
Abstract
Medical education values patient-centered communication skills of responding to patient's emotions, however, guidance is limited on how to provide a well-rounded curriculum. This study examines the effect of a 90-minute communication workshop on the level of empathy of the 116 medical students who participated in the workshop. We used three psychometric categories from the Jefferson Scale of Empathy (JSE) as dependent variables. We conducted mixed analysis of variance (ANOVA) analyses to determine the change in empathy scores after the workshop, the main effects for gender and medical specialty, and their interaction with time. We found an increase in perspective taking and compassionate care scales, although no changes on walking in patients’ shoes scale. Female and people-oriented specialty students scored higher on all scales. Some gender-specialty groups showed an empathy decrease: people-oriented specialty females on compassionate care scale and people-oriented and other specialty males on walking in patients’ shoes scale. We concluded that communication training requires a multidimensional approach to target various areas of building empathy. Standardization of training should be embedded with empathy development within medical education curriculum.
Keywords
Introduction
Clinical empathy research has shown that the ability for healthcare professionals to create interpersonal relationships with patients is beneficial (1–3). Consequently, medical education has shifted focus to a patient-centered approach that includes responding to patient's emotions, validating concerns, offering support, and developing a partnership for treatment planning (4–6). Developing empathy is key to recognizing patients’ emotions and has even become a goal of medical education recognized in licensures and medical education policies put in place by agencies such as the American Association of Medical Colleges (AAMC) (7,8). Yet, focus on empathy in medical education programs is still in the early stages and there is little guidance on how to teach, evaluate, convey, and even define empathy in medical contexts (9–11). In response to this need, the Jefferson Scale of Empathy (JSE) was developed and became a widely used instrument to evaluate empathy in medical contexts (12). The importance of teaching communication in the medical field derives from the need to enhance medical personnel's capacity to provide accurate information to patients in a manner that demonstrates care and concern for others and encourages the practical use of empathy within patient–clinician relationships (1,13–15).
Healthcare professionals must balance the communication of objective medical information while also maintaining empathy and readily responding to patient emotions (3,14,16,17). Physicians need effective skills of expressing empathy that shows understanding, respect, and support to empower patients to make informed decisions (18,19). Empathy creates emotional space to allow patients to evaluate their values and motivation for treatment (13,18,20). On the contrary, lacking empathetic communication skills decreases the patient satisfaction and can lead to burnout in physicians (15,17,21).
Patient-centered care should prepare health professionals to be empathetic and to effectively communicate empathy (10,21,22). Communication refers to a shared interpretation of meaning (23). Empathy, in this case clinical empathy, goes beyond a shared understanding and focuses on the actions of the health professional to interpret what a patient is feeling and validating through communication an understanding to the patient (12). Communication of healthcare information with explicit acknowledgment or consideration of the patients’ emotions is more effective in a clinical setting than that without expressions of empathy (9,14). Since empathy is a part of the interpersonal skills needed to understand and interact with patients, several studies recognize empathy skills should be strengthened throughout medical training (6,24).
A shared psychometric scale to measure empathy can help medical education be standardized with respect to developing recognition of emotion and expressing empathy. The present study aims to understand if a 90-min workshop given to medical students on how to recognize patient perspectives and utilize verbal expressions of empathy and exploration improves the medical students’ level of empathy as measured by the JSE. Research demonstrates an interaction of gender and medical specialty on clinical empathy (12). Hojat et al. discovered that students and physicians who identified as women scored higher on JSE (9). Additionally, students in procedure-oriented specialties are more likely to show a lower JSE score (9,12,24). To extend the scope of current research, we sought to examine the effect of a single workshop delivered to all learners on clinical empathy scores and any differences of that impact when considering gender and medical specialty.
Method
We conducted a workshop for pre-clerkship medical students to introduce and practice skills to acknowledge patients’ emotions, and articulate verbal empathy as part of a required clinical skills curriculum at the University of Texas Southwestern Medical Center (18,25). The students’ self-reported empathy was evaluated before and after the workshop on the JSE according to specific measurements. The study was considered exempt by the appropriate institutional review boards.
