
Abstract
Patients facing situations with significant unpredictability are met with challenges to expectation formation and preparation. One such context with unpredictable clinical outcomes is bone marrow transplant (BMT) for patients with hematologic malignancies. To understand the experience of unpredictability and opportunities for intervention, semi-structured interviews with patients who had received BMT (n = 7) and transplant providers (n = 8) were conducted. Thematic analysis revealed conflict between the necessity of expectation formation and the unpredictability of transplant. Providers described a tension between adequately informing patients of potential risks of transplant and presenting so much information as to create unnecessary anxiety in patients. Patients described issues with outcome unpredictability (not knowing what particular complications they would experience) and temporal unpredictability (not knowing when complications would appear). Patients struggled to make sense of unexpected complications and resulting limitations post-BMT and plan for the future amid the nonlinear recovery timeline. The challenges of unpredictability warrant a support solution that enables patient sensemaking in their evolving illness journey and facilitates adaptation to new circumstances.
Keywords
Introduction
For many patients with hematologic malignancies, a bone marrow transplant (BMT) offers the only potential cure. However, BMT is defined by unpredictable outcomes and significant potential for morbidity and mortality. Patients and providers must navigate an unpredictable illness trajectory with an unclear prognosis, meaning patients may struggle to understand the consequences of BMT (1). BMT can lead to various acute and chronic side effects that may be life-threatening or significantly impact quality of life (2,3). The risk of various life-altering complications lasts for years after transplant, with providers unable to predict outcomes for individual patients (4,5). Consequently, patients may experience potentially debilitating uncertainty (6,7).
Patients must cope with “enduring uncertainty” (8) that extends well beyond the procedure. The unpredictability of recovery can lead to anxiety (9–12), challenges in self-management of complications (13), and frustration with the inability to plan for the future (14). Even patients who recall being warned about transplant challenges may still be surprised by and unprepared for the severity of complications, their duration, and the effects on their lives (15–17). Inconsistencies between expectations and experiences can have harmful effects on individual well-being and relationships (14,18,19). Support finding meaning in the BMT experience is desired by patients (20) and critical for effective coping (21). Yet, unpredictability makes it difficult for patients to understand what they are and will be experiencing, with current methods for patient preparation falling short. The objective of this study was to describe how patients and providers experience and manage the unpredictability of BMT to ultimately identify opportunities for support.
Method
This study used semi-structured interviews with patients who had received transplant (n = 7) and transplant providers (n = 8). All research procedures were IRB approved and participants provided written consent.
Study Participants and Setting
This research was performed at a large academic cancer center in the northeastern United States. This project was initiated by transplant providers interested in creating a decision support tool to predict personalized outcome likelihoods with BMT or with other treatments. However, as the research team became embedded in the clinic and began speaking with and observing patients and providers, we found the most difficult challenges were not around the decision but around expectations. Providers repeatedly described instances of patients returning after transplant and claiming to have been unprepared for the outcomes they experienced. Patients described the transplant “decision” as not being a true choice between two viable options—what Patient 5 described as “die or try.” This led to a shift from investigating decision-making to investigating how patients understood the experience and how providers supported patients in forming that understanding.
