
Abstract
Hospital medicine ward rounds are often conducted away from patients’ bedsides, but it is unknown if more time-at-bedside is associated with improved patient outcomes. Our objective is to measure the association between “time-at-bedside,” patient experience, and patient–clinician care agreement during ward rounds. Research assistants directly observed medicine services to quantify the amount of time spent discussing each patient’s care inside versus outside the patient’s room. “Time-at-bedside” was defined as the proportion of time spent discussing a patient’s care in his or her room. Patient experience and patient–clinician care agreement both were measured immediately after ward rounds. Results demonstrated that the majority of patient and physicians completely agreement on planned tests (66.3%), planned procedures (79.7%), medication changes (50.6%), and discharge location (66.9%), but had no agreement on the patient’s main concern (74.4%) and discharge date (50.6%). Time-at-bedside was not correlated with care agreement or patient experience (P > .05 for all comparisons). This study demonstrates that spending more time at the bedside during ward rounds, alone, is insufficient to improve patient experience.
Background
Ward rounds is a crucial process in the care of hospitalized adults (1 –3). Defined as “the time when the physician team meets to discuss each patient and make clinical decisions” (4), ward rounds provides an opportunity for physicians to evaluate their patients, answer questions and concerns, and ensure that the clinician team develops a shared mental model regarding a patient’s care (5 –7). Unfortunately, most of the time during ward rounds is spent away from the patient’s room, in locations such as the conference room or hallway, which may negatively impact patient outcomes and experience of care (8,9).
Interventions have been proposed to increase the amount of time clinicians spend with their patients during ward rounds. For example, bedside rounds has been advocated as an ideal intervention to facilitate effective patient–physician interactions and promote patient-centered care (10 –13). During bedside rounds, the clinician team discusses clinical updates and care plans in the presence of the patient and his or her family caregivers. In theory, this process allows for information sharing between patients and physicians, which can promote shared decision-making and improve outcomes. However, despite the intuitive benefit of bedside rounds, recent systematic reviews have shown that bedside rounds, compared to other forms of ward rounds, appears to have a no meaningful impact on patient-centered outcomes (14,15).
The lack of clear benefit from bedside rounds suggests that simply spending more time at the bedside is insufficient to promote patient-centered care. Indeed, observational data demonstrate that patient–clinician interactions at the bedside primarily involve information gathering by physicians, are filled with medical jargon, and rarely focus on the patients’ concerns and psychosocial circumstances (16 –18). If this explanation is true, interventions should focus on restructuring bedside encounters during ward rounds to facilitate patients’ involvement in their care.
This study’s overarching goal is to further our understanding of how time spent at the bedside during internal medicine (IM) ward rounds affects patient outcomes. To accomplish this goal, we proposed the following specific aims: To measure the correlation between “time-at-bedside” during ward rounds and plan of care agreement between patients, nurses, and physicians. To measure the correlation between “time-at-bedside” during ward rounds and patient experience.
Methods
Study Design, Setting, and Participants
We performed a prospective cohort study of physicians, nurses, and patients on 4 IM inpatient teaching services at Mayo Clinic Hospital in Rochester, MN, from July 1, 2016, through June 30, 2017. Each IM resident service consists of 1 attending physician, 1 postgraduate year (PGY)-3 IM resident, and 3 PGY-1 IM residents. Internal medicine resident services notify nurses via a paging system when the service is rounding on a patient for which they are caring. Nurses are encouraged to attend and participate.
For this study, we defined ward rounds as “the time when the physician team meets to discuss each patient and makes clinical decisions” (4). Ward rounds typically begins at 8:30
Sampling and Data Collection
To ensure variability in rounding practices (ie, “time-at-bedside”), we used stratified purposeful sampling when selecting IM resident services for observation (19). Specifically, services were selected based on characteristics of the attending physician, team, and rotation. Attending characteristics included years since residency graduation and professional practice (hospitalist/nonhospitalist). Team and rotation characteristics included month (July-September, October-November) and call-cycle day (on-call/postcall). Notably, these variables were selected based on prior literature, indicating their impact on time-at-bedside during ward rounds (8,20).
