
Abstract
Background:
Malignant pleural mesothelioma is a rare but complicated disease associated with very poor prognosis, despite all forms of treatment and almost 100% mortality after diagnosis.
Objectives:
The use of extrapleural pneumonectomy (EPP) in the management of malignant mesothelioma has become controversial recently and appears to be a dying modality. This retrospective study aimed to review and compare our results with available literature.
Methods:
Consecutive patients were reviewed from March 1999 to April 2011 who underwent EPP for malignant mesothelioma. Short- and long-term outcomes were analyzed retrospectively until February 2013.
Results:
There were 30 consecutive patients who underwent EPP in 13 years. The majority of them were male (29 patients) with a mean age of 61 years (34-71 years). There was no in-hospital or 30-day mortality in this cohort, although Thoracoscore predicted 7.9% risk of in-hospital mortality. The overall median survival was 20 ± 24 months, which prolonged to 47.5 ± 24 months in patients who received trimodality treatment. Thirty-one percent of patients survived ≥4 years and 2 patients are still alive at 6 and 7 years postoperatively. Survival was significantly longer in epitheloid versus biphasic mesothelioma, right versus left pneumonectomy, age below 65 years, and with no N2 disease. Survival at 6, 12, and 18 months was 80%, 65%, and 55% in comparison with 65%, 52%, and 34%, respectively, in the Mesothelioma and Radical Surgery trial.
Conclusions:
Epitheloid mesothelioma, right pneumonectomy, negative extrapleural lymph nodes, and age below 65 years are associated with prolonged survival. Extrapleural pneumonectomy has a role in the management of malignant mesothelioma in selected patients by experienced surgeons.
Introduction
Malignant mesothelioma is a rare but complicated disease associated with very poor prognosis, despite all forms of treatment and almost 100% mortality after diagnosis. It is a major health issue worldwide and Great Britain possesses the highest incidence of mesothelioma in the world, with more than 2000 deaths in 2006. 1 The treatment option has been controversial between surgical and nonsurgical management. The aim of extrapleural pneumonectomy (EPP) or extended pleurectomy decortication (EPD) is to reduce macroscopic tumor burden so that adjuvant therapies are then used to complete the cytoreductive process by eliminating micrometastatic disease. 2 High operative mortality has been reported of up to 9%, 3 but recent studies have reported significantly reduced operative mortality of 3.4%. 4 Variable median long-term survival has been reported. 5 –9
Tom Treasure’s group designed a multicenter randomized control trial (RCT) in 2005 to assess patients’ acceptability and potential recruitment rate for a larger trial to compare trimodal therapy (chemotherapy + EPP + hemithorax radiotherapy) with chemotherapy alone. The Mesothelioma and Radical Surgery (MARS) trial was initiated to test the feasibility of randomizing patients in the knowledge that the study was not powered to prove effectiveness of EPP over other management. 1 The MARS trial concluded the result that, in view of the high morbidity associated with EPP in this trial and in other nonrandomized studies, a larger study is not feasible. These data, although limited, suggest that radical surgery in the form of EPP within trimodal therapy offers no benefit and possibly harms patients. 10
Our institute has provided surgical treatment in the form of EPP for malignant mesothelioma for over 20 years. According to the guidelines of General Medical Council, United Kingdom, we have to reevaluate our practice against best medical evidence to maintain good medical practice. The MARS trial was the first best available evidence. Therefore, we decided to review our experience of EPP performed in the last 10 years and analyze the mortality and long-term survival in the reflection of the MARS result.
Methods and Material
Patients
We retrospectively analyzed the data of 30 consecutive patients with diffuse malignant pleural mesothelioma (MPM) from the departmental database and hospital records of those who were treated with EPP from March 1999 to April 2011 at Castle Hill Hospital, Hull, United Kingdom. Patients had been referred from peripheral hospitals, and we were unable to collect all the information regarding recurrences and complications, in particular for those patients comprising the early half of study.