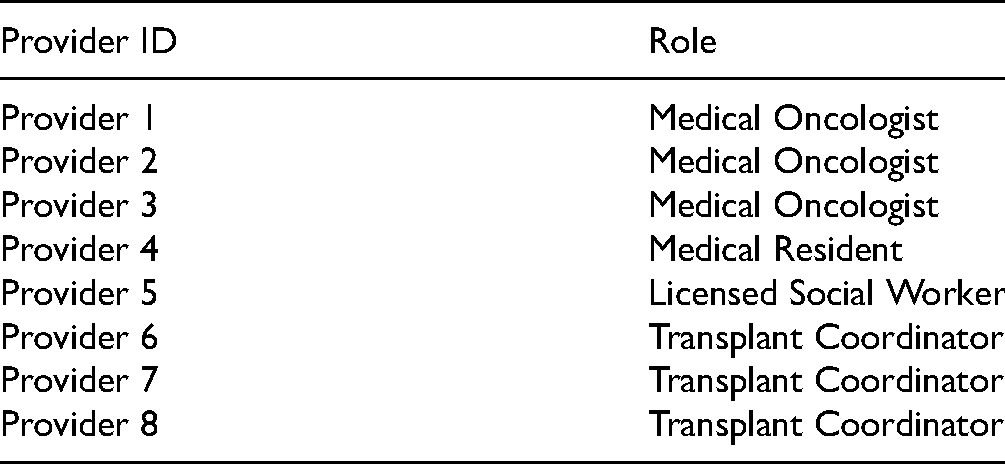
The providers interviewed had various roles within the BMT clinical team, as seen in Table 1. Providers identified patients who had received transplant and were healthy enough to participate. The research team then contacted the identified patients and asked if they would like to participate in an interview discussing their experiences with transplant. While the patients who participated had all received the same treatment, they were being treated for a range of hematologic malignancies, including acute myeloid leukemia, chronic myeloid leukemia, and chronic lymphocytic leukemia. All patients had received an allogeneic transplant, meaning they received stem cells from a donor. Patient characteristics are seen in Table 2.
Provider Characteristics.
Patient Characteristics.

Data Collection
Semi-structured interviews were performed by three members of the research team. During these interviews, providers were asked about values, communication challenges, and decision-making. Examples of questions providers were asked include: (1) What are the main challenges you face when communicating with patients? (2) What information is hardest for your patients to understand or that causes the most confusion for patients? (3) Are there topics that are uncomfortable to talk about with patients? Patients were asked about communication/information needs, decision-making, and challenges in the BMT experience. Examples of questions patients were asked include: (1) What have you found most helpful as you’ve learned about your diagnosis and treatment options? (2) What information have you found most useful in helping you understand what's going on? What information do you wish you had been given that you didn’t receive? (4) If you met someone who was recently diagnosed, what advice would you give to them? Interviews were recorded and professionally transcribed.
Data Analysis
Transcripts were imported into NVivo and analyzed using thematic analysis, a useful method for applied problems like those in health research (22). Transcripts were initially segmented for passages describing preparation and expectations. These segments were then inductively coded for emergent themes and iteratively read to solidify and condense thematic categories. Members of the research team produced analytic memos reflecting on the common themes observed in these data which were discussed amongst the team. The research team regularly discussed and refined identified themes based on individual analyses.
Results
The critical challenge for patients and providers is reconciling the unpredictability of transplant with the need for expectations. Patients and providers often shared the perception that one cannot prepare for transplant because of the unpredictability of both disease and outcomes. As one patient commented, “[i]t's impossible to lay out the trip before you even disembark” (Patient 5). Providers described concerns about their ability to effectively communicate risk information. Patients expressed challenges related to the unpredictability of which complications they might experience (outcome unpredictability) and the nonlinear recovery timeline (temporal unpredictability).
Provider Challenge: Informing Patients
Providers attempted to address outcome unpredictability by providing patients with information about all possible complications. This was accomplished through a mandatory 3–4 h long orientation class during which providers presented information on the procedure, possible complications, and other important details of recovery.
The design of the orientation class suggests that providers expect patients to understand and retain large amounts of information prior to transplant. However, providers also recognized that patients may not be able to process all of the complex information they receive in the orientation class. Patient unfamiliarity with transplant and the unpredictability of outcomes for an individual patient make it impossible for patients and providers to know what information will ultimately be relevant: I'm going to just go out on a limb and say it's like childbirth. You can't describe it. You can't know it until you're in the middle of it. You know, to say it hurts wouldn’t begin to really cover that… and that’s why, no matter what we say to these patients, they will sometimes look up and say, “Nobody told me." …Some people kind of sail through this, minimal side effects. Some people get every side effect on the list. And we don't know. We don't have a crystal ball. (Provider 5)
Providers described multiple instances of patients returning after transplant and claiming to have experienced complications they had not been warned about: Six months after [transplant, the patient] relapsed, and she started accusing me of not explaining anything about the transplant, that the possibility that the disease could come back, that I never told her any of that stuff… And it took everything… all the power in my body not to go back and grab the consent form and show her you signed here on the dotted line. By you signing here means that you’ve read everything and that you’ve heard everything that was said in the class. (Provider 7)
Instances like this, in which a patient claims to not have been informed, led providers to see the challenges of patient expectation formation as partly rooted in the information received before transplant. Still, providers recognized the difficulties of communicating this information in ways patients understand.
