
Abstract
Patient–physician communication is a critical component of care in the emergency department (ED) and can be challenging within the fast-paced ED environment. Hospitals often use surveys on patient experience to evaluate physician communication skills and determine a need for improvement. As simulation has proven effective in improving physician communication skills, we developed a simulation workshop specifically for emergency physicians. Our design used simulated patient experiences, a group debrief, and scenarios that included critical communication elements that correlate with patient experience. The physicians were surveyed before and after the course. The simulated patients completed evaluation checklists and patient experience surveys for each of the physician participants. Patient experience ratings increased from 76% to 90% between the predebrief and postdebrief scenarios and 100% of participants would recommend this course to a colleague. A moderate correlation was observed between the prior year average of clinical patient experience scores for each physician and the initial simulated participant experience ratings (r(6) = .52, P = .18). This workshop is a feasible and well-received method to utilize simulated patients to provide critical feedback and improve patient experience.
Introduction
Patient–physician communication is a critical component of emergency department (ED) care. In a fast-paced, high-stress environment, building rapport with patients can be challenging for physicians. Poor communication skills can negatively impact patients’ experiences and overall experience of care. 1 A positive patient experience increases the likelihood of adherence to treatment plans and future use of healthcare services. 2 Patients are often surveyed about physicians’ ability to communicate, including whether they feel heard, understood, and involved in their own care. 1 Many institutions use tools like the Press Ganey survey to track patient feedback and identify areas for improvement.1–4
Despite evidence showing improved clinical outcomes for patients with a positive healthcare experience, many institutions do not have formal programs to ensure that their physicians maintain strong communication skills.5–6 Communication skills training has been shown to have a positive return on investment. Boissy et al demonstrated that an 8-h lecture-based communication skills training for attending physicians improved patient experience ratings and self-reported empathy, as well as reduced burnout. 6
A significantly more experience-based learning modality, simulation offers an opportunity for training in communication. Simulation exercises with simulated participants (SPs) have proven effective in educating medical professionals in training. 7 High-fidelity simulation-based medical education (SBME) is currently used for continuing education of clinical technical skills, and simulation-based education has been similarly recommended for use in training nontechnical skills. 8 Simulation training for learning communication and empathy has been successfully implemented for medical students. 9 Many residency programs have also implemented SBME of nontechnical skills and preparation for service failures in their curriculum.2,10,11 As with technical skills, empathy and communication require continuing practice throughout a physician's career to ensure expertise.
The authors developed a novel SP simulation program designed to provide feedback to attending physicians on nontechnical skills, with a particular focus on patient’ experience. The objectives of this pilot program were to test feasibility and acceptability of this curriculum type for practicing physicians and to evaluate the impact of such a curriculum on perception of physicians’ care.
Methods
Emergency medicine (EM) attending physicians were recruited to participate in a 120-min SP simulation pilot course. Demographic data regarding the participants were elicited using a presurvey. Baseline patient experience scores were obtained and anonymized, using the past 12 months of physician-specific questions on PG surveys. Participants also responded to a Toronto Empathy Questionnaire. 12 The session consisted of a prebrief, an individual patient scenario with common elements of the patient experience, a group debriefing, and then a second individual patient scenario followed by 1:1 SP feedback with the physician. These events were facilitated by simulation expert educators, including EM physicians and SP Educators. Participating physicians were asked to assume their typical clinical role in the scenario.
The flow of the workshop is indicated in Figure 1. Eight SPs were recruited for the simulation activity over 2 days. Simulated participants are part of the institution's simulation center SP Program and were trained by one of the program's SP Educators. None of the SPs were previously known to the physicians. Each SP was trained in 1 of 2 scenarios, involving presentations and behaviors related to emotions and corresponding dialogue. Scenarios followed a typical ED encounter: physicians initially conducted patient interviews, performed a physical examination, shared a clinical impression and plan, and departed from the room. A set of results of an appropriate diagnostic plan was then provided to the physicians, who then returned to the patient's room for a reassessment and discharge planning discussion. Case details are described in Figure 1; full case details are available from the authors upon request.

Flow of communication workshop.
All SPs completed standardized group training to maintain consistency in emotional portrayal and ensure accurate roleplay. Additionally, SPs were trained to provide verbal feedback on communication skills immediately after the scenario ended. Simulated participants also completed an evaluation tool on communication skills and responded to the physician-specific subset of questions mirroring the PG patient evaluations. Simulated participants evaluated between 1 and 4 physicians between the 2 days and were blinded to whether the case was the first or second experience for each physician due to scheduling.
