
Abstract
Despite high prevalence of spine pain among the Indian population, patient expectations regarding consultation and its treatment are unknown. We aimed to determine consultation and treatment expectations among patients visiting a spine rehabilitation clinic in urban India. We included 194 consecutive patients who completed a consultation expectation (CE) and treatment outcome expectation (OE) questionnaires and the Patient-Centered Outcome Questionnaire (PCOQ). To learn about the most suitable treatment for their problem (98%), and to know what kind of activities they could do and should avoid (96%) were the most important CEs, and to achieve complete relief of symptoms (96%), and prevent recurrence of pain (95%) were the most important OEs. For successful treatment, patients expected PCOQ pain levels of 2.0 (96.5% reduction) and interference levels of 1.5 (96% reduction). Patients expected to know the most suitable treatment, activities they could do and avoid after consultation, and to achieve complete relief of symptoms and prevent recurrence after treatment. Incorporating and addressing these expectations may help improve outcomes and satisfaction with the consultation and treatment of spine pain.
Introduction
Globally, spine pain is a leading cause of disability, with a significant population affected by activity-limiting spine pain (1,2). Spine pain is considered a biopsychosocial illness where behavioral and socioeconomic factors play an important role in causation and outcomes after treatment (3,4). Considering that most cases of spine pain are secondary to “nonspecific” or nonserious mechanical causes, associated psychosocial factors need to be identified and dealt with to make its treatment more effective (5,2).
Expectations have been reported to play an important role in a patient’s physical and mental health, and patients’ expectations regarding consultation and treatment have been reported to be closely linked to their disease course and treatment outcomes (6 –8). Eklund et al (8) in a secondary analysis of a randomized controlled trial reported baseline patients’ expectations to be significant predictors of low back pain (LBP) treatment outcomes. Patients with a high expectation of improvement have greater improvement with treatment than patients with lower expectations (8). Furthermore, patient expectations regarding health care may vary between high-income and low- or middle-income countries with lower expectations from health care and greater satisfaction with poor-quality care among people in low- or middle-income countries (9). Hence, understanding patients’ expectations, specific to their socioeconomic setting, regarding the consultation and treatment process for their spine pain is important to address the psychosocial aspect of their disease and ensure better treatment outcomes.
With a population of 1.35 billion, almost 18% of the world’s population lives in India, and similar to global trends, LBP is a top cause of years lived with disability in the Indian population (10). Despite the high prevalence of LBP among its population and the significant implication of patient expectations on treatment outcomes, patient expectations have not been recorded or analyzed among the Indian population who seek assessment and treatment of their spine pain. Hence, this study aimed to determine expectations regarding consultation and rehabilitation treatment of spine pain among patients visiting a spine rehabilitation clinic in urban India.
Methods
Study Design
This study was conducted at an urban outpatient rehabilitation clinic specializing in spine rehabilitation (QI Spine Clinic, Delhi) over a 3-month period from November 2020 to January 2021. Participants who visited the outpatient clinic for assessment and physical rehabilitation treatment of their spine pain were eligible for participation in this study. The study protocol was approved by an institutional review board and ethics committee. All participants signed informed consent for participation in this study and the use of their anonymized data for research.
Study Population
Consecutive patients who came for consultation and treatment of their spine pain at our spine rehabilitation outpatient clinic were recruited for this study. The inclusion criterion was patients who presented at the clinic for consultation and treatment of their mechanical spine pain. The exclusion criteria were patients with inflammatory spine pain (spondyloarthropathies, rheumatoid arthritis), peripheral joints involvement (hip, knee, and ankle joints), patients with kyphotic or scoliotic deformities or congenital abnormalities, patients with myelopathy or peripheral neuropathy, patients who have undergone spine surgery, patients <20 years of age, and patients with incomplete clinical records.
