
Abstract
Patients with a chronic skin disease, eg, atopic dermatitis, need self-management skills to increase their quality of life. We explored patients’ needs for self-management support from healthcare professionals and how these needs can be met in a dermatology setting. Interpretive description methodology was chosen for iterative data collection and analysis of qualitative interviews with patients with atopic dermatitis. Two mutually dependent themes were found to be supportive of patients’ self-management. Personal and disease-related recognition was fundamental to successful support. However, guidance for agenda-setting from healthcare professionals was also needed on the wide range of topics that could be covered in the consultation based on individual needs. Patients need self-management support in addition to what can be found with family, friends, or peers. It is crucial that the support is delivered with an appreciative approach by healthcare professionals with profound knowledge of atopic dermatitis. Equally important is guidance towards agenda-setting, a way to co-construct the consultation with a clear focus on the specific patient's needs.
Keywords
Introduction
Atopic dermatitis (AD) is one of the most common chronic inflammatory skin diseases, affecting up to 20% of children and 10% of adults in high-income countries. 1 AD is characterised by episodic eczematous flares with dryness, redness, and intense pruritus, as well as a substantial impact on the lives of the patient and their family due to persistent itching, pain, sleep disturbances, and psychological and social burdens resulting in decreased quality of life.2,3 Patients with AD sometimes find self-management complex, and patient-centred professional support is often requested. 3 In a systematic review of the values and preferences of patients and caregivers to patients with AD, more than half of the identified patient-centred needs fall into the domains of psychological challenges and disease management, supporting the claim that knowledge is lacking on how to empower patients in a supportive environment while offering them the knowledge and skills to manage their disease. 4
Self-management support for patients diagnosed with AD and other chronic conditions can increase self-management skills and alleviate the burden of disease experienced by individuals and their families.5,6 In general, self-management support programmes, often referred to as therapeutic patient education in AD research, 5 consist of lectures on AD pathophysiology, trigger factors, the itch-scratch cycle, and therapeutic options. Some programs provide room for peer-to-peer discussions and training in coping strategies.5,6 Self-management support programmes can be provided in individual sessions, group sessions, a combination of the two, or sometimes e-based and remote, with duration and intensity varying from 30 min to 24 h spread out over several weeks.6,7 Ideally, access to self-management support programmes should be offered to all patients with AD, 8 but organisational and other challenges commonly result in limitations in both the frequency and scope of the programmes and a lack of integration in the patients’ routine healthcare. 6 Furthermore, self-management support programmes are designed to accommodate the general perception of problems for a given disease, and the individual patient-specific needs are not necessarily met. Thus, ongoing efforts to integrate self-management support into routine healthcare are needed. 6
There is a knowledge gap in describing patients’ perceptions of how self-management can be delivered within a dermatological setting, either in combination with self-management support programmes or alone. Therefore, this study aimed to answer the research question: What are the patient's main concerns, and how can healthcare professionals (HCPs) address the patients’ need for self-management support in consultations?
Method
Study Design
Interpretive description (ID) methodology was chosen for this qualitative study because this flexible, inductive approach is suitable when seeking the knowledge to change clinical practice justifiably. 9 ID implies iterative data collection and analysis. 9 Aiming to create in-depth knowledge of realities experienced by patients with AD, we based the study on individual patient interviews.
Setting and Inclusion of Participants
In accordance with ID, purposive sampling was used 9 to ensure maximum variation in age, gender, and disease severity. Participants were recruited from a dermatology department and a private dermatology clinic located around a university city. Recruitment was performed by four project nurses connected to the department and staff connected to the private clinic.
The number of participants was based on information power. 10 We had a broad aim, did not use specific theory, analysed across cases, had good quality dialogue, and a dense specificity, as all participants were well experienced with AD consultations. Thus, a minimum of 20 participants was estimated to redeem the complexity of our study aim.
Patient Engagement in the Study
We included a patient panel in developing the interview guide, consisting of three individuals diagnosed with AD: one male aged 30 years connected to a private dermatology clinic and two females aged 26 and 56 years connected to a dermatology department. In August 2022, all panel participants met with the first author individually by Teams to discuss the aim of the study and what subject areas were important within this aim.
