
Abstract
Potentially preventable hospitalisations (PPHs) occur when patients receive hospital care for a condition that could have been more appropriately managed in the primary healthcare setting. It is anticipated that the causes of PPHs in rural populations may differ from those in urban populations; however, this is understudied. Semi-structured interviews with 10 rural Australian patients enabled them to describe their recent PPH experience. Reflexive thematic analysis was used to identify the common factors that may have led to their PPH. The analysis revealed that most participants had challenges associated with their health and its optimal self-management. Self-referral to hospital with the belief that this was the only treatment option available was also common. Most participants had limited social networks to call on in times of need or ill health. Finally, difficulty in accessing primary healthcare, especially urgently or after-hours, was described as a frequent cause of PPH. These qualitative accounts revealed that patients describe nonclinical risk factors as contributing to their recent PPH and reinforces that the views of patients should be included when designing interventions to reduce PPHs.
Keywords
Introduction
An admission to the hospital caused by the absence, underutilization, or inadequacy of primary care services is often classified as a potentially preventable hospitalisation (PPH) (1). By 2017–2018, almost 750,000 of all Australian hospital admissions (6.6% of total admissions) were thought to be PPHs, representing a steady annual rise of 3.5% per year since 2013-2014 (2). Rates of PPHs are often used as a proxy measure of primary care quality and equity (3). Hospitals and their emergency departments (EDs) are not appropriate places for primary healthcare as they do not allow for continuity of care, are relatively more expensive and there is a risk of exposure to unnecessary testing and hospital-acquired harms (4).
Australia's health system is funded publicly by state and federal governments. The universal health insurance scheme, Medicare, provides free hospital treatment at public hospitals throughout the country. Primary healthcare services may be provided with no out-of-pocket expenses (“bulk-billed”) through Medicare, or an additional payment may be charged (a “gap fee”). Costs associated with other health providers, such as ambulance services, vary between jurisdictions; for example, Tasmanians can use ambulance services without charge, while other states levy a charge with each use. The broader primary health system includes doctors (usually general practitioners [GPs]) nurses, dentists, pharmacists, and other allied health professions. In Australia, patients who are in a position to take out private health insurance can experience greater choice, shorter wait times, and receive a Medicare rebate.
The social determinants of health (SDoH) include education, economic and employment status, housing, access to transport, and access to health services (5). For relatively disadvantaged populations, which include rural communities in developed countries, the impact of the SDoH may be disproportionate (6). Frameworks have been developed to help highlight the significant social and structural factors that influence rural health services and outcomes (3,7–).
The rate of PPHs in remote Australian communities is almost double that in major cities, suggesting a geographical gradient in occurrence (2,8). The limited health workforce and service availability, less frequent GP visitations, an older population, and health literacy challenges in rural populations may all contribute to higher rates of PPH (10,11). Other known risk factors for PPH include low socioeconomic status (SES) (12–), limited social support (16–), and comorbidities (19–). For acute conditions, the presence of significant comorbidity increases the risk of PPH (22).
Previous qualitative studies with urban and rural Australian patients suggested the perceived urgency of their condition, an expected need for specialized services and the convenience of hospital treatment strongly influenced PPH events (23–). Social isolation, or the absence of social support, was strongly associated with adverse health outcomes, including increased mortality, mental health conditions, and poor self-rated health of older people (17,27). Risk factors for social isolation include lack of private transport, living alone, and reduced contact with family and friends (27). The contribution of social factors to hospitalization risk, specifically in the rural Australian setting, has been understudied (17) and is therefore poorly understood.
Overall, there have been few qualitative studies specifically examining Australian rural patients’ perspective of their PPH. Sociodemographic, health, and infrastructure differences in rural areas may render known predictors of PPHs suggested by urban-based studies insignificant. Therefore, the aim of this qualitative study was to identify common risk factors that rural Australian patients described as contributing factors associated with their recent PPH.
