
Abstract
Women’s experiences of childbirth have a significant impact on mother and child health and well-being as well as quality of care. A valid and reliable tool is needed to assess women's experience. This study aim was to adapt the Childbirth Experience Questionnaire to the Mongolian context and assess its psychometric properties. The study conducted between October and January 2019 at the public maternity hospital in Ulaanbaatar by recruiting a total of 828 low-risk postpartum women. The response rate was 92% (n = 761). Confirmatory factor analysis indicated a good fit for the 4-factor model. Reliability was good for the overall instrument (Cronbach's alpha = 0.83) and for individual domains (Cronbach's alphas ranging from 0.45 to 0.80). The overall and domain scores were significantly higher among women who had previous birth experience, who did not receive oxytocin augmentation, and who experienced a shorter labor duration (<12 h).The Mongolian version of the Childbirth Experience Questionnaire is a valid and reliable tool for exploring the childbirth experience. It can be used to promote women-centered, respectful care in maternity hospitals.
Introduction
Globally, there has been a significant reduction in maternal and child mortality (1) as maternity care services become increasingly geared toward providing high-quality, evidence-based, women-centered care to improve the health and well-being of women and their newborns (2,3). Childbirth is a momentous life event. During labor and delivery, women have various physical, psychological, and emotional experiences that have short and long-term effects on not only their own health and well-being but also the health and well-being of their newborns and families (3,4). A positive childbirth experience leads to maternal satisfaction, successful transition to motherhood, and a desire for natural vaginal childbirth in future pregnancies (5,6). Conversely, a negative childbirth experience is associated with lower rates of breastfeeding, poor maternal-infant bonding, disruptions within interpersonal relationships (7), postnatal depression (8) and posttraumatic stress disorder (9), fear of childbirth, and higher elective caesarean section rates (10).
Women's experiences of childbirth are also important from the policy perspective, as they have a significant impact on quality assessment and improvement of intrapartum care (11,12). Recently, the WHO released intrapartum care recommendations for a positive childbirth experience (3).
Mongolia has successfully reduced maternal and infant mortality, in line with Millennium Development Goals 4 and 5 (13,14). Antenatal care coverage and hospital deliveries are practically universal, accounting for 95.7% and 98.4% of all pregnant women in the country, respectively (15). So far, evaluation and improvement of maternity care quality has been based on medical records or data pertaining to health and medical service outcome indicators such as severe maternal morbidities, near-miss cases and mortality, intervention coverage, and cesarean section rates. Less attention has been given to women's views/experiences and their participation in care.
There is a dearth of research, besides a few organization-based surveys, on women's expectations and satisfaction with maternity care. Moreover, those surveys used the questionnaire that created without taking inputs from women (16–19). Therefore, a valid and reliable tool evaluating women's childbirth experiences is needed. Instruments measuring the childbirth experience are available in multiple languages (20). Among these, the Childbirth Experience Questionnaire (CEQ), a multidimensional tool created in Swedish (21) that comprehensively examines women's perceptions of childbirth care and feelings about their labor, is one of the most valid and reliable (20). It has been transculturally validated in the United Kingdom (22), Spain (23), Malaysia (24), China (25), and Iran (26).
The CEQ has been widely used to evaluate the quality of childbirth care and identify the needs that could improve women's experiences (20–23,26). Therefore, this study aimed to adapt this instrument to the Mongolian context and assess its psychometric properties (validity and reliability) among early postpartum women.
Methods
The Mongolian version of the CEQ was developed in 2 stages. In the first stage, the original instrument was translated and assessed for face and content validity. The next stage included evaluation of internal consistency and construct validity by collecting data from 761 women.
Stage I: Translation of the CEQ and Pretest
The translation procedure was performed following the principles for the translation and cultural adaptation of patient-reported outcomes outlined by Wild et al (27). This was done to ensure the grammatical soundness and terminological accuracy of the translation, as well as the preservation of the meaning and content of the original CEQ.