The final semi-structured interview guide was field-tested in August 2022 by two individuals diagnosed with AD: two females aged 32 and 41, one connected to a dermatology clinic and one to a dermatology department.
Interview Guide
The interview guide was informed by empirical literature, input from the patient panel and clinical experiences from the authors. The authors comprise three HCPs from the dermatology speciality and one HCP specialising in person-centred diabetes care. The interview guide consisted of five focus areas: 1. everyday life, 2. experience of consultations, 3. essential topics to discuss in consultations, 4. consultation needs, and 5. HCP support of patients in consultations. The focus areas were addressed by engaging in a dialogue with the interview participants and using the 21 questions and 15 possible additional questions to form the dialogue. The interview guide can be seen in Table 1 Supplemental materials.
Characteristics of the 27 patients included in the study.

Data Collection
Twenty-seven patients were included in the study, but for patients younger than 15 years, the interview was carried out with one parent. Two patients (<15 years) were siblings, meaning only one parent was interviewed on their behalf. Thus, we ended up with 26 interview participants.
The first author conducted the interviews between September 2022 and January 2023. The 26 interviews lasted 25 to 55 min. They were conducted face-to-face (58%) or by Teams (42%) and were audio-recorded and transcribed verbatim. The purpose of the study was thoroughly explained to the participants who, after a minimum of 24-h consideration period, provided written informed consent.
The patient characteristics (Table 1) depict that the mean age in years was 28.1. Most patients included were over 15 years of age (78%), had a disease severity of moderate-severe (70%), had AD since childhood (74%) and were from the department (89%). Most patients (63%) received systemic treatments with topical treatment as an add-on when the systemic treatment alone was insufficient. There were slightly more females (56%) included in the study; however, in the interviews, two mothers and three fathers represented patients under the age of 15 years, making gender equally distributed in the interviews.
Self-Reflexive Knowledge
The researchers were aware of the potential influence of their personal or ideational beliefs on the data sources, as is crucial when using ID methodology. 9 To minimise the impact of potential biases, the authors had thorough discussions about their assumptions when creating the interview guide and before conducting the interviews. During the interviews, the interviewer (the first author) encouraged participants to elaborate on their descriptions to ensure the analysis was grounded in genuine data rather than personal or clinical assumptions. To create a safe and open environment for participants, they were assured that their responses would be kept confidential and that there were no right or wrong answers because the interviews aimed to improve clinical practice by better understanding patients’ needs for self-management support.
Data Analysis
In line with the iterative process of ID, 9 we collected and analysed data concurrently, following the typical steps: immersing oneself in the data and developing a sense of the whole beyond immediate impressions, creating broad-based and generic coding schemes and making sense of relationships between various themes with the ultimate aim of inductively building a coherent interpretive description. 9 The interviews provided 165 pages of text material, which were managed using NVivo12 software.
Credibility and Trustworthiness
As recommended in ID, 9 we used a reflective audit trail to document the process and decision-making throughout the study and enhance the credibility and rigour of the data gathering and analysis. Trustworthiness of the findings and interpretations was increased by regular analytic discussions between authors and by iteratively working with the text material and our interpretations using quotes and examples to illustrate interpretations.
The data gathering and analysis process is further illustrated in Figure 1.

Process for data analysis.
Findings
In the interviews, participants described how they managed their own or their child's AD every day, including medical treatment and preventive measures, identification of triggers that could worsen the AD, and incorporation of their experiences into daily living. Participants described how they were striving for a good quality of life but that it was difficult at times, and self-management support was needed.
The participants described different ways of gaining self-management support. Many found support in their family and friends, and some participants talked about how they found or would like to find support from peers also diagnosed with AD who could mirror their feelings and share experiences. However, the participants described that this was sometimes insufficient, and they specifically needed support from a dermatology HCP who had the knowledge and experiences to support their self-management. Nevertheless, the participants stressed that the quality and usefulness of the support from the HCP depended on recognition and guidance for agenda-setting. These two key themes will be unfolded below and substantiated with quotations in Table 2.