A trained research assistant collected data through direct observation. The unit of analysis was the patient, so the research assistant recorded the amount of time (minutes) spent in each major location on ward rounds (workroom, hallway, patient room) while reviewing and discussing each patient’s care. Based on our institution’s call structure, each unique general medicine team was observed for 3 consecutive days to ensure that all physician team members were observed and that there was adequate variability in rounding practices. Oral consent was obtained from eligible physicians, patients, and nurses before ward rounds on the day of observation.
Patients were eligible for inclusion if they were cared for by an IM teaching service. Exclusion criteria were the inability to speak English; the patient was a prisoner or residing at the Federal Medical Center in Rochester, MN, and cognitive impairment. Nurses were eligible for inclusion if they were primarily responsible for the care of an eligible patient.
Immediately following rounds, the research assistant administered a survey to the attending physician, patient, and nurse to collect the outcome variables (outlined below).
Predictor Variable: “Time-at-Bedside”
The unit of analysis was the patient, so the research assistant recorded the amount of time (minutes) spent in each major location on ward rounds (conference room, hallway, patient room) while reviewing the care for each patient. “Time-at-bedside” was calculated as the amount of time spent in a patient’s room divided by the total amount of time the team spent discussing that patient’s care.
Outcome Variables: Plan of Care Agreement and Patient Experience
Plan of care agreement
Plan of care agreement between physician, nurse, and patient was assessed using a method previously described by O’Leary et al (21,22). Immediately following ward rounds, each patient, the patient’s bedside nurse, and the attending physician were independently approached to complete a structured survey instrument regarding the plan of care. The instrument focuses on the following 7 domains: (1) patient’s principal diagnosis, (2) patient’s chief concern, (3) tests planned in the following 24 hours, (4) procedures/surgeries planned in the following 24 hours, (5) medication changes planned for today, (6) anticipated date of dismissal, and (7) discharge location (home, assisted living, skilled nursing facility).
Study investigators independently reviewed responses from patients, nurses, and physicians reviewed by 2 of 3 study investigators, and a summary agreement score (0 = no agreement, 1 = partial agreement, 2 = complete agreement) was assigned for each plan of care domain. To illustrate, below is an actual example within each agreement category for the “planned tests” domain:
Complete agreement
∘ Patient: “Computed tomography (CT) scan biopsy,” physician: “CT-guided biopsy”
Partial agreement
∘ Patient: “Check out legs—don’t know what it is called,” physician: “Vascular tests for right lower extremity”
No agreement
∘ Patient “Possible for another paracentesis,” physician: “Possible CT scan”
All responses were scored in duplicate, with disagreements resolved by consensus.
Patient experience
Patient satisfaction was measured using items adapted from the Picker Patient Experience (PPE) questionnaire (23). The PPE contains 15 items, rated on 5-point Likert scales (1 = strongly disagree, 3 = neutral, 5 = strongly agree) and was designed to measure the following dimensions of the experience of hospitalized adults: information and education, coordination of care, physical comfort, emotional support, respect for patient preferences, the involvement of family and friends, continuity and transition, and overall impression. Validity evidence supporting the use of the PPE questionnaire includes rigorous development and content validity, excellent psychometric properties and internal consistency reliability, and criterion validity, as demonstrated by a positive correlation between PPE and other patient experience measures (24).
For this study, we reviewed and selected items from the PPE-15 that were applicable to ward rounds. The items were pilot tested, and wording was modified to ensure that patients’ responses reflected their experience from ward rounds on the day of observation. Our final instrument included the following 3 items: “Based on your interaction with your medical team
Independent Variables: Characteristics of Patients, Clinicians, and Ward Rounds
Independent patient variables included resuscitation status (resuscitate/do not resuscitate/do not resuscitate and do not intubate), discharge disposition (home or skilled nursing facility), Charleston Comorbidity Index, readmission (yes/no), requiring contact precautions (yes/no), bedded on home units (yes/no), sex, age, length of stay, and education level.
Independent clinician variables included attending physician and nurse experience (years), sex, and physician specialty (hospitalist vs not). Rounding variables included nurse presence during rounds (ye/no), average duration of rounds, and average time per patient on rounds.