Outcome Measures
Outcomes measures of pain, disability, expectations regarding consultation with the spine physiotherapist, and expectations regarding rehabilitation treatment were collected from all patients using self-administered scales and questionnaires in the clinic before the consultation. Pain intensity was measured using the numerical pain rating scale (NPRS) score (11) and disability using the Oswestry disability index (ODI) or neck disability index (NDI) (12,13). Based on the ODI/NDI score, patients were categorized as having minimal (0-20), moderate (21-40), or severe/crippled (>40) disability (13). Expectation questionnaires were designed by the authors to collect data about expectations regarding the consultation (CE) and expectations about treatment outcomes (OE) and were based on similar questionnaires used in previous studies on patients with spine or musculoskeletal pain (14 –19). The CE questionnaire contained 9 items related to pathology, diagnosis, prevention and treatment options, and prognosis (Supplementary Table 1). The OE questionnaire contained 8 items related to post-treatment outcomes, such as pain, functional ability in terms of activities of daily living, work, and recreational activities, and prevention of future events such as recurrence and surgery (Supplementary Table 1). All items in the CE and OE questionnaires were scored using a 5-point Likert-type scale (1 = very important, 2 = somewhat important, 3 = a little important, 4 = not important, 5 = does not apply to me).
The Patient-Centered Outcome Questionnaire (PCOQ) (20,21) was also administered to all patients prior to clinical consultation. The PCOQ was used to quantify both baseline (pretreatment) scores and post-treatment expected scores based on patient expectation across 4 domains (pain, fatigue, emotional distress, interference with daily activities) (21). The PCOQ asked patients to rate 4 items, that is, pain, fatigue or tiredness, emotional distress, and interference with daily activities at the time of consultation (usual), levels desired by the patients (desired), levels expected by the patient (expected), for the treatment to be considered successful (successful), and how important improvement is for each domain (importance) (21). The 4 items were rated on a numerical scale of 1 to 100, with 0 as none/not at all important and 100 as worst imaginable/most important (21). We also collected current ODI or NDI scores and the expected ODI or NDI scores after treatment in all patients before the start of consultation (12,13).
Demographic data including gender, age, body mass index, and lifestyle (sedentary, semiactive, or active) based on the American College of Sports Medicine recommendations (22), education (school/high school, graduation/postgraduation), occupation, medical illness, clinical presentation (central spine pain with or without radicular pain), and duration of symptoms (acute/subacute ≤12 weeks, chronic >12 weeks) were collected in all participants.
Statistical Analysis
With a margin of error set at 5%, CI at 95%, and a population size of approximately 375 patients visiting the clinic over a 3-month period (based on patients numbers for the same period from the previous year), a minimum sample size of 191 patients was determined for the study (Raosoft Sample Size Calculator). Categorical data were compared using the Fisher’s test or χ2 test, and continuous data were compared using t test or one-way analysis of variance. For subgroup analysis, percentage of patients who selected a CE or OE questionnaire item as “very important” were compared among subgroups based on gender, age (20-45 years, >45-65 years, or >65 years), education (school/high school or graduate/postgraduate), occupation (professional/self-employed or unemployed/housewife/retired), pain duration (acute/subacute or chronic), NPRS score categories (≤3, 4-7, or >7), and disability categories (minimal, moderate, or severe/crippled). Statistical analysis was performed using the GraphPad QuickCalcs online statistical analysis tool (GraphPad Software).
Results
A total of 210 patients with spine pain were evaluated during the study duration at the clinic and were eligible for participation in the study. Based on exclusion criteria, 16 patients were excluded (9 patients with inflammatory spine pain, 2 patients with peripheral joint involvement, 2 patients with congenital abnormalities, 2 patients with myelopathy, and 1 patient who was <20 years of age), and data from 194 patients with mechanical spine pain were analyzed for this study. The demographic details and clinical presentation of the study population are summarized in Table 1. A majority of the patients were males (64.5%), with active/semiactive lifestyle (59%), had graduate or postgraduate education (81%), and were either professional or employed (50%; Table 1). A majority of patients had chronic (69.5%), central spine pain (52.5%) involving the lower back (79%). A majority of the patients had an NPRS score of 4 to 7 (63%) and had moderate disability (41%) on presentation.
Demographic and Clinical Details of Study Population.a

Abbreviations: BMI, body mass index; NDI, neck disability index; ODI, Oswestry disability index; NPRS, numerical pain rating scale.
a All values are given as mean ± SD (95% CI) or number (percentage).