Preoperative staging was based upon both clinical and radiological findings. In the initial period, computed tomography scan was used primarily, however recently positron emission tomography (PET) scanning has been used for disease assessment. The tumour, node and metastasis (TNM) staging has been based on the information thus obtained. All patients underwent video assisted thoracic surgery (VATS) diagnostic procedure, and MPM was confirmed histologically on pleural biopsies. Preoperative staging did not reveal N2 or stage III disease. Epitheloid histology was the most common subtype MPM in those patients chosen for EPP, while patients with sarcomata MPM were not offered EPP. All these patients were assessed for their fitness for surgery as per the protocol. Postoperative risk of in-hospital mortality was measured retrospectively by using Thoracoscore as a validated model of predicting postoperative risk and mean predicted risk was 7.9% ± 2.5% mortality.
Statistical Analysis
Survival data were collected from hospital records and their general physicians. Survival was observed until February 2013 and measured from date of surgery to the date of last contact or death due to any cause. Statistical analysis of survival was undertaken by use of a landmark of 30-day mortality after surgical resection. Univariate analysis was performed by means of the Kaplan-Meier life-table method to determine the effects of demographic and pathologic variables. The log rank test was used to determine statistical significance of comparisons among survival curves. Results with a P value of less than .05 were considered significant.
Results
All treatment modalities, including EPP, were carried out with a curative intent. Two surgeons performed procedures involving EPP, pericardiectomy, diaphragmatic resection and reconstruction with synthetic graft, and mediastinal lymph node excision. During the early period of study, patients received postoperative platinum-based chemotherapy only and those who were not fit received limited radiotherapy to wound. Later in the study, almost all patients were treated with postoperative adjuvant therapy that was the combination of systemic platinum-based chemotherapy and hemithoracic radiotherapy. However, no patient received any neoadjuvant therapy, intrapleural chemotherapy, or external beam radiation therapy.
Thirty patients had undergone EPP at Castle Hill Hospital from March 1999 to April 2011 (Table 1). Patients were predominantly male (29 patients) with a mean age of 61 ± 9 years (range 34-71 years). Eleven (37%) patients were aged 65 years or older. Median follow-up interval was 20 months (range 1.8-84 months). There was no in-hospital or 30-day mortality in our study group. Median hospital stay was 12 days. All patients were discharged home. However, 4 patients died within 60 days after surgery, 2 of them were older than 70 years of age and none of them received trimodality therapy.
Patients’ characteristics.

Abbreviations: postop, postoperative; preop, preoperative.
Survival analysis revealed overall mean survival of 28 ± 24 months (median 20 months, range 2 months to 7 years; Figure 1). Long-term survival analysis showed 35% of 3-year survival and 31% of 4-year survival. In all, 2 patients lived more than 7 years, and 2 patients are still alive after 6 and 7 years. In this study group, only 50% of patients (15 patients) received trimodality therapy. The patients who completed trimodality treatment showed significantly improved median survival of 47.5 months compared to 9 months in nontrimodality group (P value = .004, hazard ratio 0.3, 95% confidence interval [95% CI] 0.1-0.6; Figure 2). The 3- and 5-year survival in the trimodality group was 50% and 30%, respectively. In comparison, 3-year survival in nontrimodality was only 20% and no one lived for 5 years in this group. Postoperative histology showed that 80% of patients (24 patients) with MPM consisted of epitheloid cell type while 20% (6 patients) had biphasic cell type. Survival benefit was significantly evident in epitheloid versus biphasic mesothelioma (median survival 27 vs 8 months, P value .001) with a hazard ratio of 0.07 (95%CI 0.01-0.3; Figure 3A). The 3-year survival in epitheloid mesothelioma was 44%, while no patients survived 18 months in the biphasic mesothelioma group. Although no invasive disease (N2/stage III) was detected on preoperative staging, postoperative histology identified N2 disease in 30% of patients. Similarly, 83% of patients were identified with stage III disease postoperatively. N2 disease significantly reduced short-term survival. Median survival in patients with N2 disease was only 7 months compared to 25 months in patients without N2 disease (Figure 3B). Younger patients benefited more with EPP than older patients. In this study, patients below 65 years revealed median survival of 27 months compared to 12 months in patients with age of 65 years or older (hazard ratio 0.9, 95% CI 0.3-2.5, P value = .8; Figure 4A). The 3-year survival in younger patients was 41% while only 24% in elder patients. Two patients were older than 70 years and their median survival was only 1.97 months. In all, 19 (63%) patients were operated for MPM of the right chest and 11 (37%) patients had disease in left chest. Patients who underwent right pneumonectomy demonstrated better survival than left pneumonectomy (median survival 27 vs 10 months; Figure 4B). The 3-year survival was 42% in patients who underwent right EPP while 24% in patients who underwent left EPP. There was no recurrence in 13 (43%) patients but 9 (30%) patients presented with recurrences, that is, 5 with local recurrence, 1 in contralateral chest, and 3 in abdomen. However, we don’t have any information about 8 (27%) patients.