Exemplar quotes from the data.
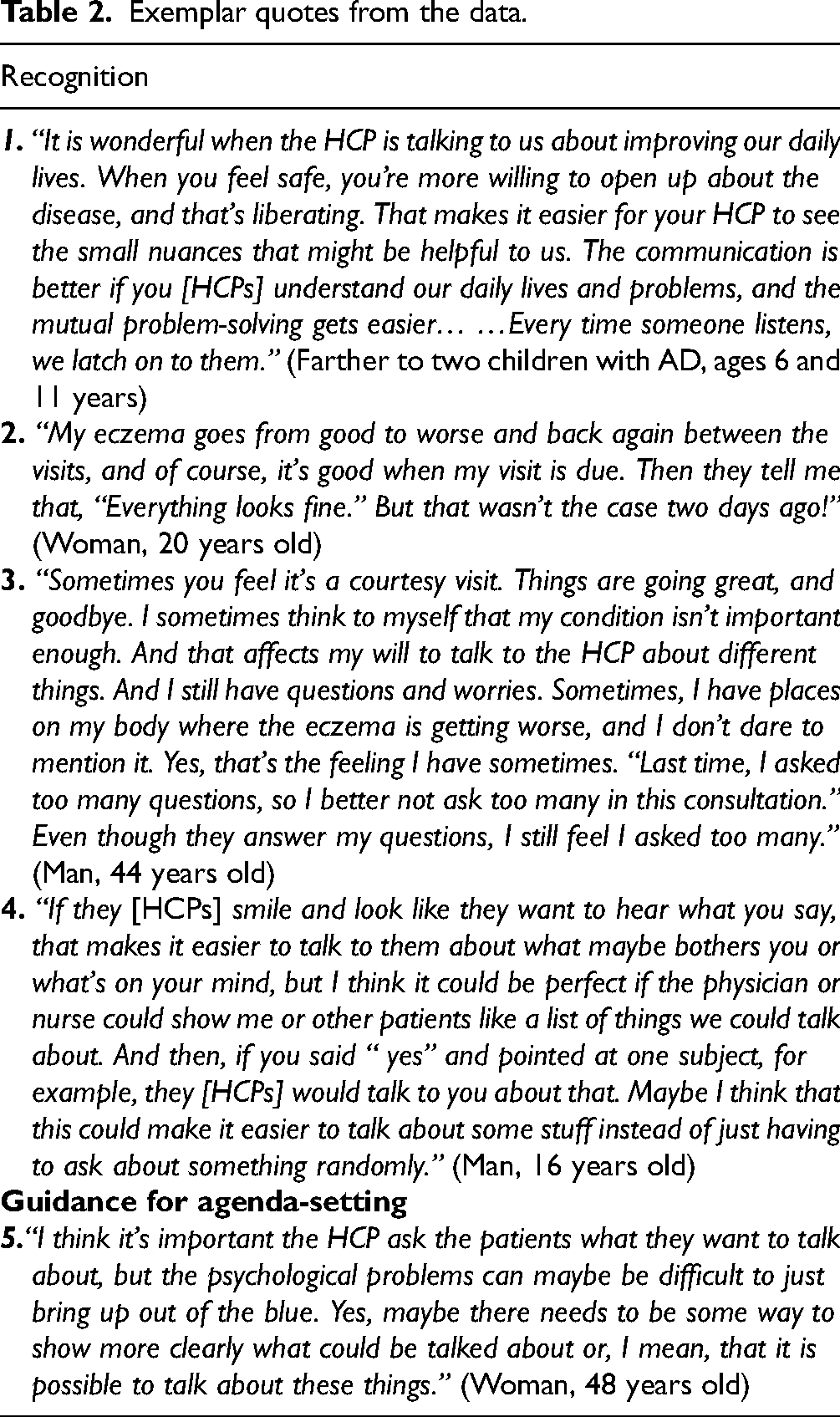
Recognition
Regardless of whether the participants had a consultation at a dermatology department or private clinic, they described both positive and negative experiences in meeting with HCPs. The usefulness of the meeting was affected by the patient's feelings of being understood, listened to, valued, trusted, acknowledged, and respected as a unique person - being recognised by the HCP. When the participants felt recognised, they were more willing to talk about the impact of the disease on their lives and the difficulties managing it. They would feel safer about showing insecurities and ask the HCP for advice and support (Table 2, quote 1).