Two Mongolian researchers who are fluent in English independently translated the original instrument into Mongolian. Thereafter, both researchers compared their translations, reached a consensus regarding semantic, idiomatic, and conceptual equivalence, and produced the first draft of the Mongolian version of the CEQ (CEQ-M). The CEQ-M was reviewed by 5 experts in midwifery and obstetrics and gynecology with regard to the simplicity, transparency, and relevance of the items. We used the Delphi method with 2 round structural iterative communication with experts. In the first round, each expert rates and comments on the simplicity, transparency, and relevance of the items. The questionnaire was corrected for use of appropriate and transparent vocabulary, grammar, and importance of items based on their context in Mongolian. In the second round, expert made further comments on the revised version.
Subsequently, cognitive interviews were conducted with 5 postpartum women to test the understandability, interpretation, and acceptability of the questionnaire from their perspectives. Then, the researchers and expert team reviewed and amended discrepancies, thereby finalizing the CEQ-M.
Stage II: Field Study
Study setting
A cross-sectional hospital-based study was conducted at a public maternity hospital in Ulaanbaatar from October to January 2019. This is one of the 4 public maternity hospitals in the Mongolian capital. At this hospital, which accounts for approximately 25% of the deliveries in the city, the delivery rate ranges between 25 and 40 per day.
Study participants
Participants included women aged 18 to 42 years who had undergone a vaginal delivery at the maternity hospital. The inclusion criteria were: (1) women who giving birth to a healthy baby without any complications at a gestational age of 37 to 42 weeks; (2) ability to read Mongolian; and (3) willingness to participate in the study. The exclusion criteria were: (1) caesarean delivery; (2) severe pregnancy and childbirth complications such as preeclampsia, eclampsia, postpartum hemorrhage and admission to the intensive care unit; and (3) Apgar score of <7 at 5 minutes.
Data collection
Three researchers collected the data. A senior midwife from the maternity hospital created a list of eligible participants and retrieved data from medical records. A senior lecturer at the medical university and a senior student from the midwifery bachelor program recruited and collected data from eligible women who agreed to participate in the study. Postpartum women who delivered at the selected hospital and met the inclusion criteria were recruited from the postnatal wards before discharge (2-3 days after childbirth).
We collected demographic and obstetrics data and responses to the CEQ. The demographic and obstetrics data, extracted from the participants’ medical records after obtaining their permission, included age, educational background, parity, onset and duration of labor, mode of delivery, use of oxytocin augmentation, pain management, pregnancy, and childbirth complications.
