
Abstract
Increasing prevalence of type 2 diabetes mellitus (DM) poses ongoing challenges to current health care systems. DM prevalence is higher in veteran patients as compared to general population. 1 Teleconsultation, an alternative to in-person specialty care, is particularly suited to patients who cannot travel extended distances for specialty care. 2 The Veterans Health Affairs system has pioneered and supported many virtual health interventions,3,4 including DM electronic consultation services, which we initiated in our institution in 2012. As part of the internal qualitative analysis, we assessed if electronic-consultation for DM management is as effective as standard, in-person endocrinology care. A retrospective chart review was performed of 281 patients at the Michael E. DeBakey VA Medical Center (MEDVAMC) upon approval from the Baylor College of Medicine Institutional Review Board. Inclusion criteria included diagnosis of DM and hemoglobin A1C (HbA1C) 8% or higher. Patients were excluded from the analysis if they were actively managed by another endocrinologist, on insulin pump therapy, or pregnant. Primary end point of change in HbA1C after 6 months of care was evaluated within each group and between groups. Data collected included type of consult (in-person or e-consult), demographic characteristics, duration of DM, use of oral DM medications, insulin doses, laboratory parameters, date of consult request, and completion and implementation of e-consultation recommendations. All items were collected at baseline and 6 months. All analyses were performed based on initial consultation type, with last observation carried forward for missing data. We used statistical software package Stata/IC: Release 10 (StataCorp LP, College Station, TX). Student’s t-test was used for normally distributed variables and Wilcoxon rank-sum test for non-normally distributed variables. No significant differences in demographic characteristics, anthropometric data, laboratory parameters, or comorbidities were noted. Patients in the e-consult arm lived significantly farther from the MEDVAMC than in-person group (81.8 and 47.7 miles, respectively; P = .002). Baseline mean HbA1C was greater than 10% in both groups. Electronic-consultation was equally effective in reducing 6-month HbA1C as in-person diabetes clinic (−1.05 ± 1.7% e-consultation vs −0.99 ± 1.9% diabetes clinic; P = .77). The HbA1C reduction in patients with implemented e-consults (−1.21%, n = 174) was significantly greater than the nonimplemented group (−0.79%, n = 107; P = .04) (see Table 1). Time to consult completion was approximately 4.7 days for e-consult and 77 days for in-person consultation. The reason for this difference is attributed to intrinsic differences in consult completion. Electronic consults are completed within 7 days, do not require scheduling, and are resolved by the specialist directly. In contrast, in-person consultation requires administrative assistance to schedule and consult completion depends on clinic access. In conclusion, diabetes electronic consultation at the MEDVAMC can achieve similar clinical outcomes to in-person specialty care. The benefits of electronic consultation service include comparable glycemic outcomes, the option of telephone-based education versus in-person diabetes education, recurring electronic consultation guidance as needed, and reduced hospital cost utilization. Although there is no surrogate for in-person specialty care and counseling, electronic consultation care should be considered for patients needing specialty care, but whose physical or financial limitations prevent in-person specialty assistance.
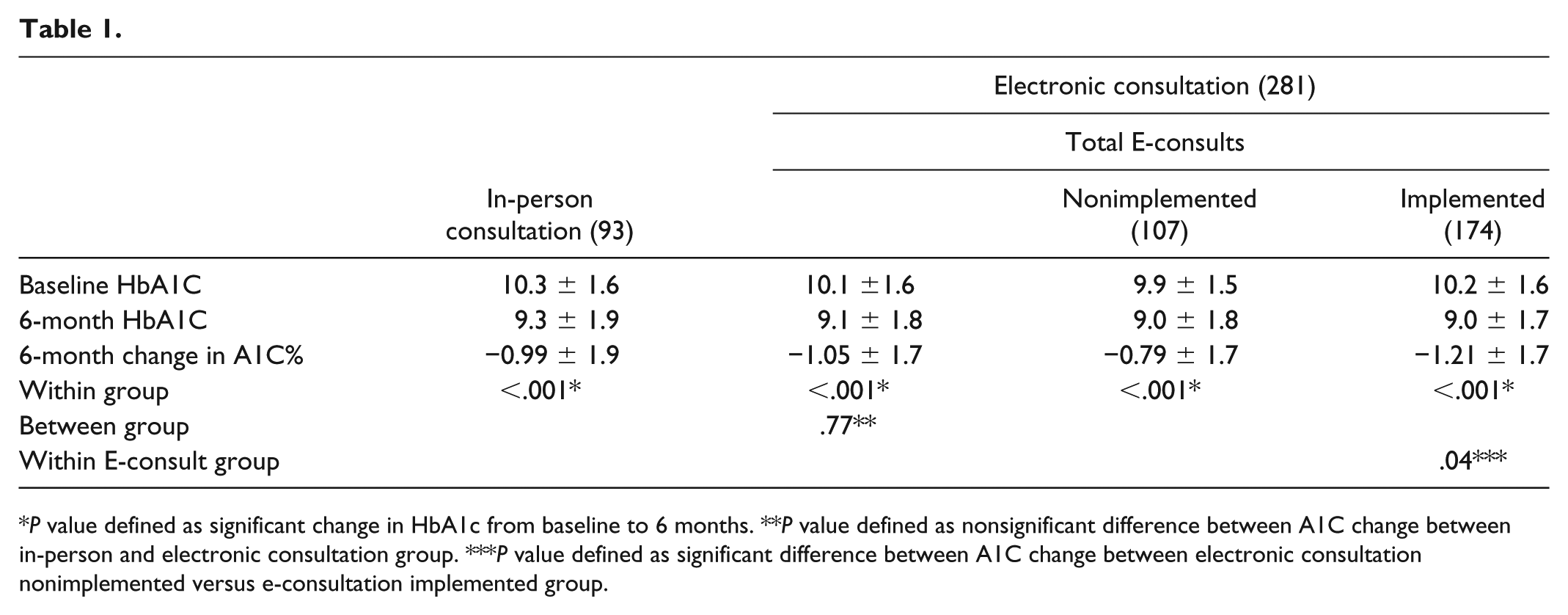
P value defined as significant change in HbA1c from baseline to 6 months. **P value defined as nonsignificant difference between A1C change between in-person and electronic consultation group. ***P value defined as significant difference between A1C change between electronic consultation nonimplemented versus e-consultation implemented group.
Footnotes
Acknowledgements
The data for this study are stored on a computer issued by the Veterans Health Affairs at the Michael E. DeBakey VA Medical Center in Houston, Texas. All patient information has been stored without patient identifiers and under encryption. Any and all data can be released to the reviewer and can be mailed electronically at their request.
Abbreviations
DM, diabetes mellitus; HbA1C, hemoglobin A1C; MEDVAMC, Michael E. DeBakey VA Medical Center.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.