Communicating Unpredictability
For providers, the challenges of communicating outcome unpredictability related to (1) the quantity of complications that may result from transplant and (2) the emotional impact of this unpredictability. Providers described a tension between ensuring that patients are adequately informed and presenting so much information that it becomes “so overwhelming for the patient that they can't do anything” (Provider 3). If providers communicate all possible complications, they risk information overload, resulting in poor understanding and negatively impacting the patient–provider relationship: If you really tried to inform [patients], are you just going to scare them? (Provider 1)
The desire to avoid overwhelming patients unnecessarily conflicted with the desire to prevent later claims of not being informed. This posed a perceived threat to the doctor–patient relationship because, as Provider 3 put it, talking about the risks would “reduce that sort of bond that you have with the patient, you know? Because you're coming to see a doctor to be better.” This conflict influenced communication practices, as providers must balance obligations to inform with emotional harm: There's so many what-ifs, you know? And you can see it in a person's eyes as you speak about each what-if, they're like, “Oh my gosh”, you know? So, then I think the natural inclination is like… you kind of hedge it a little bit. But eventually they obviously do need to hear it, but the possibilities are so wide… you don't want to provoke too much anxiety in a patient on something that’s, like, 1% risk or something. (Provider 4)
Providers frequently described experiences of providing support or responding to patient emotions, consistently recognizing that “fear of the unknown” was an inevitable part of the patient experience. The information-rich orientation class intends to reduce unknowns, yet providers continued to observe patients struggle to apply this information meaningfully.
Patient Challenges: Understanding Unpredictability
Patients’ descriptions of expectation formation echoed providers in the difficulties created by the quantity and unpredictability of potential outcomes. The BMT process begins once the providers have determined that BMT may be a potential treatment option for a particular patient. Depending on the progression/severity of the disease, this discussion may occur soon after diagnosis or after the patient has first received alternative therapies to control the disease. Patients may feel physically sick from their disease or treatment at this time. Once transplant has been discussed as a possible treatment, the patient and at least one caregiver must attend the orientation class to be considered for transplant. Approximately two-thirds of this class is didactic, consisting of prepared presentations from the transplant coordinators, a social worker, and a nutritionist, with the last third consisting of a panel of the veteran patients that is intended to provide real-world experiences from people who have actually been through transplant. A significant portion of this time is spent describing the various manifestations of graft-versus-host disease (GVHD).
When patients are exposed to this information, they are still learning of the life-threatening nature of their condition, making it difficult to see past survival: I think in the beginning when the transplant option comes up, [the providers] focus on the macro which I think is survival, living. There may be micro things. For example, like your taste is going to change or your organs might shrink a little…Those are minor when you’re thinking about ‘I just want to live’…I don’t think it would be fair to say that [the providers] should tell us all of that because there’s already so much to absorb in the beginning… In the beginning it’s, you know, choose life or death and then you choose life, and then you tackle the bumps along the way. And they did say there will be bumps along the way. So, you know, there are challenges. You’re just not sure exactly which ones and when. (Patient 1)
This patient's experience brings up two important issues for patient expectations: (1) not knowing which of the many complications she will experience (outcome unpredictability) and (2) not knowing when they will arise (temporal unpredictability). The consequences of this unpredictability manifest in the practical challenges of making sense of a new reality and how to adapt.