Overall survival with 95% confidence interval. Cohort = 30 patients.

Comparison of survival in trimodality versus nontrimodality treatment. Trimodality group = 16 patients and nontrimodality group = 14 patients.
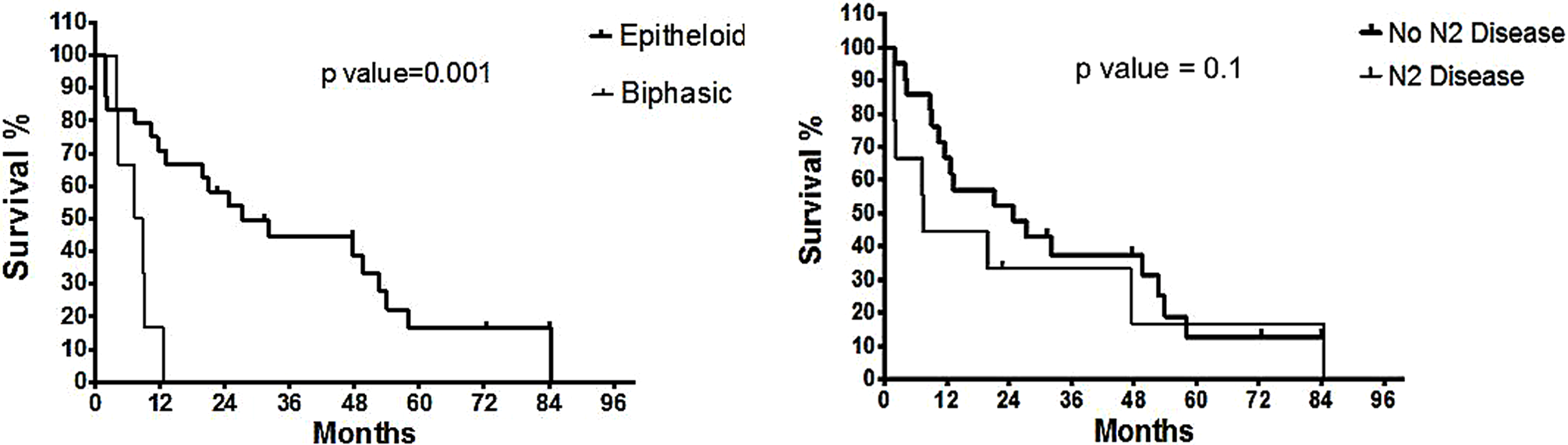
A, Comparison of survival in epitheloid versus biphasic malignant pleural mesothelioma (MPM). Epitheloid group = 24 patients and biphasic group = 6 patients. B, Comparison of survival in no N2 versus N2 disease. N2 disease group = 21 patients and no N2 disease group = 9 patients.

A, Comparison of survival in patients <65 versus ≥65 years. <65 years group = 19 patients and ≥65 years group = 11 patients. B, Comparison of survival in right versus left EPP. Right EPP = 19 patients and left EPP = 11 patients. EPP indicates extrapleural pneumonectomy.