Data Analysis
Patient-level outcomes (communication quality, plan of care agreement) and team composition were summarized with means and SD for continuous variables, or frequencies for categorical variables. To evaluate associations between the distribution of time spent in each geographic location and the outcome variables, generalized linear mixed-effect models were used to account for the clustering of patients within a ward rounds team (25). The regression models included a random intercept shared by all patients for each ward round team, and the variability of the random intercepts was estimated. The effect of different strategies for rounds location, adjusting for observed potential confounders, was assessed using the parameter estimates in the regression model. The analysis was done in R version 3.4.2, and a P value of less than .05 was considered statistically significant.
Results
Clinician, Patient, and Rounding Characteristics
Three hundred sixteen patients were assessed for inclusion. Of these, 113 (35.8%) were included in the analysis (Supplementary figure).
Characteristics of the patients, as well as clinician and rounding characteristics, are summarized in Table 1. Additionally, the majority of patients had at least a high school education (76 [88.4%]), were full code (97 [85.8%]), were newly admitted to the hospital during the date of observation (57 [50.4%]), and were discharged to home (88 [78.8%]; data not shown). For each patient observed during rounds, the clinician team spent most of the time outside of the patient’s room (60.05%), either in the conference room or hallway.
Patient, Clinician, and Rounding Characteristics.

Clinician–Patient Agreement
Clinician–patient agreement scores are shown in Figures 1 and 2 and in Supplementary table. Following ward rounds, the majority of patient and physicians completely agreed on planned tests (66.3%), planned procedures (79.7%), medication changes (50.6%), and discharge location (66.9%), but disagreed on the patient’s main concern (74.4%) and discharge date (50.6%). The majority of nurses and patients completely agreed on discharge location and planned tests and procedures, but disagreed on the patient’s chief concern.
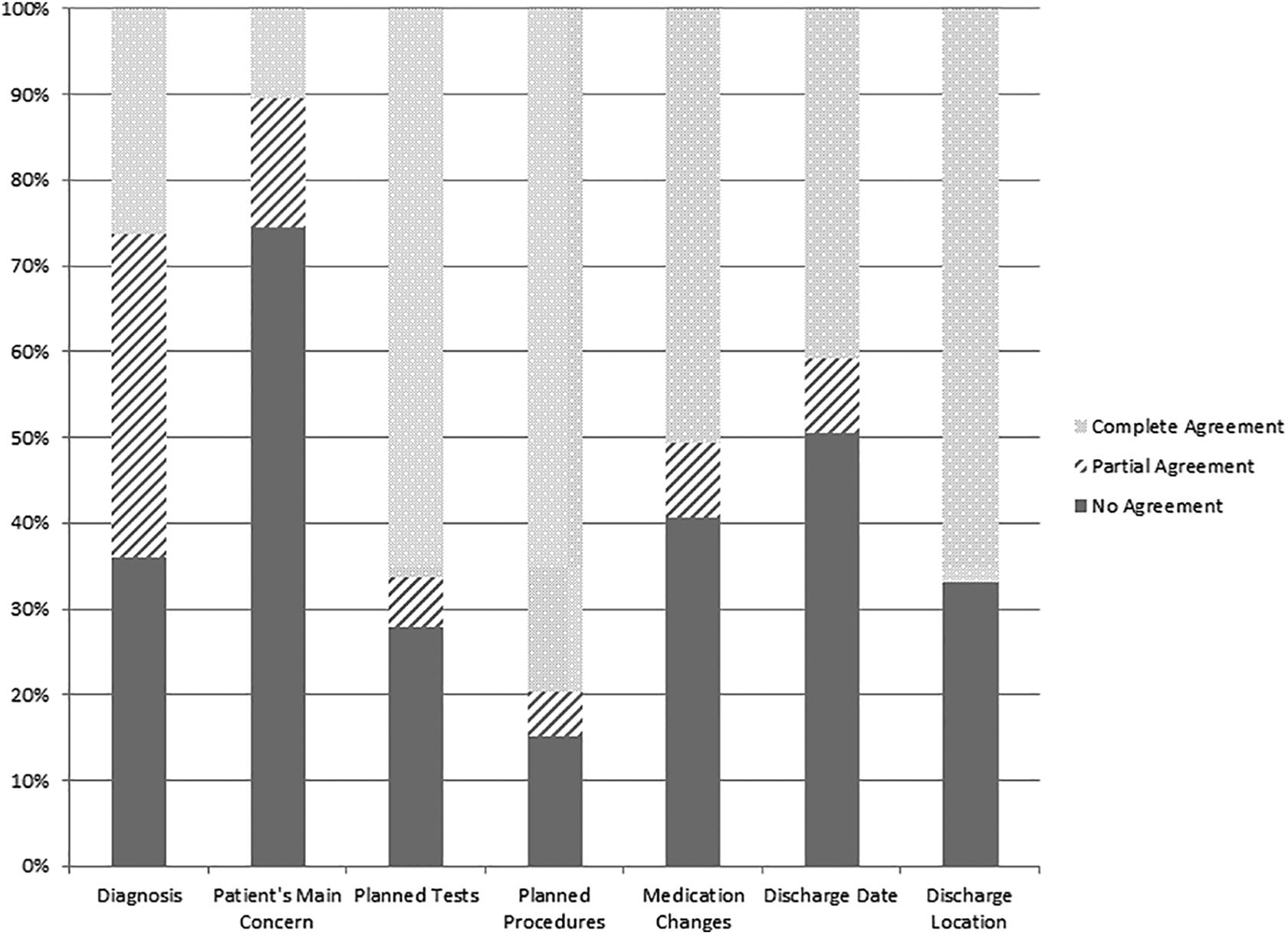
Physician–patient plan of care agreement.

Nurse–patient plan of care agreement.
Associations Between Time-at-Bedside, Clinician–Patient Agreement, and Patient Experience
Generalized regression models were created to assess for associations between time-at-beside and clinician, patient, and rounding characteristics (data not shown). In the unadjusted model, having postgraduate education was positively associated with time-at-beside (β [SE], .33 [0.09]; P <.001), while total time per patient was negatively associated with time-at-bedside (β [SE], −.008 [0.002]; P < .001).
Associations between time-at-bedside, patient–physician agreement, and patient experience are provided in Table 2. Additionally, there were no statistically significant associations between time-at-bedside and patient–nurse or nurse–physician agreement for any of the plan of care items (data not shown).