When the participants were asked, “In which situations do you need to talk to the HCP about your eczema?” They unanimously said, “When I’m having a flare.” This answer was given because they needed help with the flare, but also because they wanted to show the HCP how their AD looked at its worst and get confirmation that the HCP understood their condition and would trust their statements in future consultations when their skin looked good even though they complained that it was not going well (Table 2, quote 2).
The participants’ need for the HCP to understand their life with AD was also reflected in the participants stressing that they would like to have a solid reference in the HCP group. It could be a physician or nurse, as long as the HCP had the knowledge and skills to support them. Furthermore, they elaborated that meeting the same person more than once would spare them from repeating the story of their AD disease course, build trust, and make them feel more comfortable talking about difficult topics, often described as psychological challenges.
The participants expressed a desire for consultations to be building blocks to which new knowledge or skills could be added each time. This desire was in our study not limited to specific characteristics of the participants, ie, age, gender, or disease severity, or to participants who only had AD for a short period or did not have control over their AD. Those who had found a way to manage the disease still described how their need for knowledge, skills, and support changed over time and how new knowledge sometimes became available, so they felt that meeting with the HCP could be essential for their self-management. The participants expressed a need for support on complex AD matters. For example, some participants were struggling with the psychological challenges of living with a chronic disease and sought support on how to deal with these feelings. While others were struggling with reconciling the life they wanted with the structured management required to manage their AD and sought support about different ways of managing symptoms of AD, trigger factors and treatments. What participants found difficult were individual and closely related to their life circumstances, and the participants were aware that they had to speak up to let the HCP know they were requesting support. However, if they did not feel recognised, they were reluctant to do so because they thought that whatever they had to say could possibly be deemed ‘not important’ by the HCP, and that would make them feel not worthy of the HCP's time (Table 2, quote 3).
In contrast, when participants described feeling recognised by the HCP, they explained how it created a foundation for discussing what they believed to be important. Nevertheless, they still described it as challenging to know what could be addressed in a consultation or how to bring up a specific topic (Table 2, quote 4).
Guidance for Agenda-Setting
When participants were asked to describe a consultation, they described a standard consultation in detail. When asked, “Is there anything you miss talking about in consultations?” almost all participants said, “No” or “I don’t know.” The participants expressed in various ways that they did not know how to respond to this question because the consultations were, in their minds, controlled by the HCP.
The participants knew they could ask questions and focus the consultation on getting specific answers. They described how HCPs often asked them if they had any questions towards the end of the consultation. However, the participants sometimes found it difficult, thinking that not all questions were possible or appropriate. In addition, they described the need to ask short and precise questions because the consultation was almost done. Furthermore, some participants expressed a need for guidance towards multiple possible topics to talk about more than the need to ask a single concrete question.
If the question from the interviewer was rephrased as, “Imagine you have no boundaries in a consultation and can say anything you like. What would be important for you to know and talk about regarding eczema?” the participants had many thoughts on different topics. Topics mentioned were, for example, everyday life with eczema, medication and treatment plans, thoughts and feelings, sexuality and intimacy, work/study/school, economy and hay fever, asthma, and food allergies. Many were closely related to individual challenges when the question was asked. Nevertheless, the topics were not limited to their own challenges, as many participants also listed topics that they themselves had found help in talking to HCPs about and from which others with AD could benefit (Table 2, quote 5).