We compared our study against the surgical arm of the MARS trial to evaluate whether or not our results were acceptable. Patients in our study group and the EPP arm of the MARS trial were very similar in patient characteristics such as gender, age, World Health Organization performance status, preoperative histology, preoperative nodal status, and staging (Table 2). In our cohort, all patients underwent a successful procedure while only 17 (71%) patients were offered surgery in MARS. There was no perioperative mortality in study cohort compared to 18% in the operated group of MARS. The MARS reported the survival only up to 18 months after surgery. 10 Overall median survival was 14.4 (5.3-18.7) months in MARS and 20 (1.8-84) months in our cohort. Survival at 6, 12, and 18 months was reported 65%, 52%, and 37% in MARS and 80%, 65%, and 55% in our study cohort, respectively. Overall, 3-year survival in our study cohort was 35%.
Comparison of this cohort with MARS trial.
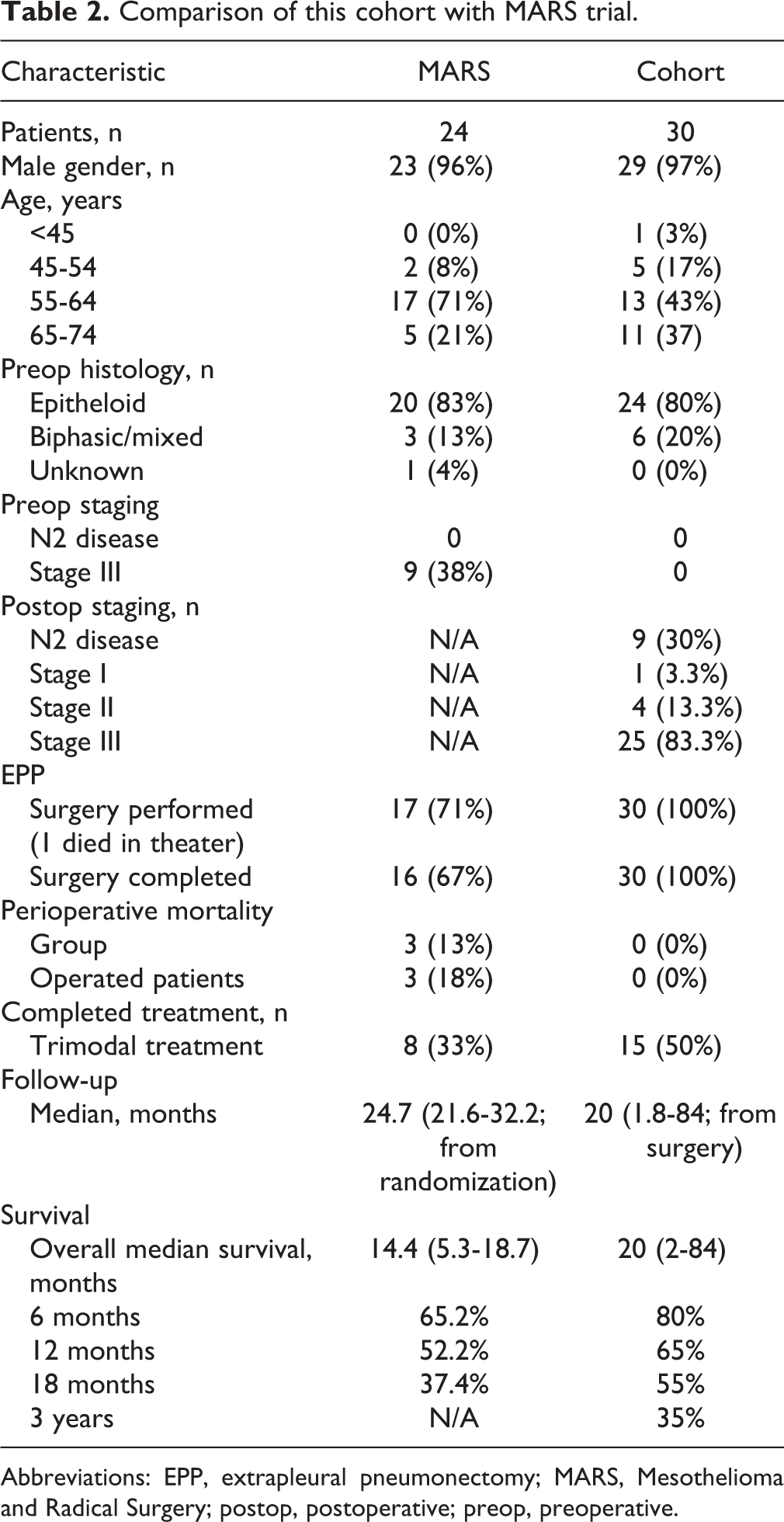
Abbreviations: EPP, extrapleural pneumonectomy; MARS, Mesothelioma and Radical Surgery; postop, postoperative; preop, preoperative.