The group debriefing between scenarios was moderated by an expert simulation educator (SMH) with extensive experience facilitating the debriefing of communication scenarios. The session focused on achieving the workshop's educational goals by reviewing relevant patient experience literature in the context of physicians’ real-world experiences.13–15 Using a standard format, the debriefing gathered initial reactions, shared observations, and reviewed key patient experience findings. Topics covered included expressing empathy during difficult discussions, validating patient perspectives, and addressing patient comfort through nonmedical gestures. No data were collected during the debriefing. Individual SP ratings were shared with each physician during the feedback portion of the course.
Descriptive statistics were used to evaluate scores. Pre- and postdebrief scores were compared using a paired t test. The Shapiro-Wilks test demonstrated a normal distribution of the data. The baseline PG scores were compared to the predebrief PG score using a Pearson correlation. This study was reviewed and determined to be exempt by the institutional review board at Rush University Medical Center.
Results
As outlined in Table 1, 9 physicians out of 45 eligible emergency physicians enrolled in an optional communication workshop. Preworkshop surveys revealed 89% found simulation for communication skills “extremely useful.” The baseline average TEQ score was 55.4 (±5.5), higher than the general population's average of 43.5 to 48.9. 12 Simulated participant patient experience rating improved from 75.7% predebrief to 89.6% postdebrief (13.9%, P = .03). Press Ganey scores from 12 months prior to the course averaged 81.7% after excluding one physician with less than 12 months of data, a moderate, but not statistically significant correlation with predebrief SP ratings was found (r(6) = .52, P = .18). Evaluations indicated that 100% of participants would recommend the workshop to a colleague and found the group debriefing helpful.
Attending TIPS Course Data Summary Table Totals.
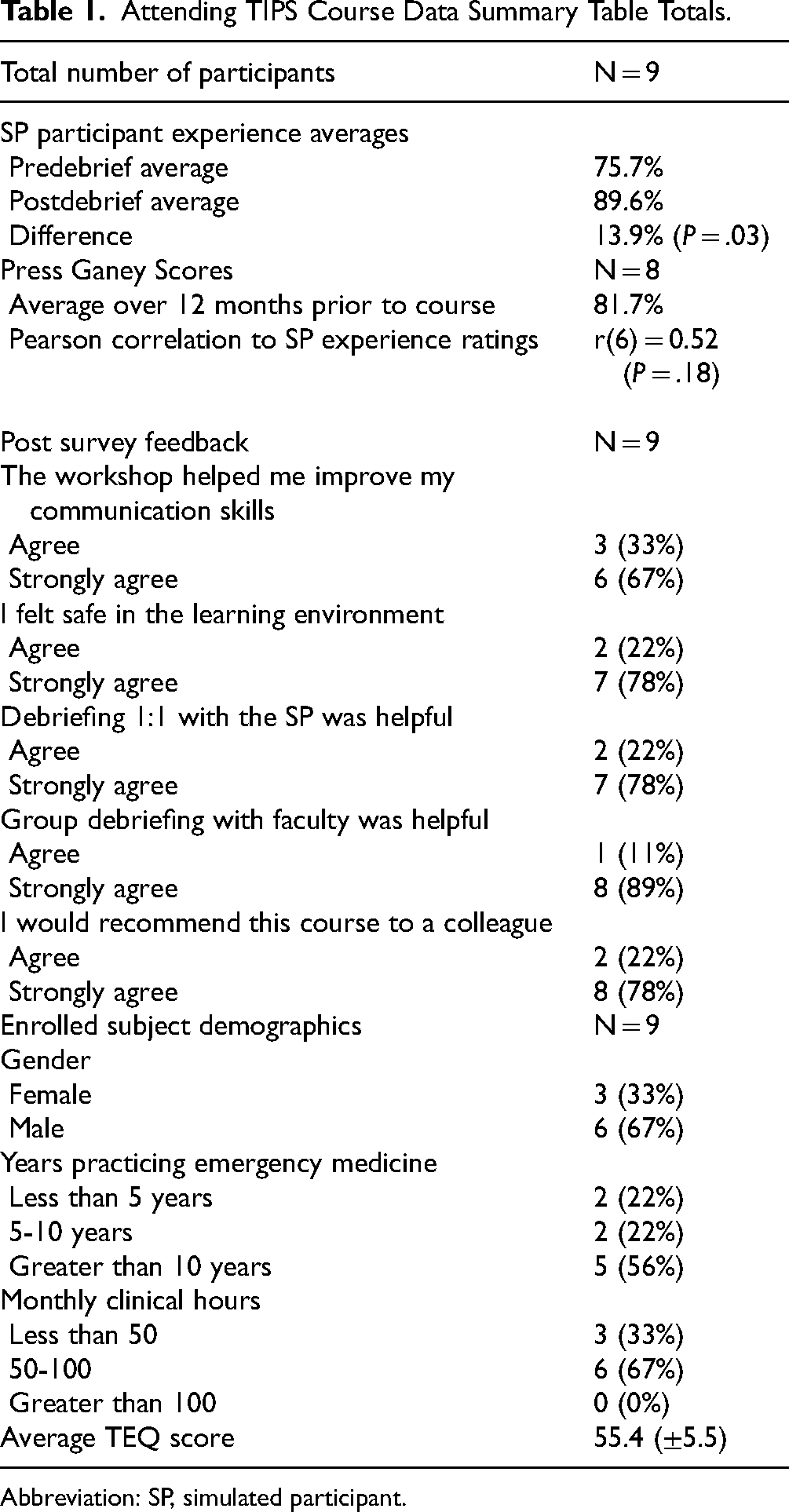
Abbreviation: SP, simulated participant.
Participant qualitative feedback was gathered using free text entry. Representative comments include: “This was a good opportunity to self-reflect on patient encounters. Simulated participants are helpful in providing feedback to improve self-understanding,” “Importance of pausing for patients to process information,” and “To be more intentional with positioning in the room in tune to patient body mechanics and to consider at least 1 nonmedical gesture during patient encounter.” These comments demonstrate that participants reflected on their performance and were given actionable feedback.
Discussion
The course was highly rated by all participating physicians, who felt the course was useful and commented that the SPs were a valuable addition. The physicians valued the group debrief session and 1:1 individualized feedback from the SPs. Course feedback centered around developing scenarios that allowed for a sufficiently challenging emotional response from the SPs. A challenge we encountered was striking a balance between an appropriately challenging patient without changing the focus of the course towards patient de-escalation techniques.