Expectations Regarding Consultation
Patient expectations from consultation with the attending spine physiotherapist are summarized in Figure 1. To learn about the most suitable treatment for their problem (98%), to know what kind of activities they could do and they should avoid (96%), to get a clear diagnosis or know the cause of their condition (95%), and to learn how to deal with sudden increase of pain at home or at work (95%) were the most important expectations with the consultation for the majority of the patients (Figure 1). Based on subgroup analysis, a significantly greater (P = .02) percentage of patients with chronic spine pain wanted to know a biomechanical and ‘anatomical’ explanation of their problem when compared to patients with acute/subacute spine pain (Supplementary Table 2). A significantly greater percentage of patients with NPRS score >7 wanted advice on how to return to normal activities (P = .0004), to learn how to deal with sudden increase of pain at home or at work (P = .004), and wanted to be reassured about their condition (P = .01) when compared to patients with NPRS score ≤3 (Supplementary Table 2). A significantly greater percentage of patients in the severe/crippled disability categories wanted to be reassured about their condition (P = .02) when compared to patients in the minimal disability category (Supplementary Table 2).
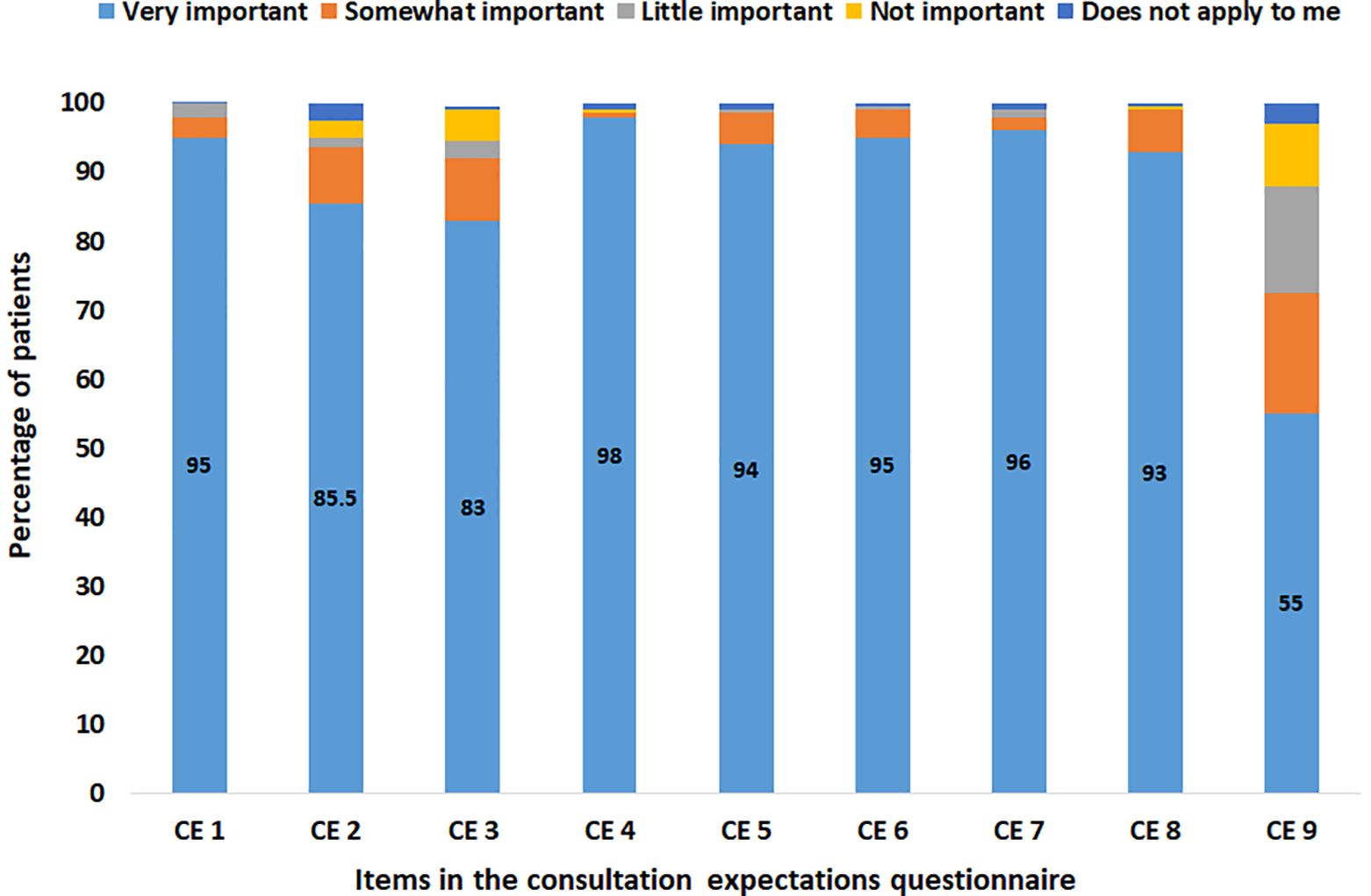
Percentage distribution of patient expectations from the consultation with the attending spine physiotherapist.
