between COVID-19 and sarcoidosis disease behavior, were diffuse in all groups, and notably in those with cardiac sarcoidosis. Despite, interest in sarcoidosis therapies potentially attenuating COVID-19 virility, participants’ fear of their immunosuppressed status drove compliance with the new/alternate sarcoidosis treatment strategies in response to the pandemic.
Shared and Intersecting Patterns
Evolving knowledge of research, diagnosis, natural history, and disease phenotypes, prognostic factors, and management as well as patient, general population, and clinician education were voiced as sharing similar trajectories in COVID-19 in the general population and the pre-COVID-19 sarcoidosis experience. The groups expressed that respiratory and multi-organ system conditions, like sarcoidosis, historically received limited public awareness, research attention, and funding; and that the COVID-19 pandemic may lead to a greater appreciation of and knowledge in respiratory and multi-organ system diseases. Further expressed was the hope that knowledge gained in sarcoidosis (1,11–16) might be useful in understanding the quality-of-life and therapeutic realms of COVID-19 treatment and recovery.
Participants had proactive self-determination strategies distilled to minimizing risk, vigilance in detection, paying attention to distinctive features of otherwise non-specific symptoms, for example, fever-type, and pattern, and self-reliance in deciding when and how to seek medical treatment. Though sarcoidosis was perceived as an experience which cultivated skills that facilitated greater ease in coping with and responding to the threat of exposure and to the uncertain medical knowledge during COVID-19; a sarcoidosis diagnosis was perceived as creating disparities when compared with the healthy population impacting “eligibility selection” for life-saving COVID-19 interventions such as mechanical ventilation and ICU admission. Many perceived COVID-19 infection as inexorably linked to death, in sarcoidosis; therefore each group's COVID-19 survivors were important catalysts for expressed new perspectives, relief yet sustained vigilance.
Healthcare Logistics
COVID-19-related disruption on all aspects of routine and emergent sarcoidosis-care was diffusely reported in relation to essential and critical diagnostics, infusions, medication assessment/tapering, attainment of refills and communication lines to specialists. Participants expressed a sense of health system abandonment during the pandemic, apprehension was particularly voiced regarding follow-up care by those with cardiac and ocular sarcoidosis and those midstream of a new sarcoidosis diagnositic work-up. These strains led to worry and greater uncertainty for sarcoidosis-related survival. Related to this, participants voiced a sense of guilt in having a health condition that required significant attention and resources, while in the midst of a pandemic.
The abrupt discontinuation or prolonged unchecked administration of glucocorticoids, were voiced experiences. Participants reported difficulties with hydroxychloroquine attainment as a result of depleted supplies as well as roadblocks by insurance in the United States.
Environmental/Societal External Needs and Influences (OT3)
“Environmental/Societal External Needs and Influences” (OT3)
captures predominantly fixed situational factors that patients perceive require patient effort to navigate and influences patient behavior and outcomes. It characterizes factors which are predominantly unidirectional pressures. This is different from the bi-directional inter-relational growth experiences of “
Race, Gender, Socio-Economic, and Disability Inequity
“Discrimination” and “Healthcare Disparities” were pervasive themes relational to recurrent sub-themes including a disproportion of essential workforce thus increasing COVID-19 exposure and contraction, financial hardship pressuring work and caring for vulnerable others. Also, many sub-themes of deficiency in access to education, computers, technology as well as being pre-disposed to disrespectful social interactions (18).
While racial, gender, and SES health disparities such as COVID-19 testing and insurance coverage were less prominently voiced in the UK group, health disparities related to geographic location and preferential medical resource allocation to the able-bodied without underlying health conditions, such as access to critical care beds or mechanical ventilation, was strongly voiced by all groups.
Managing Exposure
Having sarcoidosis, immunosuppression, and prior non-COVID-19 infection experiences drove sub-themes of early self-imposed isolation, moving from city dwellings, and combining or splitting households to reduce location-based risk. Household decision-making regarding decontamination rituals, obtaining and handling of essential supplies, and risk reduction strategies between household members were motivated by the immunosuppressed vulnerability.