Communication Intervention Workshop
The 90-miute workshop was delivered to all pre-clerkship medical students by faculty mentors responsible for all clinical skills curriculum delivery. Each mentor is matched with a small group of 6–10 students which remains consistent throughout their training. Faculty received one hour of training on the curriculum content and delivery of the workshop. Learners were assigned asynchronous pre-reading to review the effects of communicating empathy (16). The workshop first introduced a case example of a patient presenting to discuss their laboratory results which requires a provider to “break bad news” of a new diabetes diagnosis. Faculty then reviewed a framework of various skills to express verbal empathy which includes naming emotion, understanding patient perspective, respecting patient experience, providing statements of support, and further exploring patient emotion (26). A brief scripted role-play was introduced, with faculty reading different patient responses to the news. The students were encouraged to recognize patient statements as emotional responses, and faculty then facilitated a repetitive drilled practice for students to deliver scripted phrases of verbal empathy in response to each patient statement.
The workshop concluded with a structured debrief of the experience. The repeated phrases used during the drills were developed using evidence-based methods of articulating empathy through validating and exploring patients’ feelings (18,25,27).
Research Sample
The sample consisted of 116 pre-clerkship medical school students who participated in the communication training workshop as part of their standard clinical skills development curriculum. They voluntarily completed the pre- and post-survey assessments and opted for data inclusion. The participants were asked to identify their gender, medical school specialty or area of interest, and year in medical school. Fifty-eight of the students identified as male and 58 as female. The students were given the option to select a gender based on their own determination. The specialties consisted of 23 primary selections with 18 sub-selections. Those selections were then categorized and broken into three areas previously established by research related to the JSE. The areas are Procedure-oriented, People-oriented, and Other. As described in the literature, the people-oriented specialties focus more on long-term care, such as general internal medicine, family medicine, pediatrics, and psychiatry (12). The Procedure-oriented specialties focus on diagnostic or technical procedures and usually do not require long-term care of patients; some examples are surgery, radiology, and pathology (12). The Other specialties do not fit into a specific category as it relates to patient–clinician relationships and can have traits of both procedure- and people-oriented specialties, such as dermatology and emergency medicine (9,12,24). The classification was established and supported by existing literature utilizing the JSE (9,12,24).
Table 1 describes the distribution of the sample by gender and specialty.
Descriptive Statistics of Distribution Sample.

Instrument: JSE
The JSE version created for medical students was used to assess participants’ levels of empathy pre- and postworkshop. The JSE is a psychometric instrument of 20 questions, based on a 7-point Likert scale. Higher scores indicate higher levels of empathy, and two items required reverse scoring statements. The JSE contains three categories of questions within the 20-question survey (12). The first category indicates the clinician's Perspective taking which is the ability to see patients with empathic concern and dutifulness (9,12). Second is Compassionate care, which involves being empathetically concerned, having faith in people, displaying tolerance as well as self-protection, all while maintaining clinical neutrality (12). Lastly is Walking in a patient's shoes and seeing how their environment, social, and physical attributes affect their lifestyle. All these components involve verbal and nonverbal communication from both the patient and medical professional which may be exerted at different levels.
Data Analysis
Composite scores were computed as the means of the corresponding JSE items for each of the three psychometric scales. The reliability of the three scales was calculated based on the pre-workshop results. Cronbach's alpha coefficients were .794 for the Perspective talking scale; .727 for the Compassion of care scale; and .737 for the Walking in a patient's shoes scale. The three psychometric scales are the dependent variables in the study while gender and medical specialty are factors. We then conducted a series of mixed analysis of variance (ANOVA) analyses to determine the change in empathy after the workshop (time as within-subjects factor), the main effects for gender and medical specialty (between-subjects factors), and their interaction with the workshop intervention described as time.
Results
Gender Effects
Mixed ANOVA analyses were conducted to assess the effect of gender on the three psychometric scales between pre- and postworkshop. Table 2 shows descriptive statistics comparing pre- and postworkshop mean scores by gender. Then we present the results of the ANOVA analyses for the three JSE scales.
Perspective Taking
There was no significant interaction between gender and time, F(1, 114) = .223, p = .638. There was, however, a significant main effect for time, F(1,114) = 20.585, p <.001, with both gender groups showing an increase in empathy scores after the workshop. The gender effect was not significant, F(1, 114) = 1.683, p = .197 although females scored higher than their male counterparts.
Compassion of Care
There was no significant interaction between gender and time, F(1,114) = .000, p = .995. There was no significant main effect for time, F(1, 114) = 3.226, p = .075, with both gender groups showing an increase in empathy scores after the workshop. The gender effect was significant, F(1, 114) = 6.585, p = .012, women scored higher than their male counterparts at both times.
Walking in a Patient's Shoes
There was no significant interaction between gender and time, F(1, 114) = 1.628, p = .205. There was no significant main effect for time F(1, 114) = .01, p = .895, with only the female gender group showing an increase in empathy scores after the workshop. The gender effect was significant, F(1, 114) = 4.296, p = .040, women scored higher than their male counterparts.