Researchers who did not work at the maternity hospital proceeded to obtain informed consent, instructed participants to answer the questionnaire, and checked completeness of the questionnaire. Participants were able to freely complete the self-administered questionnaire in their room and submit it before discharge.
Study tool
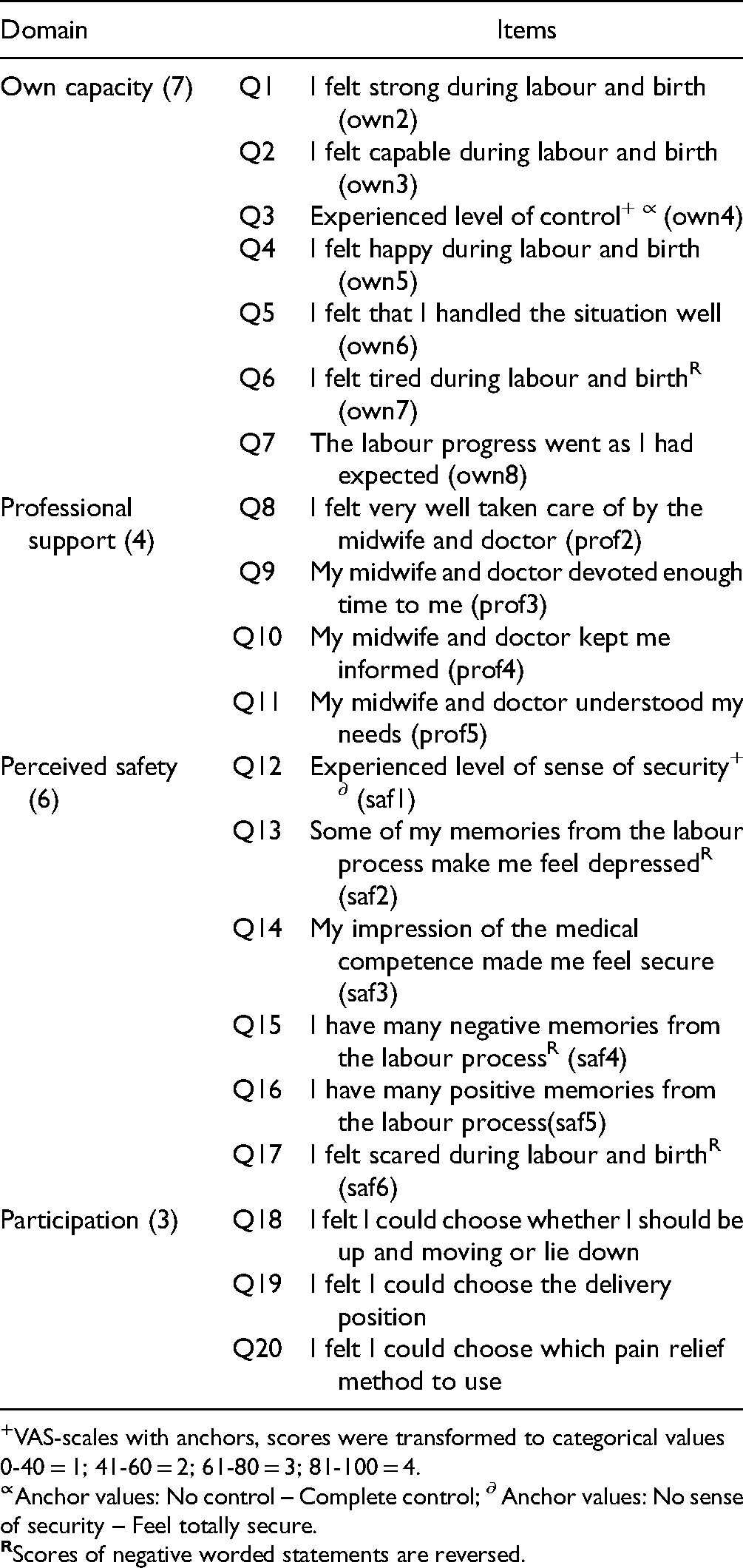
The CEQ consists of 22 items that measure 4 dimensions of the childbirth experience: own capacity (8 items), professional support (5 items), perceived safety (6 items), and participation (3 items). The responses to 19 items were scored using a 4-point Likert scale: totally agree (1), mostly agree (2), mostly disagree (3), and totally disagree (4). Three items regarding labor pain, sense of control, and sense of security were scored from 0 to 100 on a visual analog scale, where zero indicates no pain, control, or security and 100 indicates the worst imaginable pain, complete control, or feeling totally secure. These scores were converted to categorical values for scoring (0-40 = 1, 41-60 = 2, 61-80 = 3, and 81-100 = 4). The scores of the negatively worded items were reversed. The item ratings were aggregated to scale scores by summing the item score on each scale and dividing it by the number of items on the scale to obtain the mean. The score ranged from 1 to 4 points, and higher scores reflected more positive experiences. The CEQ's scoring process has been detailed in the literature (21).
Statistical and Psychometric Analyses
First, face and content validity were evaluated. Then, construct validity was assessed using confirmatory factor analysis (CFA) and validity from known-groups analysis. Reliability was assessed using internal consistency.
Content and face validity
Content validity was assessed by asking 5 experts in midwifery and reproductive health for their opinions on the clarity and feasibility of the new scale. To determine face validity, 10 postpartum women were asked to comment on the questionnaire in terms of clarity, ambiguity or possible misinterpretation of the phrases, and difficulty of the phrases and words.
Confirmatory factor analysis
The construct validity of the questionnaire was evaluated using CFA (28), adapting the 4-structure model as tested in previous studies (21). The fitness of the model was confirmed using the following thresholds: root mean square error of approximation (RMSEA) < 0.08, goodness-of-fit index (GFI) ≥ 0.90 (29,30), standardized root mean square residual (SRMR) < 0.08, comparative fit index (CFI) ≥ 0.95, Tucker-Lewis Index (TLI) ≥ 0.95 (31,32), and normed chi-square (χ2/df) <3.0 (33).
Known-groups validity
The known-groups method was used to assess construct validity based on the differences in the CEQ-M total and domain scores among the subgroups (21). Similar to previous CEQ validation studies, duration of labor, parity, and oxytocin augmentation were selected as the comparison variables. The independent Mann-Whitney U test was used to compare total and domain scores of childbirth experience among groups. The effect size was calculated by Cohen's definition (the mean difference between the 2 groups, with the result divided by the pooled standard deviation) (34). Values of 0.2 to 0.5, 0.5 to 0.8, and >0.8 were considered low, moderate, and high, respectively (34).