Social Factors
Positive and negative social factors were voiced. Participants noted that local communities rallied to assist and protect those more vulnerable, but alternatively participants reported feeling increasingly vulnerable due to self-interested individualistic attitudes toward protecting others and because of “guidance” from unreliable sources. Participants also experienced negative attitudes in pre-COVID-19 times for sarcoidosis symptoms such as coughing in public—now markedly exacerbated.
In the UK, a “shielding letter” for high or moderate risk groups was necessary for priority food and pharmacy deliveries and to access special protected shopping hours (9,10). However, sarcoidosis was not specifically listed (10,19) with patients frustrated and reliant on the local physician/GP for issuance. The practical value of the letter was perceived to have both negative (potentially being denied ventilator support) and positive (priority access to medications and groceries) implications.
Work and Family
Patients reported myriad layers of complexity dictated by circumstance influencing work and home relations with resultant physical, financial, logistical, and psychological implications. A number of participants were primary caregivers which had further implications for self-exposure as well as protecting and providing for the vulnerable family member. Configuration of physical space impacted exposure risk, personal relationships, and well-being. The UK organized specialty provisions for childcare and eldercare for essential workers as well as work accommodations for vulnerable employees or employees with vulnerable family members at home.
Discussion
In the best of times, it is challenging for clinicians and patients to address healthcare needs related to complex multi-organ system diseases such as sarcoidosis. As researchers, investigating sarcoidosis experiences of the COVID-19 pandemic, the purview of the sarcoidosis experience before the COVID-19 pandemic provided an essential relational platform. The COVID-19 pandemic has amplified and disclosed underlying infrastructural vulnerabilities that had routinely impacted this population, but it also appears to have underscored strengths often cultivated by living with a serious health condition.
This research exemplifies the extent to which patient expertise has the potential to drive research and health system priorities. As a result of living through the COVID-19 pandemic, people with complex health conditions can provide guidance on both how navigate the extreme times precipitated by a pandemic as well as how this experience can influence routine healthcare delivery in the future. We anticipate these pre- and intra-pandemic findings are unlikely to be unique to sarcoidosis (19) and ardently hope that this dense, intense base of information will inform investigational off-shoots into psychological, systems management, and quality-of-life research in sarcoidosis and other multi-system diseases—including “post-COVID-19 syndrome.”
The framework is intricate and more extensive than could have been anticipated, but it captures the necessary detail reflective of a complicated multi-system disease (sarcoidosis) experienced with in the context of another biologically and socially complex disease (COVID-19). In this regard, the framework is an agent of sensitization and strategy that can be tested and applied beyond sarcoidosis. In regard to sarcoidosis, the framework discloses unstable underpinnings to healthcare system structure, education, communication, and service industries that required the push of a crisis for overt revelation. The crisis also illuminated pre-existing education and knowledge gaps, and the need to be better equipped to support those living with precarious multi-system diseases in a crisis. Importantly, the pandemic heightened participants’ pre-existing sensibilities and frustrations regarding inequities of disability and race, and healthcare structure and society interactions as a subclass, particularly in relation to research funding, allocation of healthcare resources, knowledge, and clear communication.
The strengths of the design harnessed the perspectives, priorities, and concerns of participants residing in global English-speaking areas with the highest incidence and mortality during the time of data collection. Thus, we anticipate that the broadest and most intense experiences of the COVID-19 outbreak as experienced by people living with sarcoidosis are captured here. The collection time-period occurred after the initial few weeks of isolation measures, therefore, allowing for valuable assimilation perspectives and experiences to augment relevant concept collection.
In this study, patient participants, PRPs, and researchers developed an authentic collaboration at the onset, in question framing, research design and conduct, and subsequent dissemination strategies. Power-sharing served to reduce inequalities and enabled honest and transparent discussions.
Pervasive in all groups was the need for improved access to specialist physicians and nurses for a deeper lever of individualized support and care. The authors draw attention to the lack of any patient and caregiver inclusion on COVID-19 related research published to date. These frustrations were recently expressed by the physician–patients with COVID-19 (20) and echo throughout our findings with relevance to the COVID-19 or sarcoidosis disease experience or both combined. These physician–patients urge the formation of “one-stop” clinics as hubs of care, pattern-recognition and sentinel expertise to identify and manage COVID-19 sequelae in order to expeditiously augment and propel the acquisition and dissemination of medical knowledge. Sarcoidosis centers of excellence still appear to have a sequestered recognition and treatment knowledge not yet deployed in general pulmonary, rheumatology, or other sub-specialty clinics, as reflected in the framework. However, the framework also states that the global experience of COVID-19 may yet influence the frontiers of knowledge dissemination in these rarer complex multi-system diseases.