Expectations Regarding Treatment
Patient expectations regarding treatment outcome are summarized in Figure 2. To achieve complete relief of symptoms (96%), to prevent recurrence of spine pain in the future (95%), and to achieve improvement in ability to do their activities of daily living (94.5%) were the most important expectations from rehabilitation treatment for the majority of the patients (Figure 2). Based on subgroup analysis, a significantly greater percentage of males wanted to go back to their usual job (profession, occupation) (P=.0002), and to be able to drive a vehicle (P = .0002), and to be able to do exercise, play sports, or recreational activities (P = .0005) after treatment, when compared to females (Supplementary Table 3). Similarly, a significantly greater percentage of patients in the 20 to 45 years age group wanted to go back to their usual job (P=.007), and to be able to drive a vehicle (P = .01) after treatment, when compared to patients in the >65 years age group (Supplementary Table 3). A significantly greater percentage of patients who had graduate/postgraduate education wanted to go back to their usual job (P=.009), and to be able to drive a vehicle (P = .0004), and to be able to do exercise, play sports, or recreational activities (P = .02) after treatment, when compared to patients who had school/high school education (Supplementary Table 3). A significantly greater percentage of patients who are professionals or self-employed wanted to go back to their usual job (P=.0001), and to be able to drive a vehicle (P = .0005), and to be able to do exercise, play sports, or recreational activities (P = .01) after treatment, when compared to patients who were unemployed, housewives, or retired (Supplementary Table 3). A significantly greater percentage of patients with NPRS score >7 wanted to go back to their usual job (P=.006) after treatment, when compared to patients with NPRS score ≤3 and a significantly greater percentage of patients in the severe/crippled disability categories wanted to go back to their usual job (P=.0002), and wanted to prevent surgery now or in the future (P = .03) after treatment when compared to patients in the minimal disability category (Supplementary Table 3).

Percentage distribution of patient expectations regarding treatment outcome.
Patient-Centered Outcome Questionnaire Scores and Post-Treatment Expected ODI/NDI
The PCOQ scores for usual, desired, expected, successful, and importance outcomes are summarized in Table 2. The usual PCOQ score was highest for pain and interference with daily activities followed by fatigue and emotional disturbance (Table 2). For treatment to be successful, patients recorded significant reduction in scores for all the 4 domains of pain, fatigue or tiredness, emotional distress, and interference with daily activities (Table 2). However, in terms of importance, mean PCOQ score was highest for pain and interference with daily activities followed by fatigue and emotional disturbance (Table 2). For treatment to be successful, patients expected pain levels of 2.0 (96.5% reduction), fatigue levels of 1.5 (95% reduction), distress levels of 1.0 (96% reduction), and interference levels of 1.5 (96% reduction). The mean current ODI/NDI score on presentation was 30 ± 16.5 and the mean expected ODI/NDI after treatment was 3 ± 5.4 (90% reduction) in the study population.
Patient-Centered Outcomes Questionnaire (PCOQ) Scores in the Study Population.a

a All values are given as mean ± SD (95% CI).
