
Abstract
The rapid development of metastatic melanoma treatment options has significantly improved overall survival, but paralleled patient educational and supportive care resources have fallen behind. Particularly, the need for grassroots programs targeting environments outside urban centers has grown. Accordingly, an environmental scan of the Durham region in Ontario, Canada, showed the lack of melanoma-specific resources for outpatients. The goal of this study was to identify the needs of metastatic melanoma patients and survivors attending a large outpatient clinic in Durham, and then develop a patient-reviewed intervention plan. Needs were assessed in 5 domains through a melanoma-specific supportive care needs assessment survey. Among 75 surveyed melanoma patients and survivors, high-level needs were identified in 3 domains: psychological, health system information, and melanoma-specific information. Furthermore, domain-specific needs were heightened in specific sociodemographic groups. Based on these survey results, a multifaceted intervention plan was developed to mitigate future needs. The intervention plan was patient-reviewed in focus groups prior to implementation, refining the developed intervention plan.
Keywords
Introduction
Despite representing only 4% of cancers, melanoma results in 80% of the skin cancer-related deaths worldwide (1). In Canada, melanoma is one of the few commonly diagnosed cancers among youth and young adults (ages 15-29) (2). Moreover, the incidence of melanoma has steadily increased at about 2% per year since 1984 for males and 1994 for females (2). Until recently, melanoma prognoses have remained dichotomized and stagnant. Although early stage 1 lesions are easily treated by excision and have 10-year survival rates over 90% (3), unresectable stage 3 and 4 metastatic tumors have historically imposed a 5-year survival rate of less than 10% (4). However, advances in metastatic melanoma treatments via immunotherapy (5 –7) and targeted therapy (8,9) have significantly improved the survival rates for late-stage melanoma patients. Expectedly, these novel treatments harbor unique adverse reactions (10) and unfortunately the essential patient education and supportive care services have fallen behind.
In addition to necessary emotional support systems (11), receiving more comprehensive information about the disease and treatment is one of the highest needs for melanoma patients (12 –14) and misinformation can be dangerous. For example, a study investigating sentinel node biopsies, a prognostic tool used to identify possible lymphatic metastases, found that only one-third of patients knew it was a prognostic tool and 15% of patients believed it was curative (14). Due to the high survival rate of early stage patients and the overall low relative incidence compared to other cancer types, melanoma patient’s supportive care needs are often unmet (15), despite having the same impact on patient health (16). In addition, melanoma patients face unique challenges such as an increased risk of developing recurrences, resulting in the need for persistent skin monitoring (17). Tackling these challenges and their looming negative psychosocial outcomes is highly dependent on the accessibility and availability of support care and educational resources. Unfortunately, regional cancer centers outside major urban centers may lack the infrastructure and personnel for cancer-specific support systems.
This problem was identified by Durham Regional Cancer Centre (DRCC) health care professionals through patient complaints. An environmental scan for on-site resources (eg, informational tools) and off-site resources (eg, support groups) was performed by speaking with cancer support centers and organizations and with specialists at the DRCC. This confirmed the lack of melanoma-specific support systems for patients and survivors in the region. Beyond health care professionals, the Internet is the most common source of information utilized by cancer patients (18,19). Despite the wealth of knowledge online, the myriad number of unregulated sources causes misinformation and unwarranted distress. The goal of this study was to identify the needs of metastatic melanoma patients and survivors attending the DRCC and subsequently develop a patient-reviewed intervention plan.
Methods
Participant Recruitment
Patient recruitment was approved by the institutional ethics board (RID # 2015-032). Participants were recruited both prospectively and retrospectively by oncologists at the DRCC. General inclusion criteria included: minimum age of 18 years, English literacy, and informed written consent. Prospective patients attending the DRCC from June 2015 to June 2016 for metastatic melanoma treatment were consented for need assessment survey completion and focus group participation—patients were given a mail return package to complete and return the survey. Retrospective patients had previously attended and been treated at the DRCC for metastatic melanoma between June 2013 to June 2015. Eligible retrospective patients were identified through electronic medical records and contacted by mail. Mail packages contained a detailed description of the study, consent forms, needs assessment survey, and prestamped return mail envelope. All returned surveys were deidentified.
Patient Survey Tools
Three short surveys tools were used to capture melanoma patient’s needs: (1) supportive care needs survey, (2) melanoma-specific supplement, and (3) additional screening questions. In total, there were 53 questions, which took about 20 minutes to complete and were comprehensible at a 10th grade (age 14-16) reading level (Supplementary A).