Whether underlying inflammatory diseases are pathogenically triggered or worsened by the contraction of COVID-19 was presented in this data months before such suppositions were published in the literature (21,22). This speaks to seasoned patients’ instinctual inclination related to sarcoidosis natural history, susceptibility according to the degree of immunosuppression, and conceivable synergistic and potentiating pathogenicity. Similarly, astute speculations regarding vaccine availability, effect, and management—as well as discriminatory implications of COVID-19—again, seemed driven by patients’ expertise acquired by experiential sensitization to pathogenicity and medical knowledge exposure.
Regarding study limitations, the hope for survival appears to drive content, however, defeat, a fairly common concept expressed on patient social media, is absent in our study. Selection bias with participant self-referral via patient associations may have attracted participants: (a) with higher levels of self-efficacy skills, (b) “seasoned” with longer disease durations and possibly “upskilled” in coping, and (c) less likely hampered by psychological demotivation. Outreach strategies designed specifically to support those newly diagnosed and experiencing mental hardship could be warranted.
We regret that access to linguistic resources impeded the ability to investigate non-English speaking, high COVID-19 endemic areas. We also recognize that representation was heavily weighted by participants with more severe disease. However, a bias toward disease severity likely intensifies and broadens the conceptual spectrum that might be experienced across sarcoidosis severity and phenotypical differences. We will further examine these differences in the global open-query phase of this project.
The conclusions reached in this study promise helpful and generalizable insights; despite constantly evolving information and issues of the COVID-19 pandemic. Data collection was completed prior to the current global concerns of schooling during the pandemic, however the six PRP authors as international leaders advocate this to be a serious situation and best left to parental households to decide on an individual family basis.
Future directions are currently querying these results in the global sarcoidosis patient community to assess generalizability and deficits of these findings.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221075556 - Supplemental material for Sarcoidosis Illuminations on Living During COVID-19: Patient Experiences of Diagnosis, Management, and Survival Before and During the Pandemic*
Supplemental material, sj-docx-1-jpx-10.1177_23743735221075556 for Sarcoidosis Illuminations on Living During COVID-19: Patient Experiences of Diagnosis, Management, and Survival Before and During the Pandemic* by Lesley Ann Saketkoo LA, MD, MPH, Kelly Jensen, MD, MPH, Dimitra Nikoletou, PhD, MSc, Jacqui J. Newton, Frank J. Rivera, BA, Mike Howie, Rodney K. Reese, Melanie Goodman, BS, Patricia B. Hart, MBA, Whitney Bembry, MD, Adam Russell, BA, Isabelle Lian, MS, Matthew R. Lammi, MD, MSCR, Mary Beth Scholand MB, MD, and Anne-Marie Russell AM, PhD, APRN, ATSF in Journal of Patient Experience
Footnotes
Acknowledgments
Sarcoidosis UK, Sarcoidosis Awareness Foundation of Louisiana, National Sarcoidosis Support Network, New Orleans Sarcoidosis Support Group. AMR is a National Institute for Health Research (NIHR) Senior Nurse and Midwife Research Leader. The views expressed in this article are those of the author(s) and not necessarily those of the NIHR, or the Department of Health and Social Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sarcoidosis Awareness Foundation of Louisiana (grant number L30 HL129466, unknown). Charles and Elizabeth Wetmore Foundation (LAS), Sarcoidosis Awareness Foundation of Louisiana (LAS), National Institutes of Health (US) NIH/NHLBI L30 HL129466 (MRL). National Institute of Health Research UK (AMR).
Ethics Statement on Human and Animal Research
The study protocol was approved, implemented, and with all participants providing consent according to Institutional Review Board #743566 and the World Medical Association Declaration of Helsinki. This study did not involve animals.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.