Methodology
Consistent with a pragmatist worldview (28), the authors employed the six-step reflexive thematic analysis (29,30), to inductively identify sub-codes, codes, and themes from the data. Given the small number of participants (n = 10), going beyond the surface meaning of the data (latent themes) would not have been appropriate (31,32). It was not assumed that the risk factors identified in different studies and locations, or indeed the same population (33), would be reinforced by this study; rather, this study was intended to provide evidence of PPH causes unlikely to be represented in quantitative data. The guiding research question was: “According to adult patients from rural Tasmania, Australia, who have a lived experienced of a PPH, what were the drivers of their PPH and could these admissions have been prevented (if so, how)?”
Reflexivity
One author (A.R.) was familiar with PPH literature and has previously led quantitative research in the same setting (33). The researcher (V.A.) employed to collect data had no prior connection to the study population; this was to avoid any potential for power imbalance or courtesy bias. Independent to the GP practice, researchers G.P. and R.N. were able to provide critical prompts to ask questions in their review of the codes, sub-themes, parent themes, and quotes.
Rigor
Qualitative research rigor was ensured by use of the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (34) (see Supplemental Material), and the framework for ensuring qualitative research integrity is described by Colorafi and Evans (35) (Table 1).
Rigor Measures for Qualitative Research and Application to This Study.
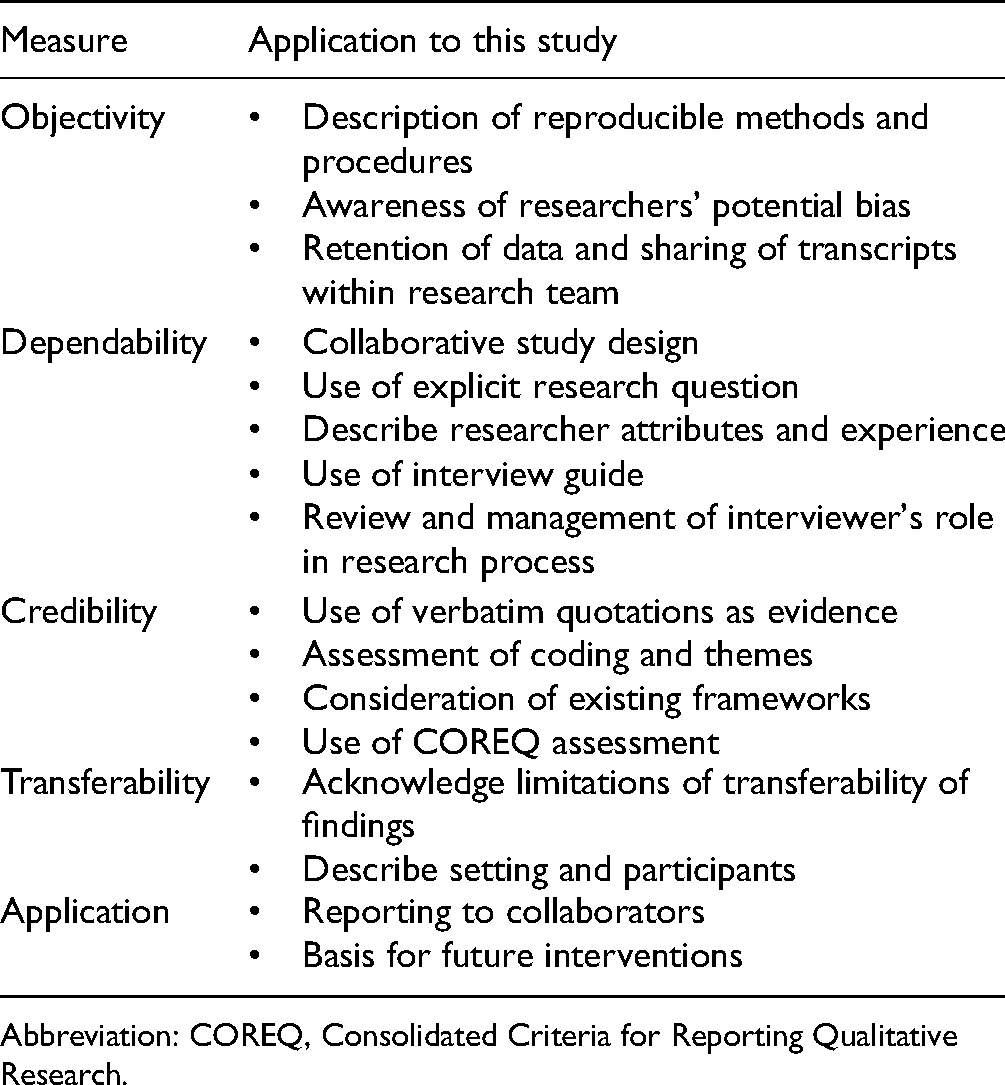
Abbreviation: COREQ, Consolidated Criteria for Reporting Qualitative Research.