Although the quality of life and patient satisfaction measures can identify problems, they may not be sensitive enough to detect melanoma-specific issues (20). Instead, needs assessment surveys provide insight into the classification and magnitude of specific unmet needs (21). The Short-form Supportive Care Needs Survey (SCNS-SF34) was used to measure the supportive care and educational needs of metastatic melanoma patients and survivors. Originating from the Long-form Supportive Care Needs Survey, the SCNS-SF34 measures 5 need domains: psychological, health systems information (HSI), patient care and support (PCS), physical and daily living (PDL), and sexuality. Both surveys have been evaluated for psychometric properties and confirmed to have construct validity, 72.1% of total variance was attributed to the 5 domains, and internal reliability, Cronbach α coefficient greater than 0.8 in all domains (22,23). Moreover, the SCNS-SF34 was chosen because of its successful utilization in previous cancer needs assessment studies (24 –26). The SCNS-SF34 takes about 10 minutes to complete, is comprehensible at an eighth grade reading level, and is measured on a 5-point Likert scale: 1 = no need to not applicable; 2 = no need to satisfied; 3 = low need; 4 = moderate need; 5 = high need.
To focus the instrument on the needs of specific cancer patients, multiple cancer-specific supplementary modules have been created to be used in conjunction with the SCNS (27). The melanoma module is applicable for patients with a variety of disease severities, treatment modalities, and cancer care timelines. The module consisted of 12 melanoma-specific questions that were developed by the Supportive Care Review Group and the Centre for Health Research and Psycho-oncology (22,28). The melanoma module was confirmed to have content validity, takes about 6 minutes to complete, is comprehensible at a 10th grade reading level, and is also measured on the same 5-point Likert scale (27).
Finally, a supplementary module with 7 “yes or no” questions regarding additional information and screening behaviors was used. Five questions had been previously used in a Canadian melanoma needs assessment study (25). The remaining 2 questions were added by DRCC oncologists and asked whether participants had previously attended an information session or support group—if yes, then where they attended.
Focus Group
Focus group participants were convenience sampled in that those who consented for participation during survey completion were contacted and invited to provide feedback on a developed intervention plan based (Supplementary B). Four 60-minute sessions that consisted of an average of 5 participants per session were conducted at the Hearth Place Cancer Support Centre. Participant identities (n = 20) were anonymized, and study staff present during the focus groups signed a confidentiality agreement. Each session was audio recorded and subsequently transcribed, had the same moderators, and participants received a $5 gift card for their participation. This information was reviewed at the beginning of each focus group. Example quotes are presented verbatim.
Data Analysis
Descriptive statistics were performed as per survey administration guidelines (27), using RStudio Version 1.2.5 (29). To determine which domains reported the highest need, a Likert summated scale analysis was performed (27). Some participants did not answer every survey question, so for domain analyses the missing questions were inputted with the average need that the individual scored in the specific domain (27,30). Two-tailed t tests and chi-square, significance set at P <.05, were performed to investigate the relationships between patient needs and sociodemographic data. Focus group transcripts were thematically analyzed through a stepwise process: familiarization and coding of data, followed by forming, reviewing, and finalizing transcript themes (31).
Results
Participant Overview
Of 225 eligible prospective and retrospective patients, 75 were returned for a response rate of 33.5%. The majority of respondents were male (61.3%). Participants had an average age of 63.04 ± 10.59 and an average age at diagnosis of 60.32 ± 10.13 (n = 60). Additional sociodemographic data are summarized in Table 1.
Patient Sociodemographic Characteristics in Frequency (and Percentage).

Abbreviation: SD, standard deviation.