Associations between Time-At-Bedside and Plan of Care Agreement, and Time-At-Bedside and Patient Experience.

Discussion
Our objective was to measure the relationships between the proportion of time spent at the bedside during ward rounds, patient–clinician plan of care agreement, and patient experience. Using direct observation, we found that physician teams spend most of the time discussing their patients’ care away from the bedside. Additionally, although patients’ experience during ward rounds was generally positive, their agreement with their doctor and nurse regarding essential care items was low. However, we found no relationship between the amount of time spent in the patients’ room and the level of agreement or patient experience. These findings have important implications for hospital-based clinicians.
Integration and Interpretation of the Findings
Our results are consistent with prior research showing that hospitalized patients have a limited understanding of their diagnoses and treatment plans (21,26 –30). Additionally, we found that physicians and nurses are often unaware of their patients’ main concerns. The reasons for our findings are unclear but may be related to several factors. First, medical jargon is ubiquitous during ward rounds and may limit patients’ ability to understand and participate in the conversation regarding their care (16,17,31 –33). Second, interactions during ward rounds are often dominated by physicians, with little opportunity for patients to ask questions or seek clarification (16,31). Third, patients with acute medical illnesses may have distracting physical and psychological symptoms, limiting their ability to comprehend and retain information (18). Lastly, hospitalized patients often have personal concerns that extend beyond their principal diagnosis. However, observational research demonstrates that, when confronted with patients’ psychosocial concerns during rounds, physicians often respond in a neutral or minimalistic manner (34).
The results of this study also reinforces research evidence, demonstrating that the quality of a bedside encounter, rather than time alone, has the greatest positive effect on patients’ experience of care. For example, one experiment demonstrated that when physicians sit, rather than stand, at the bedside, postoperative patients perceived that the physician spent more time with them, even when there was no difference in the actually amount of time spent (35). This is not to say that spending time at the bedside is not important. Indeed, the proper etiquette to promote good patient experience often requires an extra investment of time at the bedside, particularly during the first patient–physician encounter (36). Rather, our results support that the notion that quality time at the bedside is what is needed to provide the optimal patient experience.