Medical Specialty Effects
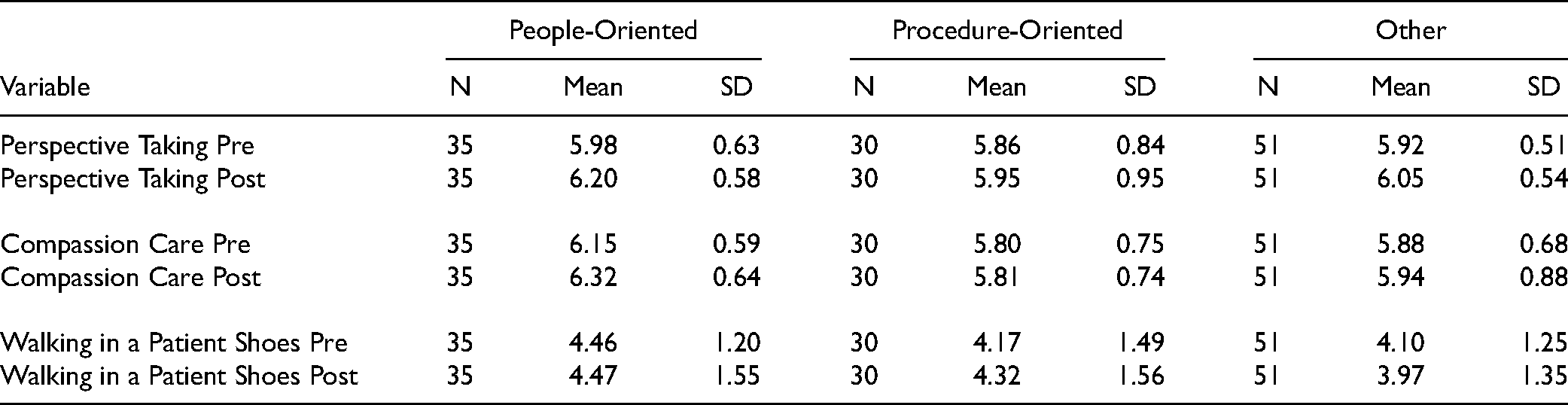
A similar analysis was conducted to assess the effect of medical specialty on empathy scales before and after the workshop. Table 3 shows descriptive statistics comparing pre- and postworkshop mean scores by medical specialty. Then we present the results of the ANOVA analyses for the three JSE scales.
Descriptive Statistics of Jefferson Scale of Empathy (JSE) Scales by Time and Gender.

Perspective Taking
There was no significant interaction between medical specialty and time, F (1, 113) = 1.361, p = .261. There was however a significant main effect for time, F (1,113) = 19.875, p <.001, with all specialty groups showing an increase in empathy scores after the workshop. The specialty effect was not significant, F (1, 113) = .672, p = .513 although people-oriented specialty scored the highest.
Compassion Care to Patients
There was no significant interaction between medical specialty and time, F (1, 113) = 1.009, p = .386. There was no significant main effect for time, F (1,113) = 3.049, p = .084, although all specialty groups showed a slight increase in empathy scores after the workshop. The specialty effect was not significant, F (1, 113) = .672, p = .513 although people-oriented specialty scored the highest.
Walking in Patient's Shoes
There was no significant interaction between medical specialty and time, F (1, 113) = .662, p = .518. There was no significant main effect for time, F (1,113) = .015, p = .903, with all specialty groups showing an increase in empathy scores after the workshop except for the category of other, which scored lower. The medical specialty effect was not significant, F (1, 113) = 1.175, p = .312 although people-oriented specialty scored the highest.
Gender and Medical Specialty Effects
In this section, we will examine the changes in empathy scores over time at the intersection between gender and medical specialty. Similar mixed ANOVA analyses were conducted to assess the effect of gender-specialty groups on the three psychometric scales between pre- and postworkshop time. The six gender-specialty groups correspond to male people-oriented, male procedure-oriented, male other, female people-oriented, female procedure-oriented and female other. Table 4 shows descriptive statistics comparing pre- and postworkshop mean scores by gender-specialty groups. Then we present the results of ANOVA analyses for the three JSE scales.
Descriptive Statistics of Jefferson Scale of Empathy (JSE) Scales by Time and Specialty.
Descriptive Statistics of Jefferson Scale of Empathy (JSE) Scales by Time and Gender-Specialty Groups.