Needs Assessment Survey
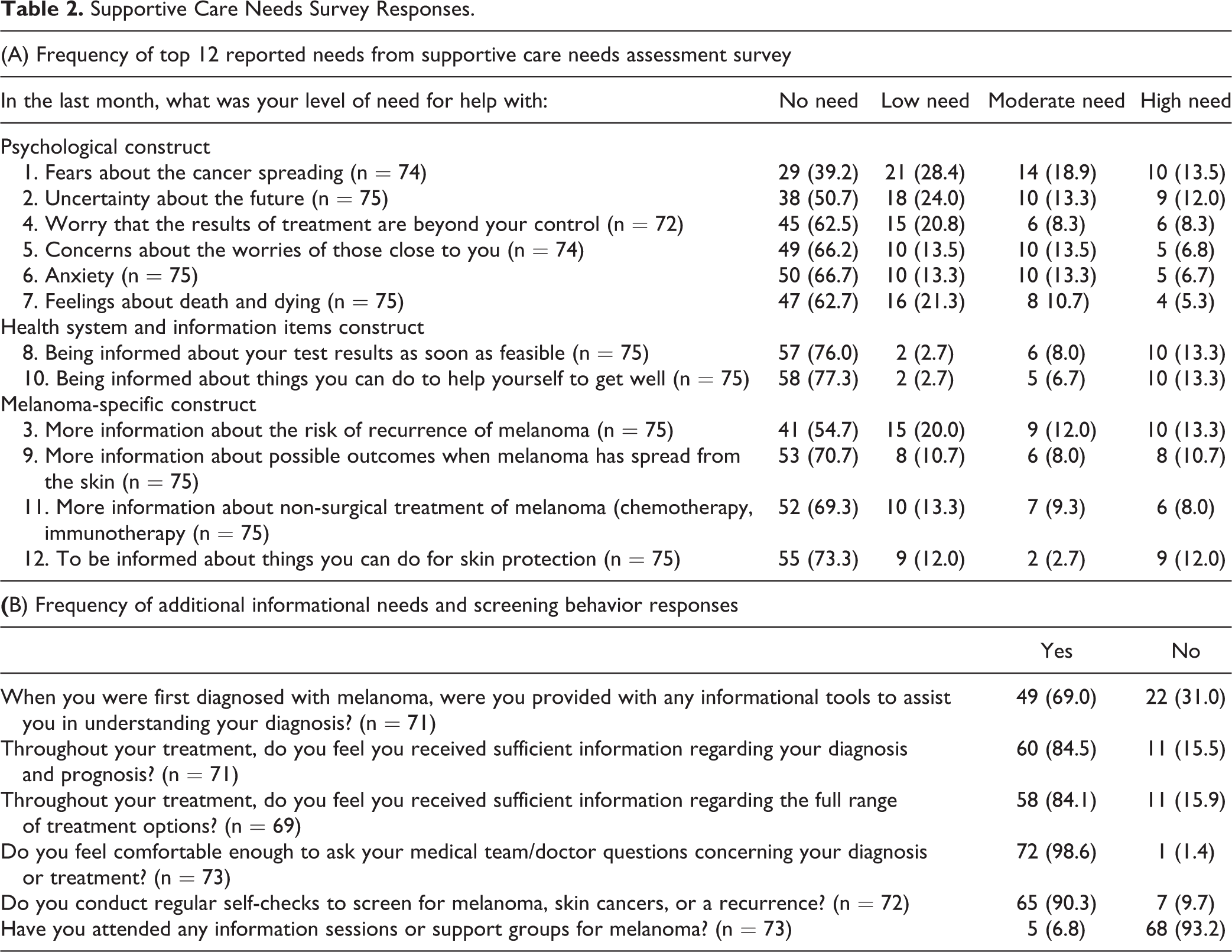
The reported domains from highest to lowest were psychological, HSI, melanoma specific, PDL, PCS, and sexuality (Figure 1). The top 12 reported needs all fell into either psychological, HSI, or the melanoma-specific domain. Six of the top 12 reported needs were in the psychological domain, including the highest reported need; fears about the cancer spreading (60.8% reported some level of need). Top reported needs are summarized in Table 2A.

Likert summated scores for constructs in SCNS-SF34 plus melanoma-specific domain. Psychological, health system, and information and melanoma-specific domains had the highest scores, indicating participants required more need in these domains compared to other domains. HIS indicates health system information; PCS, patient care and support; PDL, physical and daily living; psych, psychological.
Supportive Care Needs Survey Responses.
Sociodemographic Trends
Female participants had significantly higher needs in 4 questions: work around the home (F = 2.47, P = .019), anxiety (F = 2.26, P = .029), being given information about sexual relationships (F = 2.22, P = .035), and to be informed about the need for surgical removal of lymph nodes (F = 2.46, P = .020). Participants under the mean age of 63 years had significantly higher needs (P < .05) in 14 questions from the psychological, sexuality, or melanoma-specific domains.
Analysis of marriage variables found that those who are currently not married had significantly higher needs (P < .05) than married participants in 6 questions from either the psychological or PDL domains. Similarly, for living status, those living alone had significantly higher needs (P <.05) for 3 questions from the psychological and PDL domains. Participants who attended postsecondary school experienced significantly higher need for help with anxiety (F = 2.10, P = .039) than those with lower levels of education. Finally, individuals who are currently not working (F = 2.37, P = .022) and those living without children (F = 2.36, P = .022) had a significantly higher need for help with lymphedema than their respective counterparts. No other significant relationships were observed.