Discussion
Treatment of MPM has been evolving progressively including surgical and nonsurgical management. Current surgical treatment aims to achieve macroscopic complete resection (MCR) either by EPP or EPD, followed by adjuvant chemoradiation therapy. 2 Operative mortality of EPP has reduced significantly from 31% reported by Butchart et al 11 in 1976 to 4.3% reported by Buduhan et al 12 in 2009 and 3.4% reported by Sugarbaker et al in 2011. 9 Variable median survival has been reported after EPP with trimodality therapy, demonstrating better median survival than surgery alone. 13 –16 Cao et al, in his recent systemic review of trimodality therapy for patients with MPM, reported median overall survival ranged from 12.8 to 46.9 months while perioperative mortality ranged from 0% to 12.5%. 17 Rusch et al in her recent analysis of a worldwide registry sponsored by the International Association for the Study of Lung Cancer (IASLC) demonstrated an 18-month overall median survival and 40 months for stage I epitheloid histology in patients who underwent EPP. 18
Our study included a cohort of 30 patients who underwent EPP over 12 years but only half of the patients managed to receive adjuvant therapy as a part of trimodality treatment. There was no operative mortality (0%) in our study group and overall median survival of 20 ± 24 months was observed. We have shown similar overall survival of 47% at 2 years and 13% at 5 years to those reported by Sugarbaker and associates in 1999. 6 Our 2- and 5-year survival in epitheloid MPM was 58% and 17% while in negative N2 disease was 47% and 12%, respectively, whereas 3-year survival was significant in epitheloid MPM (44%), negative extrapleural nodes (37%), younger patients (41%), and right EPP (42%). Valerie Rusch reported a 19-month median survival among 1359 patients with all stages of epithelial MPM who underwent surgical resection either by EPP or pleurectomy/decortication (P/D) in IASLC registry. Stage I tumors resected by EPP were associated with a median survival of 40 months, whereas those managed by P/D had a median survival of 23 months 18 while Flores et al reported similar outcome after EPP or P/D but a higher recurrence in P/D patients. 19
Despite all the evidence in favor of EPP, the MARS trial designed only to test feasibility of trimodality therapy concluded not only that a larger study is not feasible, but also that “radical surgery in the form of EPP with trimodal therapy offers no benefit and possibly harms patients (p. 763).” 10 Although an RCT cannot be compared with retrospective study statistically, we believe that the observed differences between the studies are due to some important and fundamental factors. In our study, when a diagnosis of MPM was confirmed histologically, surgery was offered without any further delay by 2 experience surgeons followed by chemotherapy and radiotherapy. However, in MARS, patients waited for long time in surgical arm before proceeding to operation. There was a median study design delay of 3.6 (2.8-4.3) months from registration (112 patients) to randomization (50 patients). In all, 53% patients were disqualified for clinical reasons (ineligibility, clinical decision, disease progression, and inoperability) before registration and 55.2% didn’t proceed to next stage of randomization mainly due to disease progression. Furthermore 6 (25%) patients in the surgical arm had disease progression and 2 patients refused surgery, subsequently 16 (67%) patients completed EPP, and 4 surgeons were involved. As a consequence of all these inherent delays and inconsistencies, only 8 (33%) patients completed the full trial treatment. 10
We know MPM is an aggressive disease and has a very poor survival without treatment. First, we believe that the inherent study design delays in the MARS trial resulted in disease progression thus contributing to the poor surgical outcome they observed. Second, there was no strong evidence for the role of neoadjuvant chemotherapy prior to mesothelioma surgery at that time of the MARS trial and that has not improved as of the time of writing this article. Again we suggest this inherent delay resulted in delaying surgery and allowed disease progression. Third, while all the analysis in the trial were by intention to treat analysis, the outcome in surgical arm emerged poorer as only one-third (8 patients) of patients in a small group received the full intended trial treatment. On comparing the 2 groups in MARS, the no EPP group had fairly uniform treatment, while in the EPP group, only one-third received chemotherapy, one-third received chemotherapy + EPP, and only one-third completed the proposed trial treatment, this group variance contributed to the statically poor outcome in surgical arm. Our chosen treatment pathway is contrary to that described in MARS, that is, early surgical cytoreduction delivered by only 2 experienced surgeons with a special interest in mesothelioma surgery, followed by adjuvant treatment delivered by a specialist oncology team. We believe that this approach is the major reason for the differences we report here.