Discussion
The findings of our study indicate that to know about and receive the most suitable treatment for their problem, to know what kind of activities they could do and they should avoid, and to get a clear diagnosis or know the cause of their condition were the 3 most important expectations from the consultation process for the majority of the patients. Furthermore, to achieve complete relief of symptoms, to prevent recurrence of spine pain in the future, and to achieve improvement in ability to do their activities of daily living were the 3 most important expectations from rehabilitation treatment for the majority of the patients.
McCarthy et al (14) in a study of 55 subjects with LBP attending a multidisciplinary rehabilitation service in the United Kingdom reported that a clear diagnosis and effective treatment were rated by patients as important expectations from the service. Similarly, a recent systematic review by Lim et al (19) where an analysis of 41 studies, all from high-income countries, indicated that clear information on the diagnosis or cause was an important expectation of patients seeking treatment for their LBP. This is in contrast to the findings of the current study where although getting a clear diagnosis was the third most important expectation from the consultation process, knowledge about the most suitable treatment was the most important expectation. The reasons for patients’ need to know the exact cause or diagnosis of their spine pain include the need for validation and legitimization of their symptoms, a belief that their pain could not be substantiated without a specific diagnosis, and a belief that a diagnosis indicated that health professionals know what they were doing (19). A possible explanation for a higher priority to know the most suitable treatment and a lower priority to know the diagnosis and other expectations among our patients could be due to the difference in socioeconomic status and its effect on patient journey through the health care system among subjects in a middle-income country like India when compared to populations primarily derived from Western, high-income countries in previous studies (19). Noncommunicable diseases like spine pain are an important cause of years lived with disability and absence from work and impose a significant financial burden on households in low- and middle-income communities (10,23). Furthermore, lack of health insurance coverage and higher out-of-pocket expenditures to access health care is prevalent in a middle-income country like India (approximately 60% in a developing country like India compared to 20%-25% in developed nations), which adds to the financial burden on patients (24,25). Hence, receiving the most suitable treatment and getting back to their work and daily life as soon as possible was the first priority rather than spending more scarce resources on investigations and knowing the diagnosis in the current study.
Bishop et al (17), in a secondary analysis of a randomized controlled trial of 140 patients with neck pain who attended a physical therapy clinic in the United States, reported moderate relief of pain, prevention of disability, and the ability to do daily activities as the top 3 patient expectations from physical therapy (exercise or manipulation) treatment. Although this was similar to findings of the current study, the majority of our patients expected complete relief of their symptoms after treatment. Expectation of complete relief from symptoms with rehabilitation treatment for spine pain has been reported to be associated with several factors such as high baseline pain and disability, sudden onset of pain, older age, and a positive impression of the treatment method (26,27). In the current study, a majority of subjects had moderate-to-severe baseline pain (86.5%) and disability (66%), which could be the reason for expectation of complete relief of pain among the majority of subjects in the current study. Furthermore, past experiences with treatment of spine pain and lack of awareness and knowledge and about the rehabilitation treatment method may lead to higher and more unrealistic expectations regarding treatment outcome (28). To be able to participate in recreational activities and to be able to drive were the least important expectations from treatment in the current study. A possible explanation for this could be that a large percentage of people in India are inactive during their leisure time with fewer than 10% engaging in recreational physical activities (29).
From their consultation, patients with chronic spine pain were more keen to understand the anatomical basis of their problem, and patients with NPRS > 7 wanted advice on return to normal activities. Interestingly, only patients with NPRS score >7 and with severe disability wanted to be reassured about their condition. Patients with chronic spine pain and higher baseline pain and disability have been reported to have a higher level of distress and catastrophizing (30,31). Hence, such patients may seek an explanation of the underlying anatomic cause of their spine pain and reassurance that the cause of their spine pain is benign. Regarding treatment, males, patients in the 20 to 45 year age group, graduates/postgraduates, professionals/self-employed individuals, and patients with NPRS > 7 or severe disability prioritized and expected to go back to their usual job, to drive a vehicle, and to be able to do exercise, play sports, or recreational activities after their treatment compared to other subgroups. Hence, based on the patient’s demographic and socioeconomic profile, expectations from spine rehabilitation treatment may vary. Demographic and socioeconomic characteristics have been reported to significantly influence expectations toward health care quality and outcomes, especially in low- and middle-income countries like India (9). Interestingly, patients with severe disability also prioritized and expected to prevent surgery in the future after their rehabilitation treatment. A possible explanation for this could be that patients seeking treatment for spine pain have been reported to have expectations of a less favorable outcome with surgical management and valued rehabilitation treatment more than other treatment methods (17,19).