Additional Information Needs and Screening Behavior
Most patients (85.9%) were given sufficient information, but on occasion (31%), this was not done upon diagnosis. Patients felt very comfortable communicating with their health care providers (98.6%) and regularly performed skin self-checks (90.3%). Most participants (93.2%) had not previously attended a support group or informational session about melanoma. Questions and data are summarized in Table 2B. Separate chi-square analyses found no other significant relationships.
Developing an Intervention Plan
An intervention plan was built upon the major themes identified through survey results. The highest reported needs pertained to psychological, melanoma-specific, and health system information. Providing comprehensive informational support has been shown to be imperative for reducing psychological distress (32). Psychological stressors result in harmful health practices (33) such as failed treatment compliance (34) and reluctance to practice preventative behaviors (35) or seek medical advice (36). Defined as negative emotional, cognitive, and behavioral reactions experienced when confronted with a situation which exceeds available coping resources (33), psychological stress can be directly mitigated by increasing coping resources.
Psychological needs can be addressed through supportive care and have been proven to improve the psychosocial outcomes of patients (33). Informational needs can be addressed through valid and comprehensible educational resources (37) and have been proven to improve adherence to preventative behaviors and reduce psychological distress. For example, a study assessing self-skin checks found the number of patients performing the optimal frequency of checks (once every 1-2 months) doubled after an educational intervention (38).
In developing an intervention plan, a multi-faceted approach was taken. The 4 pillars of interventional techniques proven in cancer care were considered—educational, behavioral, individual psychology, and group support (39)—in conjunction with our findings of major need domains and interindividual differences identified through sociodemographic analyses.
Focus Group Themes
The proposed intervention plan (Supplementary B) was presented and 5 major themes were identified: (1) there is not much information available outside of the Internet; (2) once the melanoma diagnosis is confirmed, the treatment process is exceptional and expedited; (3) the public perception of melanoma does not complement the seriousness of the disease; (4) a mentor such as a previous patient would be the best source of support, and most participants were willing to act as a mentor for new patients; and (5) all the tools presented (Supplementary B) would have been helpful.
Focus group participants noted that oncologists explained the aspects of their disease and treatment thoroughly. Although, given the short clinic time window, every detail could not be addressed. Questions arising afterward could only be answered during follow-up visits, weeks to months later. Despite the prognostic benefits from expedited treatment upon diagnosis, patients are strained to understand the process, contributing to their perception of being ill-informed.
With respect to psychological support, most participants relied on family members, primarily spouses, to cope. Some mentioned they were offered a general cancer support group; at the time of the study, there was no melanoma-specific support group in the area. One participant outlined his concern with nonspecific cancer resources: I was given a cancer support group where I would be in with breast cancer and other cancers and I thought like melanoma as deadly as it is, it has such a high survival rate didn’t feel it was appropriate going in there. I didn’t feel like it fit me.”—Anonymous Participant
Discussion
Cancer types, subtypes, and stages are not all treated the same. Similarly, this heterogeneous population of patients have unique and specific supportive care needs. The primary goal of this study was to develop and refine an intervention plan based on self-reported needs. Pan-cancer supportive care needs analyses have found differences in patient needs between cancer types (13,40). For example, melanoma patients have an increased propensity for recurrence, requiring long-term anxiety-inducing skin monitoring (17). Supportive care research for melanoma patients in Canada is scarce compared to other regions with increased prevalence like Europe and Australia. Although important lessons can be learnt from these regions, their support resources may not always be complementary. One study found that despite one-third of melanoma patients reporting psychological and emotional distress, their needs were overlooked (33). This gap in resources was identified and tackled through a patient-reviewed intervention plan including educational resources, behavioral tools, individual, and group psychological support.
Our findings outlined the highest domains of need as psychological, health system information, and melanoma-specific support. Studies with similar patient sociodemographic distributions and survey methodology (SCNS-SF34) found the highest need domains to be psychological and melanoma-specific (24,25,27). With respect to sociodemographic variables, our findings suggest specific cohorts: female, younger, and single/living alone have significantly different needs. Female participants had significantly higher needs for work around the home, anxiety, being given information about sexual relationships, and being informed about the need for surgical removal of lymph nodes. Younger participants had significantly higher needs in the psychological, sexuality, and melanoma-specific domains. Finally, those single or living alone had significantly higher need in the psychological and PDL domains. Congruent with other studies, patients who were younger (21,24,28,41), female (28,41,42), and single or living alone (24,43) also had specific higher needs—especially in the psychological domain. Our study found that participants who had postsecondary education experienced significantly higher need for help with anxiety. In contrast, other studies have shown patients with lower education to have higher needs (44) or poorer outcomes (45). Inability to stratify our data beyond delineating by postsecondary education may explain this discrepancy.