Ethics
Ethics approval for the project was obtained from the Human Research Ethics Committee of Tasmania (Reference: H0018575).
Method
Participants were recruited from among patients (aged ≥18 years old) who regularly attend the Huon Valley Health Centre, a three-campus, general practice service in the Huon-Bruny Island area of Tasmania, Australia. Participants were eligible for interview invitation if they had experienced a hospital admission between July 1, 2019 and June 30, 2020 that was due to a condition listed in the Australian Institute of Health and Welfare's definition of PPH (36). An admission to hospital was defined as a stay in hospital for at least one night and excluded episodes of care where treatment was provided in the ED only (2). An invitation to participate in a semi-structured telephone interview was posted to a purposive sample (37) of 55 English-speaking patients with a PPH within the aforementioned time period, as determined from their medical records. Reminder letters were posted to nonresponders 14 days later. Written consent was obtained from 10 patients.
Semi-structured interviews were conducted by telephone by an experienced qualitative researcher (V.A.) with no prior relationship with the study population to avoid any conflict of interest or power imbalances (38,39). An interview guide was used to ensure relevant history and viewpoints of the health system were shared (Appendix 1). The interview enabled participants the flexibility to describe the background and events of their hospital admission in their own words and style.
The interviews were recorded and professionally transcribed verbatim. No participant names or identifying comments were included in the final transcript. NVIVO (QSR International Pty Ltd, Victoria, Australia, v.12) was used to manage data, assist with coding and analysis. Computer-aided and manual coding checks were performed on interview data to ensure coding consistency. Reflexive thematic analysis was applied to identify, interpret and present key patterns in the data, using the methods described by Braun and Clarke (40,41). The initial coding structure closely reflected the data before axial coding was performed and refined the coding into the final themes. All coding and thematic veracity were checked by two additional investigators.
Results
Ten patients consented to participate and were interviewed during August and September 2020 (Table 2). One patient had profound aphasia following a stroke, so his partner, who was also his full-time caregiver, participated in the interview as a proxy for the patient. Participants’ responses are denoted below by italicized, indented, and centered text. Words in square brackets were added for clarification by the investigators. The characteristics of each participant are shown in Table 3.
Characteristics of Participants and Interviews.

ENT = ear, nose, and throat.
PPH = potentially preventable hospitalisation.
Participant Characteristics.