Perspective Taking
There was no significant interaction between gender-specialty groups and time, F (1, 110) = .604, p = .697. There was however a significant main effect for time, F (1,110) = 16.891, p <.001, with all six gender-specialty groups showing an increase in empathy scores after the workshop. The gender-specialty effect was not significant, F (1, 110) = 1.316, p = .263. Interestingly, in people-oriented specialties males are scoring slightly higher than females while in procedure-oriented specialties, females are scoring higher than males.
Compassion of Care
There was no significant interaction between gender-specialty groups and time, F (1, 110) = .600, p = .700. There was no significant main effect for time, F (1,110) = 1.815, p = .181, with all six gender-specialty groups showing an increase in empathy scores after the workshop except for females in procedure-oriented specialty. The gender-specialty effect was not significant, F (1, 110) = 2.451, p = .038, but females are scoring higher than males in each specialty category.
Walking in Patient Shoes
There was no significant interaction between gender-specialty groups and time, F (1, 110) = .826, p = .534. There was no significant main effect for time, F (1,110) = 0.004, p = .950, with all gender-specialty groups showing an increase in empathy scores after the workshop except for males in people-oriented and other specialties. The gender-specialty groups effect was not significant, F (1, 110) = 1.384, p = .236, but females are scoring higher than males in each specialty category.
Figure 1 shows a visual representation of the mean scores over time for each JSE scale by gender-specialty groups.

Change over time of Jefferson Scale of Empathy (JSE) mean scores by gender-specialty groups.
Discussion
The majority of JSE literature discusses specialty and gender independently as they relate to empathy. This study uniquely included interaction effects of specialty and gender subgroups within each empathy category of the JSE. The baseline data confirms most of the gender and medical specialty effects previously found in studies using the JSE instrument (9,12). In addition, we have uniquely identified that women in procedure-oriented specialty were the highest scoring subgroup in Perspective taking and Walking in patient's shoes at baseline. A unique finding in this study was the relative low score of all students, regardless of gender and specialty, in the category of Walking in a patient's shoes. Conversely, the mean scores for Perspective taking and Compassion of care were significantly higher across all specialties regardless of gender. Overall, all gender-specialty groups improved in Walking in patient shoes except males in people-oriented and other specialties which actually showed a decrease in empathy after the workshop.
The findings suggest that curriculum development may need to be adapted to target learner's specialty of interest, highlighted by differences in workshop impact on people-oriented and other-oriented specialties and less notable impact on procedure-oriented specialties. This may reflect different learning styles, particularly given no significant difference in those groups at baseline.
Limitations
While a well-established validated instrument, the JSE relies on self-reporting that may influence participants to provide a more positive response in the posttest (9,12,28). Additionally, the workshop is based on scenarios from clinical environments with which students may not have had adequate experience, and thus could affect scoring. Even with these limitations, the workshop shows promising benefits in raising medical students’ empathy awareness.
Implications
This study uses small interventions and gauges the empathy levels of medical students that allow for implementing change. This is an important step since other national studies found that a decline in empathy occurs for both students and residents as they go through schooling (3,9,24,28). This study contributes to research suggesting that clinical empathy should be embedded in the curriculum through diverse workshops that can be adjusted to the specific needs of the students. More research is needed to understand how empathy affects performance, trust, and self-efficacy within healthcare teams as medical students move into residency.
Conclusion
Healthcare professionals are expected to demonstrate empathetic concern, perspective taking, compassion, and understanding of patients. Research shows that higher levels of clinician empathy and patient–clinician communication skill training can improve patient satisfaction and reduce physician burnout (10,16,22). Communication training requires a multidimensional approach to target the various areas of building empathy; and as highlighted by this study, the impact of a curriculum can vary based on the participant’s demographic and medical specialty. Further research is needed to identify and optimize curricula for all medical students, regardless of gender and specialty. In addition, understanding deficits in domains of empathy allows communication training experts to focus on a specific curriculum, and openly discuss and assess the issue throughout healthcare professionals’ education and career (29,30). Our study notes the lowest scores in Walking in a patient's shoes. Research shows courses in arts and humanities could have a greater impact on that domain (3,15,28). Creating a cohesive, multifaceted, and standardized communication training in medical education will have shared benefits for medical students, physicians, and patients.
Footnotes
Acknowledgments
We would like to express my very great appreciation for the support of research assistant Rithwik Terala in this project through data transcription and database development. We would also like to thank Grant Moore, LCSW for agreeing to review the manuscript and offer suggestions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval to report this case was waived from the institutional review board. This was due to using deidentified data. Our institution does not require ethical approval for reporting individual cases or case series.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
There are no human subjects in this article and informed consent is not applicable.