To address the common and interindividual needs, our intervention plan heavily focused on educational and psychotherapy resources. The majority of participants (93.2%) in our study had not previously attended a support group but the possibility of speaking with others, both as the supported and supporter, was identified as extremely beneficial during focus group sessions. Comparably, a qualitative study evaluating the needs of melanoma patients found the majority of participants had not spoken to another melanoma patient (19). Only one patient had, describing their experience as an opportunity to share with someone who truly understood and believed their concerns (19). Likewise, one participant also acted as a support resource for another patient and felt this experience of counselling helped relieve their own worries (19). The same study found the primary reason patients hadn’t spoken with other patients was the lack of opportunity to do so (19). Furthermore, the major theme that patients felt that melanoma was not seen as serious as other cancers causing people to dismiss their fears has also been previously observed (19,46).
Some limitations that should be addressed are the survey tool and sampling procedures. First, while the SCNS-SF34 has been evaluated for construct validity and internal reliability (22,23,27) and the melanoma supplement has been evaluated for content validity (27), other psychometric properties have not been evaluated. Furthermore, administration of supplementary modules to the SCNS-SF34 could compromise the existing psychometric properties. Future evaluations on test–retest reliability, internal consistency, construct validity, and criterion validity for the melanoma supplement are imperative to reinforce any findings made on melanoma patients using this tool. Second, both prospective and retrospective patients returned their deidentified surveys via mail, thus any differences between these cohorts could not be assessed. Moreover, cancer patient’s psychological stressors are both complex and dynamic throughout the cancer journey (33). For example, a study using the SCNS-SF34 administered every 6 months for 2 years found the highest level of need was during diagnosis and upon recurrence events (26). Intuitively, patient needs also differ between advanced and localized disease (47). Thus, our results cannot be generalized for patients across the melanoma disease spectrum. Finally, the sociodemographic information of attending focus group participants was not recorded, thus some groups of patients or survivors may be underrepresented.
Conclusion
Over the last decade, advancements in late-stage melanoma treatment have lengthened survival for numerous patients. Though, these immunotherapeutic treatments have serious and hard to manage adverse reactions (11). This was the primary concern identified in a survey of oncologists (48). Improving patient outcomes is vital, but effective communication about disease management, prevention, and associated supportive care needs are of equal importance. Effective communication is sometimes as simple as increasing awareness. Oncologists at the DRCC can now refer patients to melanoma-specific support systems and provide a plethora of educational resources. Moving forward, DRCC patients and survivors utilizing these tools and services should be resurveyed to assess the impact and utility of the intervention plan. Continued research on the changing supportive care needs of cancer patients in a disease state-specific manner will empower patients to help themselves and others.
Supplemental Material
Supplemental Material, sj-pdf-1-jpx-10.1177_23743735211033126 - Assessing the Educational and Supportive Care Needs of Canadian Metastatic Melanoma Patients and Survivors Attending an Outpatient Clinic
Supplemental Material, sj-pdf-1-jpx-10.1177_23743735211033126 for Assessing the Educational and Supportive Care Needs of Canadian Metastatic Melanoma Patients and Survivors Attending an Outpatient Clinic by Mathushan Subasri, Manon Lemonde, Jahnavi Mundluru, Jose Chang and Rama Koneru in Journal of Patient Experience
Supplemental Material
Supplemental Material, sj-pdf-2-jpx-10.1177_23743735211033126 - Assessing the Educational and Supportive Care Needs of Canadian Metastatic Melanoma Patients and Survivors Attending an Outpatient Clinic
Supplemental Material, sj-pdf-2-jpx-10.1177_23743735211033126 for Assessing the Educational and Supportive Care Needs of Canadian Metastatic Melanoma Patients and Survivors Attending an Outpatient Clinic by Mathushan Subasri, Manon Lemonde, Jahnavi Mundluru, Jose Chang and Rama Koneru in Journal of Patient Experience
Footnotes
Authors’ Note
Data from this study are available from the author upon request.
Acknowledgments
The authors thank the participants of this study, without whom none of this would be possible; The Melanoma Network of Canada for their support and guidance; Hearth Place Cancer Support Centre for their hospitality and teamwork in running the focus groups; and the melanoma specific-support group.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding by Merck & Co. and Roche Holding AG to the Lakeridge Health research department for stationary costs regarding retrospective patient recruitment.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.