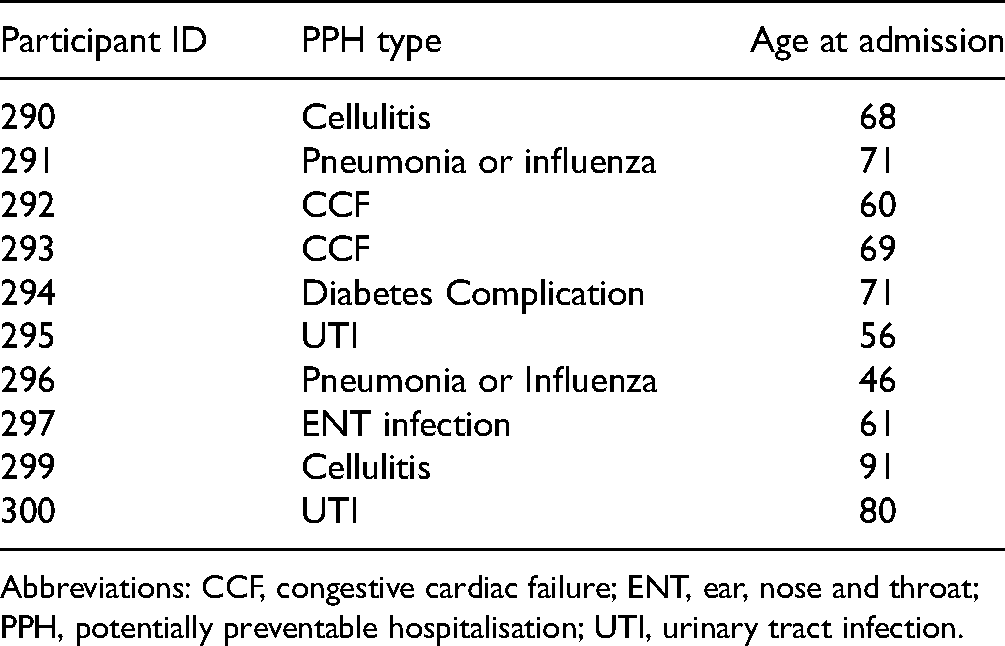
Abbreviations: CCF, congestive cardiac failure; ENT, ear, nose and throat; PPH, potentially preventable hospitalisation; UTI, urinary tract infection.
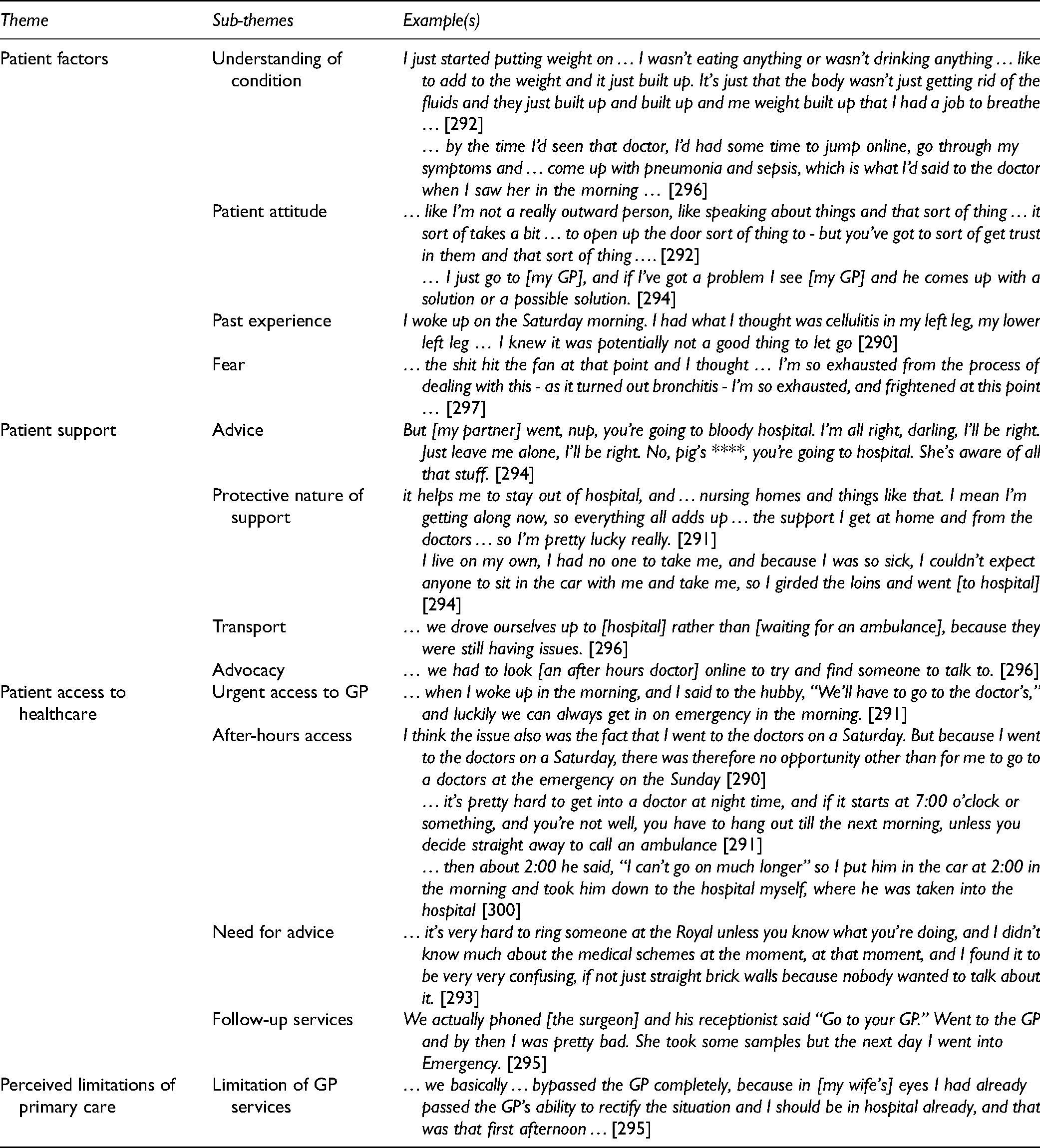
The concepts identified were condensed into four overarching themes to help understand patients’ perception of their PPH. Data that reflected several concepts were coded multiple times, possibly indicating an overlap of or a strong relationship between, ideas. Patient knowledge, beliefs, and attitude appeared substantially interdependent, so were combined into the theme of patient factors (42). The role of support in the community and access to primary healthcare services were treated as two separate themes.
Examples of themes and sub-themes are provided in Table 4. Each will now be described in greater detail.
Themes, Sub-Themes, and Example Quotes.
Patient Factors
Participants’ knowledge of the medical condition that caused their PPH was generally limited. Patients frequently failed to recognize the seriousness of their condition or conversely overestimated it. Self-diagnosis also influenced the threshold for seeking hospital treatment. I had what I thought was cellulitis in my left leg …. I knew it was potentially not a good thing to let go … Things overnight didn’t radically improve so I went to the emergency … (290)
I just go to [my GP] and if I’ve got a problem I see [my GP] and he comes up with a solution or a possible solution. (294)
Patient Support
Having connections within the community that provided advice, practical assistance, or reassurance was generally seen to be beneficial when managing an illness. Assistance in deciding when to pursue further healthcare services and what type of treatment to seek was a role frequently played by family, friends, and non-health professional community services. Sometimes, having support did not result in hospital avoidance for a PPH: But [my partner] went, ‘nup, you’re going to bloody hospital’. ‘I’m all right, darling, I’ll be right. Just leave me alone, I’ll be right’. ‘No, pig's ****, you’re going to hospital’. She's aware of all that stuff. (294) My partner is a nurse … and he was very keen for me to go. (295)