Reliability
Internal consistency for reliability was measured using Cronbach's alpha. Reliability was measured for 4 domains and for the overall questionnaire. Cronbach's alpha > 0.7 was considered acceptable (26,35).
Statistical software
Analysis was conducted using STATA/MP version 13.0 (STATA Corp LP, College Station, TX, USA), and P-values <.05 were considered statistically significant. CFA and SEM Building STATA were used to assess construct validity.
Result
Content and Face Validity
Based on the experts’ comments, we slightly modified some items to suit the Mongolian context. For example, we excluded the item “My midwife devoted enough time to my partner,” as it was considered irrelevant to maternity care—women giving birth at public hospitals in Mongolia are generally not allowed an accompanying person. The word “depressed” was changed to “sad” as the former has much stronger negative connotations in Mongolian. We added “doctor” after “midwife” to items 8 to 11, as in Mongolia, maternity services are led by doctors, that is, midwives accompany doctors. Another change was in the item “My midwife understood my needs”; this was modified to “My midwife and doctor understood my needs.” Table 1 represents the CEQ-M domains and included items. Regarding face validity, all women reported that the translated version was transparent, understandable, and easy to answer. The CEQ-M took 15 to 20 min to complete.
Childbirth Experience Questionnaire (CEQ) Domains and Included Items.
Participants
Of the 828 women who were initially enrolled in the study, 761 (91.9%) completed the questionnaire and their responses were included in the analysis. Table 2 presents the demographic and obstetrics characteristics of the participants. The mean age was 28.5 (±5.3) years, and over half of the sample had an educational level of college or above (64.0%), received oxytocin augmentation (53.0%), and exhibited a labor duration of <12 h (86.0%). Approximately 20% of the participants had undergone an episiotomy.
Demographic and Obstetric Characteristics of the Study Population (n = 761).

Confirmatory Factor Analysis
Figure 1 shows the 4-factor model of the CEQ-M. The minimum and maximum coefficients of the item-scale relationship were 0.31 to 0.82. All coefficients of the item-scale relationship in the CFA were significant (P < .001)—all items were significantly correlated with their factor. To improve construct validity, we eliminated the item “experienced level of labor pain in dilatation stage” as it presented the highest ceiling/floor effect and the lowest item-total correlation. The fitness indices of the CFA for the 4-factor model with 20 items are shown in Table 3. The results indicated a good model fit (RMSEA = 0.06, SRMR = 0.05, TLI = 0.88, CFI > 0.90).

Confirmatory factory analysis: The Mongolian model of CEQ.
Confirmatory Factor Analysis: Fit Indices of the CEQ-M (N = 761).
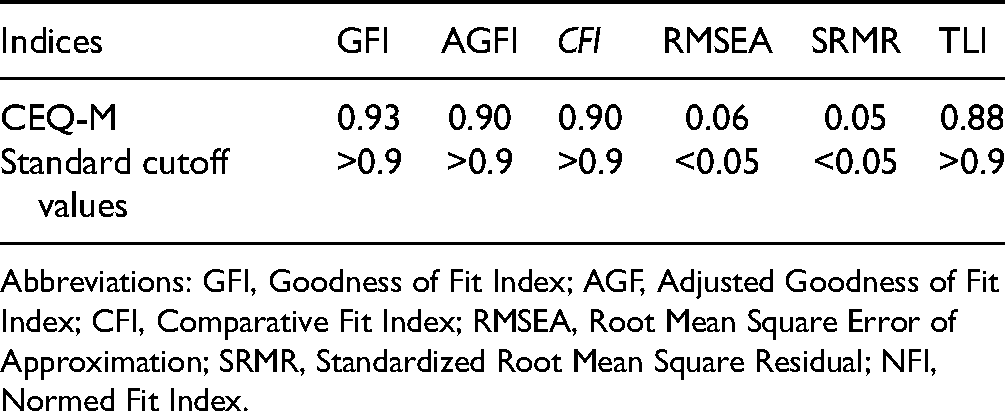
Abbreviations: GFI, Goodness of Fit Index; AGF, Adjusted Goodness of Fit Index; CFI, Comparative Fit Index; RMSEA, Root Mean Square Error of Approximation; SRMR, Standardized Root Mean Square Residual; NFI, Normed Fit Index.