High agreement was observed among participants regarding relevant topics; everyday life was central because it accentuated and incorporated the challenges that participants faced. Challenges in managing their disease often emerged when the patients’ AD was not in control or if their medical treatment or preventive measures were difficult to reconcile with everyday life or the people around them. Even though the participants generally agreed on topics that could be relevant to talk about in consultations, many described how it would be helpful to see the possible topics in a list or visualised in some way.
Discussion
We found that to promote self-management support in consultations, the relationship between the HCP and patient needs to be based on personal and disease-related recognition and a structure for guided involvement in agenda-setting, supporting co-construction of the consultation set-up with the patient's needs for self-management support as a starting point.
Recognition
It is evident and unsurprising that patients want an HCP with a humanistic and compassionate attitude who recognises the patient and their life with a disease.11–13 Combined with prior research, it can be assumed that feeling recognised by HCPs in consultations is a general need for patients with AD and other chronic conditions requiring continuous support.
The participants in this study wished for a solid reference in the HCP group, as also requested from patients with other chronic conditions in studies over time.14–16 Meeting different HCPs is challenging because support can be inconsistent and fragmented, and self-management is enhanced by good communication and a trusting relationship with the HCP.6,16,17 However, it can be difficult in practice to adhere to the need for one solid HCP reference, and a solution to this challenge could be a multidisciplinary team working in close alignment around a structured set of AD guidelines and in cooperation with the individual patient. The multidisciplinary team has the advantage of being more flexible, and including both nurses and physicians in self-management support may be a way to use different HCP competencies more effectively and structured to benefit patients.18,19 Nevertheless, patients in primary and secondary care settings often report a preference for seeing a physician over a nurse, suggesting that they may perceive a difference between physicians’ and nurses’ skills and knowledge.20,21 In our study, participants underlined that it was not important whether they met a nurse or a physician if the HCP had the necessary knowledge and skills to support them effectively. This indicates that it is crucial that the professionals involved in self-management support are well-trained within the field of AD and that there is an explicit agreement between professions about competencies, responsibilities, and patient communication.
Guidance for Agenda-Setting
During the last decade, agenda-setting has been proposed to ensure a mutually agreed-upon agenda that heightens patient involvement and is an essential component of improving self-management.22–26 Our study showed that participants would like to cooperate with the HCP in agenda-setting, but they need an invitation and guidance on what could be relevant to bring up in consultations. Consistently, agenda-setting has been suggested for more effective collaboration between patients and clinicians, establishing a shared focus and enabling sensitive topics that patients feel less comfortable bringing up.22–25 Yet, how mutual agenda-setting can be effectively carried out is debatable.26,27
Decision support tools, such as decision aids focusing on treatment choice, are used in many specialities to help patients decide on treatment. 28 However, far from everything in a consultation is about a specific treatment, and our study demonstrated different concerns and needs for support unrelated to treatment decisions. Various tools, such as Patient Reported Outcome Measures (PROMs),27,29,30 Question Prompt Lists (QPLs),27,31 and Conversation Cards (CCs),23,25,32 have been suggested for agenda-setting with patients suffering from different diseases. PROMs are suggested to be effective in improving physician and patient communication, disease management, and individualised treatment plans. 27 However, a study by Pattinson 29 revealed that no single PROM could comprehensively assess the impact of living with a skin condition. Moreover, to get comprehensive subjective information in Denmark, PROMs for patients with psoriasis and AD are assembled by multiple PROMs that patients are instructed to answer in the waiting room before the consultation or preferably electronically from home.20,33 This can be challenging for patients with a limited surplus 34 who may fail to follow the instructions, which is unfortunate from a principle of equality in the quality of care. The specific suggestions of QPLs can be considered a helpful inspiration and, at the same time, a possible restriction because it is challenging to encompass all relevant questions without making the list unmanageable for patients. 31 One study about QPL to patients with AD exists, albeit from 2007. 35 CCs are not necessarily problem-oriented but allow the patients to interpret a topic more freely while still focusing the conversation. 23 An advantage of CCs is that they do not require any technical skills or a large amount of preparation from the patient or HCP, and they incorporate both text and visualisation, which has been suggested to be helpful in studies of health literacy and patient materials. 36 Yet, the value of CCs is dependent on the content, design, and educational training of the HCP using the CCs.23,25 In general, more tools for agenda-setting need to be developed and tested in controlled trials to establish efficacy in improving self-management.23,27