Conversely, the lack of an effective support network strongly predisposed participants to PPH. A lack of someone to provide advice, reassurance, or practical support all favored the patient requiring hospital treatment.
I live on my own… I’m so exhausted, and frightened at this point. (297)
… I couldn't contact, couldn’t find anyone, rang a few times but couldn't get any chats out of anyone. And, so, I just decided that I was getting that bad again that I just presented myself to the outpatients again. (293)
Patient Access to Primary Healthcare
The availability of primary healthcare services for acute medical issues was frequently mentioned during interviews as a determinant of PPH. Some patients had positive experiences in accessing urgent appointments with their doctor, but most found that urgently accessing a doctor was sometimes not possible. Requiring healthcare outside usual business hours (ie, overnight or during the weekend) was a common problem for these patients. … it's pretty hard to get into a doctor at night-time, and if it starts at 7:00 o’clock or something, and you’re not well, you have to hang out till the next morning (291)
The doctor saw me… and put me on an antibiotic, but with the instruction that if things didn’t radically improve then I should go to the hospital the next day … But because I went to the doctors on a Saturday, there was therefore no opportunity other than for me to go to doctors at the [hospital] emergency on the Sunday (290)
Some patients and their carers sought advice or treatment from the ambulance services with the hope or intention that this would result in transportation to and treatment in the hospital. When ambulance access was not practical, some patients were transported to the hospital by private vehicle.