Implications and Directions for Future Research
The results of this study highlight the need to explore new methods to promote patient-centered hospital care. Leveraging technology may be one mechanism to ensure that patients and their physicians understand each other’s goals and needs (37). For example, effectively designed electronic health records (EHRs) that summarize essential items of the patient’s diagnoses and treatment plan can keep patients up to date. Likewise, if EHRs were programmed to allow patients to input information about their goals, concerns, and questions, this might allow physicians to be better prepared to address them and to attend to psychosocial issues beyond the patient’s hospital stay. Future research should focus on how technology can overcome the gaps in patient–clinician care agreement that time-at-bedside alone cannot.
The discrepancy between patient experience and patient–clinician plan of care agreement during ward rounds may also have implications for hospital medicine groups looking to develop performance metrics. When patients do not understand or agree with issues such as discharge date, location, or transportation, this can lead to unnecessary delays in the discharge process and increase the risk of readmission (38 –40). Although much emphasis has been put on patients’ experience during transitions of care, the use of patient satisfaction as a performance metric has been met with some skepticism among clinicians. The agreement instrument used in this study is attractive because it provides a degree of objectivity that may allow physicians to anticipate and respond to disagreements with their patients. For example, if a hospitalist is provided with real-time data demonstrating that several of his or her patients do not agree with the anticipated date of discharge/discharge location, that physician can proactively address those issues to ensure smoother transitions of care. The validity, feasibility, and acceptability of such an instrument should be explored as hospitals look to find valid metrics for war-based care.
Limitations
This study has limitations. First, it was conducted at a single academic medical center, which limits the generalizability of our findings to other settings. Second, this was an observational study, which limits our ability to make inferences about causality. Third, we used direct observation by a research assistant, which may have influenced the clinician team’s amount of time at the bedside. However, we attempted to mitigate this effect by observing each team for several consecutive days, thus allowing the clinicians to become comfortable with observation. Fourth, because this was a pilot study, we were unable to conduct an a priori power calculation to ensure an adequate sample size. However, the narrow CIs for our parameter estimates indicate that a clinically meaningful association time-at-bedside and patient-centered outcomes is unlikely. Fifth, patients’ were surveyed regarding their experience while they were still hospitalized and, as such, they may have been reluctant to provide negative ratings of their care. Sixth, while we quantified the amount of time, we did not further measure the activities performed in each location during ward rounds. Seventh, we modified the instrument used to measure plan of care agreement from its original version (21), which may have negatively affected its validity in the context of this study.
Conclusions
This study found no significant association between time-at-beside during hospital ward rounds and patient experience or patient–clinician agreement. Patients and their clinicians often disagree about important aspects of the plan of care, which may have negative downstream consequences—future research should work to identify new interventions to improve patient–clinician communication during ward rounds.
Supplemental Material
Supplemental Material, sj-docx-1-jpx-10.1177_23743735211008303 - Relationships Between Time-at-Bedside During Hospital Ward Rounds, Clinician–Patient Agreement, and Patient Experience
Supplemental Material, sj-docx-1-jpx-10.1177_23743735211008303 for Relationships Between Time-at-Bedside During Hospital Ward Rounds, Clinician–Patient Agreement, and Patient Experience by John T Ratelle, Michelle Herberts, Donna Miller, Ashok Kumbamu, Donna Lawson, Eric Polley and Thomas J Beckman in Journal of Patient Experience
Supplemental Material
Supplemental Material, sj-tif-1-jpx-10.1177_23743735211008303 - Relationships Between Time-at-Bedside During Hospital Ward Rounds, Clinician–Patient Agreement, and Patient Experience
Supplemental Material, sj-tif-1-jpx-10.1177_23743735211008303 for Relationships Between Time-at-Bedside During Hospital Ward Rounds, Clinician–Patient Agreement, and Patient Experience by John T Ratelle, Michelle Herberts, Donna Miller, Ashok Kumbamu, Donna Lawson, Eric Polley and Thomas J Beckman in Journal of Patient Experience
Footnotes
Acknowledgment
The authors thank Marybeth Floersch for her assistance with consent, observation, and data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant number (UL1 TR002377) from the National Center for Advancing Translational Science. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.