Managing AD in a Dermatological Setting and Everyday Life
Recognition from HCPs with AD expertise and agenda-setting were found to be vital prerequisites for effective self-management support in a dermatological setting. Still, a patient typically sees HCPs only a couple of times a year, managing their disease by themselves or with family, friends, and peers for the remaining time.37,38 Furthermore, motivation for self-management is affected by personal characteristics, health status, resources, and environmental attributes, which are not necessarily static.39,40 Though an HCP cannot control all factors affecting self-management, they can contribute to self-management support by engaging in a collaborative partnership with the patient and treating each encounter as a collaborative process. 37 This entails the HCPs and patient working together to assess the patient's situation and the impact of illness on the patient's life and well-being. 37 Then, they decide the next steps based on the patient's goals and design a plan fitting them. 37 Ultimately, they carry out this plan, which entails the patients knowing what to do and how the HCP can support them until the next visit. 37 Furthermore, self-management support programmes should provide additional knowledge, skills, and peer support whenever possible and complement the individual self-management support in consultations.
Limitations
For practical reasons, we included only three patients from the private clinic, and consequently, more participants represented patients with moderate to severe eczema compared to patients with mild eczema, who are typically seen in private clinics. However, the descriptions of how self-management support can be attained in consultations by participants from the private clinic were similar to those of participants from the department. Furthermore, one participant on the patient panel and one participant in the field testing were connected to a private clinic; thus, the thoughts and views related to a private clinic were considered in creating areas and questions for the interview guide.
The study was conducted in the local context of the healthcare and welfare system, which could reduce the transferability of the findings. However, the international literature supports the study's conclusions, indicating their general nature.
It should also be noted that data from an interview is the product of a particular relationship to time and place, 9 and we must stay humble about what we have uncovered. Moreover, we must remain humble regarding generalising. While these findings may not be generalisable to all AD patients, they provide insights into a group of patients’ experiences and descriptions that are possibly similar to those being followed at other institutions.
Conclusions
In this qualitative interview study with patients suffering from AD, we contribute new knowledge about what, from the patient's perspective, is needed as a prerequisite to provide self-management support in consultations. According to our study, the effect of self-management support in consultations depends on an HCP with profound knowledge of AD who recognises the individual patients and their conditions. Recognition serves as a foundation for self-management support and, combined with guidance towards agenda-setting, affords a higher chance of focusing consultation time on the patient's needs, thereby improving self-management support. Future studies could further explore the efficacy of a patient-centred agenda-setting tool that can be used in AD consultations.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241231696 - Supplemental material for Self-management Support for Patients with Atopic Dermatitis: A Qualitative Interview Study
Supplemental material, sj-docx-1-jpx-10.1177_23743735241231696 for Self-management Support for Patients with Atopic Dermatitis: A Qualitative Interview Study by Anna Sophie Belling Krontoft, Lone Skov, Elisabeth Ammitzboell and Kirsten Lomborg in Journal of Patient Experience
Footnotes
Acknowledgements
We thank the patient panel, which greatly contributed to making an interview guide with areas relevant to the aim, as well as the patients with AD. We thank all participants who agreed to an interview and who openly shared their stories and thoughts to make clinical practice better for future patients.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Ethical Approval
The study is conducted according to the World Medical Association Declaration of Helsinki. The Danish Data Protection Agency approved the study protocol (ID no. P-2022-298). According to Danish law, the Regional Committee on Health Research Ethics does not need to be notified about qualitative studies.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Herlev-Gentofte Research Foundation [2022]; Aage Bang Research Foundation [2022]; and the Novo Nordisk Foundation [NNF22OC0079791 2022].
Statement of Informed Consent
Written informed consent was obtained from the patient(s) or from a legally authorised representative(s) for their anonymised information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.