Perceived Limitations of Primary Care
Some participants believed that their condition was not able to be treated appropriately in the community, and they were willing to bypass primary healthcare providers and attend the hospital. A greater variety and intensity of health services were thought to be available in the hospital. … [in my wife's] eyes I had already passed the GP's ability to rectify the situation and I should be in hospital already… (296)
Discussion
This qualitative study found that nonclinical factors played a significant role in contributing to PPHs for our rural participants. Specifically, the analysis of our rural patients’ data raised key determinants associated with PPH risk including individual patient factors of self-efficacy and health literacy, community support networks, and appropriate pathways to access primary healthcare services. SDoH are not easily captured by exploring routine health data but may be better realized through qualitative data analysis, as captured here. Identifying and confronting these risk factors may provide a source of leverage when considering interventions to reduce PPH risk, especially in the rural context where socioeconomic disadvantage is known to be more prominent (6).
The “framework for action on the social determinants of health” (World Health Organization 8) provides an explanation of how the socioeconomic parameters, such as income, education, or occupation, can shape social, economic, and political conditions. The current study reaffirms that social, financial and educational factors may have a profound impact on individual-level health and access to health services.
Ansari (3) and Saurman (7)provide useful frameworks that explain how the geographical accessibility (location) and availability (supply and demand) of services, the perceptions of acceptability, affordability, awareness, and the adequacy of service design, implementation, and evaluation all impact access to health services. Most of these dimensions were evidenced in our data.
A model developed by Bourke et al. [43] provides a framework for change in the delivery of health services in rural locations of Australia. It acknowledges that the approach to health delivery should vary between locations, and that intervention should be informed by more than a quantitative description of health data. Our study findings also align with this framework, confirming that geographical isolation, local health responses, and broader social and system factors affect each patient's perception of their healthcare journey.
Patient Enablement
PPH occurrence in this study was associated with patients possessing limited understanding of their health, treatment, and health system. Participants’ poor understanding of their health may have led to suboptimal long-term and/or acute episode management. This was exemplified by patients presenting to the hospital because they had experienced “similar” symptoms before and felt they needed to be assessed urgently. The desire for “urgent” treatment in the hospital has been observed in other qualitative studies (23,25,44). However, previous attempts to address patients’ perception of what requires urgent treatment through awareness programs, disease-specific education, or increased access to advice/triage services have had little effect on hospital usage outcomes (4).
Conversely, postponing medical assistance until the condition became unmanageable in the community may reflect an inability to recognize early warning signs. A small or nonexistent social support network may exacerbate delays in treatment as these patients have fewer health literacy resources “distributed” throughout their social network to call upon (45).
The ability to navigate the health system, including seeking information and making appropriate arrangements regarding health, was also seen as a reflection of an individual's health literacy (46). A failure to undertake any step of the “help-seeking” process (ie, identification, intention, interaction) can cause a condition to go undiagnosed, unrecognized, and untreated [47]). Each of these steps is facilitated by greater health literacy, possessed by the individual or distributed among friends and family.
PPHs associated with chronic conditions may reflect historically poor health choices and poor management of lifestyle factors (eg, smoking cessation, weight management, improved diet and exercise, addressing modifiable risk-factors) (48). Many interviewees reflected on the management of their conditions, indicating a passive, “hands-off” attitude and some demonstrated that they had little capacity to improve their immediate or future health. Proactive social supports with good health literacy may be able to compensate for a patient's disengagement to some extent; however, social isolation or having helpers with health literacy limitations themselves will increase the risk of PPHs for such patients.
A better understanding and appropriate management of one's health are important patient-level drivers required to reduce PPHs. Tasmania has lower average health literacy than the remainder of Australia (49), prompting attempts to raise the profile of health literacy at the community level and to build cooperative partnerships to improve health (50). The term “patient enablement" may be useful here as it represents an individual's ability to understand and cope with their illness and to interact with the health system (51–). Understanding the health literacy needs of the rural community may allow services to adapt and result in improved services for individuals and the community (49). Providing disease-specific education and encouraging patients to follow beneficial health recommendations are also effective in reducing PPHs (54,55). Regular use of primary healthcare services, notably GP attendance, has been associated with reduced PPHs (19,56). Patients here were noted to have high levels of trust in their “usual” GP, so promoting adherence to management recommendations during regular GP contact may be a promising means of reducing PPHs (57).