This is one of those controversial pilot studies that was detrimental to the management of malignant mesothelioma worldwide. The overinterpretation of data and the statement “radical surgery in the form of EPP with trimodal therapy offers no benefit and possibly harms patients” 10 adversely affected the physicians, oncologists, and surgeons which resulted in the withdrawal of the surgical treatment in the trimodal therapy especially EPP. Although the United Kingdom possesses the highest incidence of mesothelioma in the world, National Thoracic Surgery Database Report 2011 of The Society for Cardiothoracic Surgery in Great Britain and Ireland has reported only 12 EPP performed in both countries during last 3 years, though there was no operative mortality. The controversial results of MARS and its acceptance as a milestone trial have been criticized worldwide. At the conference of International Mesothelioma Interest Group (IMIG) 2012, it was discussed with all participants, including the coauthor of the MARS-trial, and all agreed on the limitations and wrong perception of the trial. The recommendations from IMIG 2012 are that pathological diagnosis, including histological subtype, should be established by tissue biopsy, clinical staging be performed prior to initiation of therapy including PET scan with lymph nodes sampling, and/or magnetic resonance imaging as indicated. Surgery should be considered in appropriate patients with the goal of MCR, and the type of surgery (EPP and P/D) should be based on clinical factors as well as individual surgical judgment and expertise. The complete surgical staging should include hilar and mediastinal lymph node removal. 20
Our study has some limitations. It was a small retrospective, noncontrolled study of a cohort that received variable treatment. Regarding adjuvant therapies, patients were also referred from the peripheral hospitals and discharged back after surgery, and a local oncologist decided their adjuvant treatment. While most oncologists were not convinced about the efficacy of trimodality therapy initially, later we developed a complete trimodality treatment plan in our institution for all patients. Obviously the cohort of patients was highly selective; most of them had epitheloid histology and were young and healthy without significant comorbidities. Older patients and patients with sarcomatoid histology and severe comorbidities were turned down for surgery. Although the patients with aggressive disease were denied for surgery, 83% of patients were stage III and we did not limit EPP to patients with very early-stage disease. In the absence of a control group, the evident survival benefit might reflect the patient selection and variable natural history of mesothelioma. However, Merritt et al have shown median overall survival of 7 months of 101 patients with MPM treated palliatively. 21
In conclusion, we demonstrated improved short- and long-term outcomes for EPP in this study that are comparable with those reported international studies. The MARS trial showed significant disease progression in most of the patients due to a prolonged preoperative period and we suggest this demonstrates that early surgical cytoreduction is important. In our experience, 3 (10%) patients survived more than 7 years and this would be difficult to achieve by medical treatment alone. It is our contention that radical surgery including EPP in the management of MPM should not be discouraged on the basis of a single controversial feasibility study (MARS) that itself had to be abandoned and was doomed to fail through its inherent study design flaws. We suggest that all patients with MPM should have access to specialist treatment, and this may not be available locally. These patients should be referred to teams who have an interest and experience in mesothelioma surgery and expertise in perioperative management and the specialist oncology services that are all necessary in order to achieve the kind of results we report. We advocate that EPP can be performed safely with low mortality through proper staging, appropriate patient selection, better surgical technique, advanced perioperative monitoring, and better critical care support in a multimodality setting. However, the latest neoadjuvant and adjuvant therapies such as hyperthermic intraoperative intracavitary chemotherapy 22,23 and intensity-modulated radiation therapy should be considered as a part of multimodality therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.