A moderate correlation between ED patient experience scores and SP scores suggests that the SP experience may be similar to an actual ED patient experience. While not statistically significant, this implies that the course could potentially be used to identify physicians who struggle with providing a positive patient experience or to remediate physicians struggling with patient experience. The lack of significance could stem from provider variability and the small sample size, warranting further research with a larger cohort. The increase in patient experience scores from predebrief to postdebrief shows the course achieves its goal of encouraging reflection and improvement in communication and empathy skills.
Limitations
Our small sample size limits generalizability and statistical significance. Time commitment for the workshop led to recruitment challenges. Additionally, preworkshop ratings and self-selection may have led to a skewed sample, reducing representativeness. Broader recruitment strategies would reduce bias in future studies. The ED Press Ganey data may not solely reflect the physician's individual performance, as scores could be influenced by other members of the healthcare team and the overall patient experience in the ED. PG scores have not been validated in a simulation setting. The workshop format prevented SPs from assessing the PG question on “Doctor's concern to keep you informed about your treatment,” omitting this element from SP ratings. Variability and reliability in SP ratings were addressed through standardized training performed by SP educators. Simulated participants are trained to complete evaluation tools accurately and consistently, however, subjective items may allow for inter-rater variation and may pose a limitation in the extent of the conclusions drawn from this study.
Conclusion
A SP scenario-based workshop format is a feasible and valued way to provide feedback to physicians on patient experience. The overall experience ratings of the SPs improved from the first scenario to the second scenario following feedback and debriefing, indicating that this format of personalized feedback may result in recognition of opportunity for growth. This could ultimately lead to positive behavior change, improving patient experience over a physician's career.
Footnotes
Authors’ Note
Ethical Approval: This study was reviewed and determined to be exempt by the Institutional Review Board of Rush University medical center (24032607-IRB01). Statement of Human and Animal Rights: All procedures in this study were conducted in accordance with the Rush University Institutional Review Board (24032607-IRB01) approved protocols. Statement of Informed Consent: Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Author Contributions
SS, SH, and GCC designed and developed the project. SS and SH performed the measurements and analyzed the data. SS, SH, and MY developed the content for use in the project. GCC collected data and aided in interpreting results. SS, SH, and GCC wrote the manuscript in consultation with MY.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.