Community-Level Factors
Patient's health knowledge and management abilities are enhanced or compromised by those surrounding them. Patients living alone or without social support receive less assistance in recognizing and assessing the severity of disease symptoms and in becoming motivated to seek help. The substantial contribution that social isolation can make to PPH risk in a rural population has been observed quantitatively in the same setting (33).
A qualitative study of community-based service providers in Australia suggested functional, as opposed to structural, isolation was a driver of all-cause hospitalization, and that improving the quality of social connections may be an effective leverage point (17). The greater social capital possessed by rural communities may actually be protective against some aspects of social isolation, and thereby PPHs (10).
The presence of family and social helpers appears to be a recurring protective factor in preventing PPHs (48). Family and other social connections may notice signs of deterioration in non-isolated patients during a “pre-hospital syndrome” and arrange for earlier interventions, preventing the need for hospitalization (58). Previous studies suggest group-based, participatory interventions reduce social isolation (27), but the effect on hospital outcomes is unknown.
While patients with no social support cited this as a major factor in their PPH, the “quality” of existing social support also appears to be important. Living with family did not always seem to discourage or prevent the use of hospital services. The resourcefulness and breadth of skills among a social network may be as important as the size of an individual's social network.
High levels of combined support and knowledge possessed by an individual and their social network, however, will count for little if primary healthcare is unavailable or inaccessible in local communities.
Access and System-Level Factors
The inability to access primary care services has been reported as a significant driver of PPHs in Australia and overseas (24,26,44,59–). Many patients in this study stated that they found there were no GP appointments available at short notice or no after-hours (5 pm–8 am) services available to them. Several interviews revealed that a GP, after-hours telehealth provider, or ambulance service referred patients to the hospital when other options were not available. With generally fewer doctors and limited service availability in rural areas, it is not surprising that accessing a GP appointment is seen as a barrier to primary healthcare (2,3).
One patient noted the ability to be assessed by her GP at short notice and that services were adequate in her community, contradicting the pervasive view that rural patients struggle to book urgent GP appointments. Some literature supports this view, suggesting that the sociodemographic and health characteristics of populations are more important drivers of PPH than is the availability of primary care services (13). Whatever the true relationship, it is safe to suggest a complex interplay of local factors is likely in each rural community, which may explain the inconsistent relationship between access to primary care services and PPH occurrence.
One participant's statement regarding the benefit of increasing her disease understanding, social supports, and accessible healthcare neatly encapsulates the themes drawn from the data: Well yes, and it helps me to stay out of hospital, and helps me to stay out of nursing homes and things like that. I mean I’m getting along now, so everything all adds up together, the support I get at home and from the doctors, I only live five minutes away from them, so I’m pretty lucky really (290)
Health concerns and expecting to need further services both reflect patients’ anxiety about their health (4). Clinicians’ and laypersons’ assessments of an appropriate hospital admission often differ and help explain why patients, acting on their own perceptions and best interests, seek hospital treatment. The convenience of hospital treatment for certain conditions was not specifically mentioned in interviews although there was a recognition that the ED was always “open” with a broad range of health services “freely” available. The expectation of additional tests or procedures as a cause of PPH has been noted elsewhere in Australia (23,25), and it is reasonable to assume that this is equally, or more, important in rural populations.
This study highlights the underlying factors that patients believe are associated with their PPH. A one-size-fits-all approach to reducing PPHs is not sensible or likely to succeed. Interventions acceptable to rural patients and healthcare providers focussed on local risk factors should be considered as a means of reducing PPHs (64). Pathways to access appropriate community health services for after-hours, expected follow-up appointments and “urgent not emergent” events should be made available to all patients to help reduce acute and chronic PPHs. A “Health Literacy Mediator” (45) for rural and remote regions may be logical given their ability to simultaneously address the health literacy, support, and access issues outlined by our participants. Improving connectedness through “Social Prescribing” frameworks may help to encourage isolated and lonely patients into the sphere of existing health-literate and supportive structures (65–).