Known-Groups Validation
The results of the known-groups validity assessment of the CEQ-M are shown in Table 4. The overall CEQ-M score and “own capacity” and “perceived safety” domain scores were significantly higher among multiparous than nulliparous women. Women without oxytocin augmentation during labor had significantly higher scores in the “own capacity” and “professional support” domains than those with oxytocin augmentation. Women who experienced a shorter labor duration (<12 h) reported significantly higher scores in the “own capacity” and “perceived safety” domains, compared with women who had a longer labor duration (>12 h). There were significant differences between the “own capacity” domain score and overall CEQ-M score among women who had undergone an episiotomy and those who had not. The effect sizes of these groups were small (0.2-0.4), except for the parity group (0.8). No significant differences were observed in the “participation” domain for any of the hypothesized groups.
CEQ Subscale Scores by by Groups (n = 761).

Data presented as mean (SD); Mann-Whitney U test was applied to compute P values.
Reliability
The CEQ-M's internal consistency is shown in Table 5. Cronbach's alpha for the overall CEQ-M was 0.83. Cronbach's alpha for the “own capacity,” “professional support,” “perceived safety,” and “participation” domain was 0.77, 0.80, 0.64, and 0.45, respectively. Based on these results, the CEQ-M exhibited satisfactory internal consistency.
The Reliability of the Overall CEQ-M and its Domains.

Discussion
The CEQ is widely used to assess quality of care by evaluating women's own capacity, participation, and experience with care received (36–38). The results of the current study suggest that the CEQ-M is a valid and reliable measure of childbirth experience among Mongolian women in a facility setting. The CEQ underwent an exhaustive translation process that involved a team of experts and researchers and postpartum women. Furthermore, the results showed that the CEQ-M has similar satisfactory reliability and validity to the original Swedish and adapted English versions (21,22). In this study, the Cronbach's alpha coefficient for the total scale was 0.83, which is considered acceptable and is consistent with that obtained for its Spanish (0.88), Farsi (0.93), Persian (0.85), and English versions (0.90). Moreover, the internal consistency of the subdomains was in line with previous studies where professional support and participation had the highest and lowest coefficient, respectively (22,23,26,39).
We used the original 4-factor structure for the CFA. The model indices were in accordance with standard recommendations (40).
The original CEQ has high discriminatory power between groups, indicating individual differences in the experience of childbirth. In the original instrument, the domain “own capacity” explained most of the differences between known groups, and included items concerning emotions experienced by women, sense of control, and pain (21). In this study, we found statistically higher scores with small effect sizes for the “own capacity” domain among women experiencing labor lasting <12 h and women with no oxytocin augmentation during labor compared with women who experienced longer labor and had oxytocin augmentation, respectively. These findings are similar to those of the original CEQ validation study in Sweden, as well as adaption studies in Iran, Spain, and England (21–23,26). Compared with nulliparous women, the “own capacity” domain scores were significantly higher among multiparous women. This is in line with Soriano-Vidal et al's transcultural adaption study in Spain and suggests that women with previous birth experience are more likely to have a positive experience than first-time mothers (23). In our study, we compared women who had no perineal tears/episiotomy with those who did, and found significantly higher scores for the “own capacity” domain among the former. It has been previously suggested that any operational deliveries negatively affect childbirth experience (41,42).
The “perceived safety” domain included 6 items and measured sense of security, an important area of childbirth experience. In our study, significantly higher scores for this domain were reported among multiparous women compared with nulliparous women, and women with labor lasting <12 h versus women with a longer labor duration. These findings are consistent with the CEQ adaption studies in Spain and Iran and the original study (21,23,26). Similar to previous studies (21–23), the domain scores for “professional support” were significantly higher among women with labor lasting <12 h than among those with a longer labor duration. In contrast to the original Swedish study (21) and consistent with other CEQ adaptation studies (25,43), we did not find any significant difference in the “participation” domain in the known-groups discriminant validity test.