Outcome Unpredictability
Nearly all patients were surprised by a transplant complication. Though a couple patients experienced side effects that they had not known were a possibility, they largely did not claim to have been uninformed—instead, they were surprised by the impact of the complication on their lives. All patients reported being surprised by the resulting limitations they experienced. Challenges like not being able to return to work or school within the time frame they expected or experiencing new physical disadvantages were not just viewed as consequences of transplant; they contributed to the emotional trauma of patients feeling unlike themselves: Everything’s changed. So, you can’t think of how you used to feel… It's very hard because you want that back. You want that feeling… when you were well, you know, you’re not going to feel that way ever again. You’re not going to feel the same, you’re going to be a different you. (Patient 3)
Patients did not expect the significant mental and emotional challenge of adjusting to this new life, with all patients suggesting that future patients would benefit from being more aware of this aspect of recovery. For example, one patient who experienced a common and life-altering complication known as GVHD was treated with high doses of steroids, feeling particularly despondent during this period: I just sort of felt like this was a really bad version of me as compared to before this all happened. And if I’m never going to be me again, I’m not sure I want to be that person anymore…I felt almost like an alien or something… I was not myself and I knew it, and I couldn’t do anything about it. (Patient 2)
This patient could recognize he was not himself, unsure if that would change, and powerless to do anything about it. To patients, it was not just experiencing complications of transplant that they had not expected—they were facing unexpected challenges to their identity. They did not feel prepared for navigating the world as this new self, especially in the face of continued unpredictability. Outcome unpredictability is not just a problem of determining which complication an individual patient will experience, but more broadly identifying what are the aspects of their individual contexts (goals, relationships, etc.) that are most likely to be affected.
Temporal Unpredictability
Temporal unpredictability continued to be a burden for patients well into the recovery period. Patients remain at risk for experiencing new transplant complications for years after the procedure. Therefore, it was difficult for patients to assess their progress and plan for the future: It is very frustrating… not understanding the timetable… that’s another thing I've learned about this, it's unpredictable. It's a roller coaster ride. You're up one day, you're down the next. There's good days, there's bad days. And it's nobody's fault, it's just the way it is. (Patient 7)
Even when patients recognized that providers explained they could not predetermine what complications each patient would experience, patients still struggled with the lengthy and nonlinear progression of recovery: [The providers] tell you about, oh, you might have this, you might have that in the [orientation class], but I felt like, well, if I’m a year out then I’m probably fine, and then a year and six months later something comes up…We all think of it like a disease, you just get better or you don’t get better. But this is like you get better, but you’re not ever really totally better, but hopefully you are better. And every day who knows what tomorrow's going to bring. It is a difficult thing to articulate to someone as opposed to sort of a regular type of a break a bone, the bone heals and you go back to normal. It’s not like that. (Patient 2)
Attempts to adapt to new circumstances were challenged by nonlinear progression and seeming reversals of progress. This issue was something that Patient 3, whose chronic GVHD only became an issue a year into recovery, recommended be emphasized for future patients: I felt really good and I had energy and I was like all right, well, maybe I get back to work, and then the bottom fell out. The eyes went. The joints went… Even though I know I have GVHD, that hit me like out of the blue… You know, it was after my one year, and I was feeling well… The farther out you go, the better it is. But to get to that point, then you’re going to probably have some setbacks…We’ll deal with them as they come up, which is what they say, you know, but I think they need to say… not only a doctor needs to say it, the nurse practitioner needs to say it, you know, like multiple people need to say it. (Patient 3)
This temporal uncertainty had the unexpected impact of preventing her from returning to work, even if she was feeling well—a situation she described as being “in limbo” with no endpoint in sight. Though providers may be explaining to patients pre-BMT that recovery is potentially lengthy, nonlinear, and unpredictable, patients must continuously adjust to and accept this reality.
Discussion
The unpredictability of BMT outcomes makes it difficult for patients to form expectations and for providers to prepare patients. In this study, providers attempted to address unpredictability by offering thorough information about possible outcomes before transplant. However, patients still reported surprise, feelings of unpreparedness, and unmet expectations. Providers experienced tension between informing patients and scaring them. Even when patients recalled being informed of unpredictability, they still struggled to navigate life under such circumstances. Adapting to new, surprising limitations and nonlinear recovery were persistent challenges.