The current study showed high PCOQ scores where patients required a 96.5% reduction in pain, a 95% reduction in fatigue, a 96% reduction in distress, and a 96% reduction in interference for their treatment to be considered successful. Based on PCOQ scores, O’Brien et al (32), in an analysis of 52 patients with chronic LBP attending a spine care center in the United States, reported that patients required a 58% reduction in pain levels, a 57% reduction in fatigue levels, a 67% reduction in distress levels, and a 68% reduction in interference levels for the treatment to be considered successful. These significantly higher PCOQ scores in the current study for all 4 domains could be explained by lack of knowledge or experience regarding rehabilitation treatment methods used in spine pain, which has been reported to influence patient expectations from treatment where patients naïve to treatment commonly express their expectations quantitatively (in values) rather than qualitatively (in probabilities) (28). Similarly, patients expected their ODI/NDI to reduce by 90% in the current study with could be explained by the majority of our patients having chronic symptoms (69.5%), moderate-to-severe baseline pain (86.5%), and disability (66%), which are factors reported to influence expectation of significant relief from symptoms with rehabilitation treatment (26,27).
Limitations
There are a few limitations to this study. First, patients were recruited using convenience sampling from patients visiting a spine rehabilitation clinic rather than by random sampling. However, subjects in our study included patients from a wide range of age, education, occupation, and pain and disability levels. Second, our study included patients from an urban, private outpatient clinic and hence these results may not be generalized to a government clinic/hospital or inpatient or rural population context. Third, experiences with previous treatment elsewhere may have influenced the current expectations of patients. Unfortunately detailed information regarding prior treatment in these patients was incomplete or unavailable and hence their effect of current expectations could not be analyzed. Finally, questionnaires included expectations specific to certain domains such as pain, daily activities, work, recurrence, and prognosis, which may have led to under reporting of unanticipated expectations.
Conclusion and Clinical Implications
In summary, Indian patients with spine pain had high expectations from the consultation process and physical rehabilitation treatment. Specifically, from the consultation process, most patients expected to know the most suitable treatment for their problem, the activities they could do and avoid, and to get a clear diagnosis. A majority of the patients mentioned achieving complete relief of symptoms, preventing recurrence of pain, and achieving improvement in ability to do daily activities as the most important expectations from rehabilitation treatment. The findings of our study provide baseline data on expectations regarding consultation and treatment of spine pain at a rehabilitation clinic among Indian patients. Since patient expectations may vary based on clinical presentation and socioeconomic background, all patients attending a spine rehabilitation clinic should be screened at the time of consultation to understand their expectations and preferences. Clinicians treating patients with spine pain should include patient education and counseling as part of the consultation and treatment process to address expectations and preferences, provide accurate information about treatment and expected outcomes, correct misconceptions and unhelpful beliefs, and align patients’ expectations with that of the health care provider. This will help involve patients in the decision-making process and achieve favorable treatment outcomes and patient satisfaction.
Supplemental Material
Supplemental Material, sj-pdf-1-jpx-10.1177_23743735211034076 - Patient Expectations From Consultation and Treatment of Spine Pain in a Private Spine Rehabilitation Clinic in Urban India
Supplemental Material, sj-pdf-1-jpx-10.1177_23743735211034076 for Patient Expectations From Consultation and Treatment of Spine Pain in a Private Spine Rehabilitation Clinic in Urban India by Shikha Jain, Shivani Jha, Gautam Shetty and CS Ram in Journal of Patient Experience
Footnotes
Authors’ Note
This study was approved by an institutional review board and ethics committee (ITS Institutional Ethics Committee, Ghaziabad, India).
All procedures in this study were conducted in accordance with the institutional ethics committee approved protocols.
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.