The discriminative power of the “professional support” and “participation” domains may be explained by the inclusion of relatively few items (4 and 3 items, respectively) and a low Cronbach's alpha (0.65 and 0.45, respectively). Moreover, scores from these domains were skewed. This is commonly observed in satisfaction instruments (21,44). In this study, the reason could be that the items included in the “participation” domain were choices of pain relief methods and delivery position, which are not common practices in maternity care services in Mongolia. Moreover, as previous studies have suggested, increasing the number of items and rewording existing items or providing more response options would be a possible solution to increase the discriminative power of subscales (21,25,39,43). For instance, in the CEQ adaptation study in China, discriminant validity was improved by adding items regarding pain method, prenatal education, and companionship to the “professional support” domain.
Compared with our study, in the original CEQ study, the following were relatively higher: scores for the overall CEQ and individual domains, statistical significance, and magnitude of the effect sizes for individual domains (21). This discrepancy in results can be related to differences in the study design, participant characteristics, and childbirth context between Sweden and Mongolia. First, Dencker et al's study was a prospective clinical study, whereas ours was cross-sectional. Second, in the Swedish study, the largest effect size reported was a comparison between spontaneous vaginal birth and instrumental childbirth (including both instrumental vaginal birth and cesarean section) (21). This aspect was not included in our study as we focused on low-risk pregnant women without severe childbirth outcomes. In recent years in Mongolia, instrumental vaginal delivery has become rare, and cesarean section is conducted with medical indications (i.e., high-risk pregnant women will undergo cesarean delivery). Finally, the variability of the scores may be explained by the differences in maternal care. For instance, women's participation in childbirth is limited in childbirth care, and items in the “participation” domain included choices of pain relief methods and delivery position, which are not commonly practiced in Mongolia.
Strengths and Limitations
To the best of our knowledge, this is the first health facility-based study to quantitatively explore the multidimension domains of women's childbirth experiences by administering the CEQ in Mongolia. This study was conducted at one of 4 public maternity hospitals, recruiting a relatively homogeneous and large sample. As almost all deliveries in Ulaanbaatar take place at public maternity hospitals, the level of care, populations, and health indicators are relatively homogenous. Thus, the CEQ-M could be used for the assessment and improvement of quality of care in all Mongolian maternity hospitals. We hired 2 trained data collectors, who did not work at the hospital, to limit the response bias during data collection. We also informed the participants that their data were blinded to the hospital staff and confidentiality was secured. Additionally, participants were asked to complete the questionnaire before discharge and put it into a box. This study contributes to the existing literature by including multiparous women among the participants, which has not been done previously (23,25). It expands the limited use of the CEQ by first-time mothers to all low-risk women with a healthy pregnancy, to assess mothers’ perceptions of an uncomplicated childbirth experience regardless of parity. Lastly, we followed the patient-oriented instrument translation guidelines to achieve equivalence with the original version.
Among the limitations of this study, first is the exclusion of women with cesarean section deliveries, high-risk women, and complicated childbirths. Moreover, the study was conducted in a large public maternity hospital in an urban setting. Thus, the findings might not be applicable to primary-level hospitals or hospitals in the rural areas of Mongolia.
Conclusion
In this study, the CEQ, a multidimensional measure of women's childbirth experience, was translated into Mongolian and assessed for its psychometric properties. The findings support the validity of the CEQ-M for evaluating the quality of intrapartum care by assessing women's experiences. It promotes respectful, women-centered care by identifying their needs in health facilities and research settings. Furthermore, the CEQ-M might be useful for comparative or collaborative multi-country studies on the quality of maternal health services.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to all the participants for devoting their time to this study.
Authors’ Note
Permission was also obtained from the hospital. The research objectives were explained to the participants and they were assured of their right to withdraw from the study at any stage. Written informed consent was obtained from all participants before data collection. The study was approved by the University of Tsukuba institutional review board (IRB No.1421) and the Mongolian National University of Medical Sciences ethics committee (No. 2019/3-09). GT and TP conceptualized and designed the study and created the analysis plan. TP and BCh collected data. TP contributed to the data entry and cleaning. BTs, NN, and AKT contributed to the study implementation and logistics. GT, TP, and RKF wrote the first draft. All authors have critically read the text, contributed with inputs and revisions, and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by JSPS KAKENHI (grant number 19K19637). The funding agency had no role in the design of the study, data collection, analysis, and interpretation of data and in writing the manuscript.