The BMT population may benefit from an intervention that targets sensemaking, or the processes that people engage in to understand and act in the world around them (23). Sensemaking takes place when experiences do not match expectations (24), a common experience in BMT. Useful elements of sensemaking theories include an emphasis on context (25), the influence of past experiences (26) and emotions (27) on interpretation, and the ongoing and iterative nature of understanding over time.
Personal Relevance
While patients must receive information about complications during informed consent, they need support to understand what it means in their individual contexts. Personalized guidance, not just general information, on adapting to new limitations is important for patients in recovery (11) This is challenging because patients must learn about many complications that they may never experience. However, a support intervention that presents complications in terms of practical impact may enable patients to preemptively consider how they might adapt. For example, Patient 4 described hearing about “chemo brain” but not fully understanding what this meant until he lost his car in a parking lot. He suggested that he used to take his memory for granted, but eventually he developed “coping mechanisms” like always parking on the same side of the store. Providing patients with tools to understand the personal, practical consequences of complications can help them to prepare.
Emotional Impact
Providers described a professional obligation to inform patients of relevant risks while recognizing that covering all potential risks may seem excessively negative. For patients, it was not necessarily the complications of transplant that they were unaware of but the resulting limitations and effects on their identities. A sensemaking-support intervention could emphasize these emotional struggles. One method to enable patients to imagine emotional consequences is through narratives. Narratives of experienced patients can improve affective forecasting, or the ability to predict emotional responses to future events (28,29). Such forecasting may facilitate preparation for future coping.
Temporality
Patients and providers conceptualized challenges relating to unpredictability differently—particularly what is needed and when. Providers focused on the pre-transplant period, as they are tasked with ensuring informed consent. Patients more often described challenges after the procedure in navigating an unpredictable recovery. The unpredictabilities of transplant require an ongoing process of information support as information needs change over time (30). Further, information provided before transplant may not be relevant for months or years. An intervention to support patients in unpredictable situations would need to be accessible over the course of the illness journey. If instead of attempting to prepare patients for their possible futures, tools are designed to help them make sense of novel and confusing experiences as they come to light, we can begin to tackle the challenges of living with unpredictability.
Based on the findings presented here, a system designed to support patients in making sense of unpredictable clinical situations like BMT should be adaptive, accessible, and context-sensitive. Such a tool might utilize patient or caregiver narratives, emphasizing the delivery of timely and personally relevant information as it becomes necessary. To accomplish this, we must investigate how patients and caregivers currently interpret their experiences, what they want or need, and where this potential system fits within the illness journey. Future work should investigate the particular experiences that patients and caregivers find most meaningful and memorable in their illness experiences and how these experiences inform their expectations. Patients can be better supported in unpredictable clinical circumstances through use of a sensemaking support tool that accounts for the ways people form, evaluate, and update their expectations in response to new information and experiences.
Limitations
The present study investigated unpredictability from a multi-stakeholder perspective, exposing differences in perceptions of unpredictability and its management. However, the small sample size creates challenges for generalizability. All patients interviewed had survived, which may have created biases in interpretations of unpredictability. As in, the surprising outcomes they experienced did not have mortal consequences, despite often being life-threatening. They had the opportunity to retrospectively make sense of these experiences in ways that patients actively experiencing similar challenges may not. Further, the retrospective nature of this work limits our understanding of how expectations are being formed. Future work may look more closely at expectation formation and evolution.
Conclusion
Patients in unpredictable circumstances experience difficulties in expectation formation and in adapting to new circumstances. The unpredictability inherent to this clinical context necessitates evolving, personalized, and responsive support that enables patients and providers to iteratively make sense as clinical situations change.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Rutgers University Institutional Review Board.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Rutgers University Institutional Review Board's approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the patients and providers for their anonymized information to be published in this article.