Limitations
Some patients had multiple hospital admissions; therefore, their ability to recall specific episodes may have been a limitation. However, most patients’ circumstances would not have significantly changed between hospital admissions.
An assessment of saturation was not included in the analysis process as the number of invitees consenting to participate limited the number for interviews. However, the interviews provided sufficiently rich and deep data in that patients represented a range of age groups, social support situations, and PPH admission causes. As suggested by Braun and Clarke, analyzing high “information power” data with reflexive thematic analysis makes a formal declaration of data saturation unnecessary (41).
Conclusion
This qualitative study found that health literacy, social support networks, the ability to access primary healthcare services, and perceptions of primary care were determinants of PPH risk in this rural community. While access and utilization of well-integrated primary healthcare services is a part of the solution, consideration for community- and individual-level factors also need to be addressed when considering future interventions. A thorough understanding of local health needs and appropriate leverage points is a prerequisite to improving the performance of the primary healthcare system and lowering the rate of PPH in rural Australia. Any future PPH research locally, nationally, and internationally should seek to determine which nonclinical factors patients believe led to hospitalization.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735211069825 - Supplemental material for Rural Patients’ Perceptions of Their Potentially Preventable Hospitalisation: A Qualitative Study
Supplemental material, sj-docx-1-jpx-10.1177_23743735211069825 for Rural Patients’ Perceptions of Their Potentially Preventable Hospitalisation: A Qualitative Study by Andrew Ridge, Gregory M Peterson, Bastian M Seidel, Vinah Anderson and Rosie Nash in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735211069825 - Supplemental material for Rural Patients’ Perceptions of Their Potentially Preventable Hospitalisation: A Qualitative Study
Supplemental material, sj-docx-2-jpx-10.1177_23743735211069825 for Rural Patients’ Perceptions of Their Potentially Preventable Hospitalisation: A Qualitative Study by Andrew Ridge, Gregory M Peterson, Bastian M Seidel, Vinah Anderson and Rosie Nash in Journal of Patient Experience
Footnotes
Appendix 1. Semi-Structured Telephone Interview Guide
Semi-Structured Telephone Interview Guide
Keeping Rural Tasmanians out of Hospital
A qualitative study of causes of potentially preventable hospitalisations (PPH) in southern Tasmania
Method: Semi-structured telephone interview
Location/Time/Date: to be arranged on a case-by-case basis
Interviewer: V.A.
Introduction:
Welcome to telephone interview & thanks Any initial questions (eg, risks that may be posed) Keeping Rural Tasmanians out of Hospital: A qualitative study of causes of potentially preventable hospitalisations in southern Tasmania
That is: “seeking to understand people's perspectives on (potentially avoidable) hospital admission.”
Further explanation of study (if required) Requesting more “you went to hospital for X in March 2020 – tell me why you ended up in hospital.” ** not looking for detailed medical information ** Ideas for fixing problems What did you go to hospital for? Why did you go to hospital (vs GP)? What health issues led to your recent hospital stay? What “non-medical” issues do you think led to your recent hospital stay? How could these issues be addressed (and therefore hospitalisation avoided):
by yourself? by your GP? by the health system generally? Potential for further contact for follow up interview Opportunity for questions
Project Description:
Scope of discussion:
Discussion Points (Patients):
Concluding Comments:
Thank participant
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Primary Health Tasmania (grant number CN1001).
Availability of Data and Material
Deidentified data (interview transcripts) were available to all authors throughout the project
Code Availability
Not applicable.
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Andrew Ridge. Vinah Anderson contributed to data collection. Gregory M. Peterson and Rosie Nash performed additional analysis and code checking. The first draft of the manuscript was written by Andrew Ridge and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Ethics Approval
Ethics approval for the project was obtained from the Human Research Ethics Committee of Tasmania (Reference: H0018575).
Consent to Participate and for Publication
Participants provided written informed consent to be interviewed and for deidentified publication of results.
Publication Statement
This work is not under active consideration for publication, has not been accepted for publication, nor has it been published, in full or in part
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.