
Abstract
Over the past decade, health literacy has received increased attention as a tool for promoting health, well-being, and sustainable development. So far, educational approaches to health literacy have mainly been implemented in health sciences education and linked to the needs of health professionals in communication with patients. The main objective of this systematic scoping review was to investigate health literacy educational approaches in higher education study programs, including the covered content and the learning activities employed. Altogether, 26 studies on health literacy training in higher education study programs were included. The most frequent study programs represented were medicine and pharmacy. A wide range of health literacy content was extracted from the studies; by far the most frequently studied skill was patient communication, which was identified in 20 studies, followed by identification of patients with low literacy in 12 studies and conceptual knowledge of health literacy in 11 studies. All studies except one reported the use of student active learning as part of the educational approach, and 17 studies reported the use of educational technology. The scientific literature indicates that current health literacy educational approaches mainly focus on the individual components of health literacy and fail to address environmental components and health literacy in vulnerable population groups. Despite the rather extensive use of active learning in educational approaches, pedagogical foundations were scarcely reported. In addition, the use of educational technology was rarely pedagogically integrated.
Introduction
Health literacy refers to the cognitive, technological and social skills that influence an individual’s motivation and ability to acquire, understand, evaluate, and use information to promote and support good health (Nutbeam, 1998, p. 357). Over the past decade, health literacy has received increased attention as a tool for promoting health, well-being, and sustainable development (Okan et al., 2019).
In his early work on health literacy, Nutbeam (2000) suggested that health literacy could be classified on the basis of what it enables us to do as persons: basic/functional literacy—sufficient skills in reading and writing to be able to function effectively in everyday situations; communicative/interactive literacy—more advanced cognitive and literacy skills that, together with social skills, can be used to actively participate in everyday activities to extract information and derive meaning from different forms of communication and to apply new information to changing circumstances; and critical literacy—more advanced cognitive skills that, together with social skills, can be applied to critically analyze information and to use this information to exert greater control over life events and situations (Nutbeam, 2000).
Despite the fact that Nutbeam’s expanded definition of health literacy hinted toward the environmental conditions that support health literacy in populations, the focus of health literacy research is still on the social and cognitive skills of the individual (Smith & Ireland, 2020). Recent research has reinforced the view that health literacy is both an individual and population endeavor (Smith & Ireland, 2020). It has been argued that to improve health literacy in the population, it is necessary to address personal knowledge, motivation and competences to enable well-informed health decisions, and to decrease the complexity of society and of the health care system (Sørensen et al., 2015). Healthy People 2030, which identifies public health priorities to help individuals, organizations, and communities across the United States improve health and well-being, defines health literacy as Personal health literacy and Organizational health literacy (Santana et al., 2021). Personal health literacy is the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others (Santana et al., 2021). Organizational health literacy is the degree to which organizations equitably enable individuals to find, understand, and use information and services to inform health-related decisions and actions for themselves and others (Santana et al., 2021). A similar expanded definition of health literacy has been advocated by the Australian Commission on Safety and Quality in Health Care, which defines the health literacy environment as the infrastructure, policies, processes, materials, people, and relationships that make up the health system and have an impact on the way that people access, understand, appraise, and apply health-related information and services (Australian Commission on Safety and Quality in Health Care [ACSQHC], 2014). The need to recognize that addressing health literacy requires a coordinated and collaborative approach to integrate health literacy into areas such as education, has been highlighted (ACSQHC, 2014). Action needs to be taken on embedding health literacy into systems, ensuring effective communication and integrating health literacy into education (ACSQHC, 2014).
A few reviews have reported on health literacy education within various health and higher education contexts. One review on teaching health literacy principles to health care professionals concluded that low health literacy must be addressed by all professionals to improve the quality of outcomes (C. Coleman, 2011). The author argued that more educational research is needed to determine which health literacy competencies should be taught, to which health care professionals, in what settings and by which teaching methods (C. Coleman, 2011). Another systematic review of the literature on health literacy in nursing education revealed limited and inconsistent health literacy content in nursing curricula (McCleary-Jones, 2016). The author concluded that it is important that nursing curricula include information on health literacy regarding the implications that limited health literacy can have on patient outcomes and strategies to meet the patients’ health literacy needs (McCleary-Jones, 2016). A more recent review aiming to identify core elements for a conceptual framework for a health literacy curriculum in health professions education found that the most successful interventions were those that offered numerous training sessions and integrated knowledge and skill acquisition within real-world settings (Saunders et al., 2019). A health literacy curriculum framework consisting of core aspects and best practice teaching elements was recommended (Saunders et al., 2019).
To date, educational approaches to health literacy have primarily been implemented in health sciences programs, with a focus on addressing low health literacy among patients or clients. While the health literacy literature emphasizes enabling individuals to make optimal health choices for themselves, there has been limited attention given to the pedagogical methods used in educational approaches targeting health literacy. Recently, there has been an expanded focus on health literacy research, making it relevant across various higher education disciplines. Therefore, the main objective of this systematic scoping review was to investigate health literacy educational approaches in higher education study programs, including the covered content and the learning activities employed. A secondary objective was to assess the extent to which these educational approaches align with the current scientific knowledge base.
Method
This systematic scoping review focuses on the teaching and learning approaches of health literacy in higher education study programs, as reported in published peer-reviewed papers. The scoping review was based on recommendations and an updated guideline from the Joanna Briggs Institute (Arksey & O'Malley, 2005; Levac et al., 2010; Peters et al., 2020). In addition, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) checklist was used for the planning of the study (Tricco et al., 2018). The current scoping review was registered and made publicly available for research on the OSF database (https://osf.io/upzjb/) on September 17, 2021.
The principles for generating breadth of coverage were emphasized during the development of the eligibility criteria for the review (Arksey & O'Malley, 2005). The criteria were developed and refined through test searches and in collaboration with the OsloMet research librarian service. Based on these adjustments, the final inclusion criteria were primary studies of any type of methodological design, a dominant focus on teaching and learning of health literacy, an educational approach as part of the curriculum in a higher education study program and publication in English or in a Scandinavian language in a peer-reviewed journal within the past 10 years. Studies were excluded if health literacy was not the dominant concept, if proxies were used for health literacy (e.g., “health communication,” “patient education”), if the location was a clinical setting (e.g., hospitals, primary care facilities) or if the study did not concern content and teaching methods (e.g., students’ experiences).
The electronic databases CINAHL, ERIC, MEDLINE, PsycINFO, Web of Science, Education Source, and Google Scholar were searched. First, a search strategy for MEDLINE was developed and then adapted for the other databases. The final search was carried out simultaneously in all databases on December 16, 2021. The extensive search history material is available in Supplemental Appendix 1.
The selection of studies is displayed in Figure 1. The selection and the extraction of study content were conducted using the Covidence software (https://www.covidence.org/) and informed by recommendations from Levac et al. (2010). In total, four authors (YR, AT, BS, and KR) participated in the selection and extraction of the studies. The selection of studies consisted of two steps: abstract and full-text screening. Before the abstract screening, a workshop was arranged in which borderline cases were discussed and inclusion and exclusion criteria adjusted. Thereafter, all abstracts were screened independently by random pairs of two team members. Conflicts between reviewers were solved through discussion. In cases where the team members were unsure, studies were treated as eligible for full-text screening. Next, the full text was retrieved for all studies included after the abstract screening. The full-text screening followed the same procedures as the abstract screening.
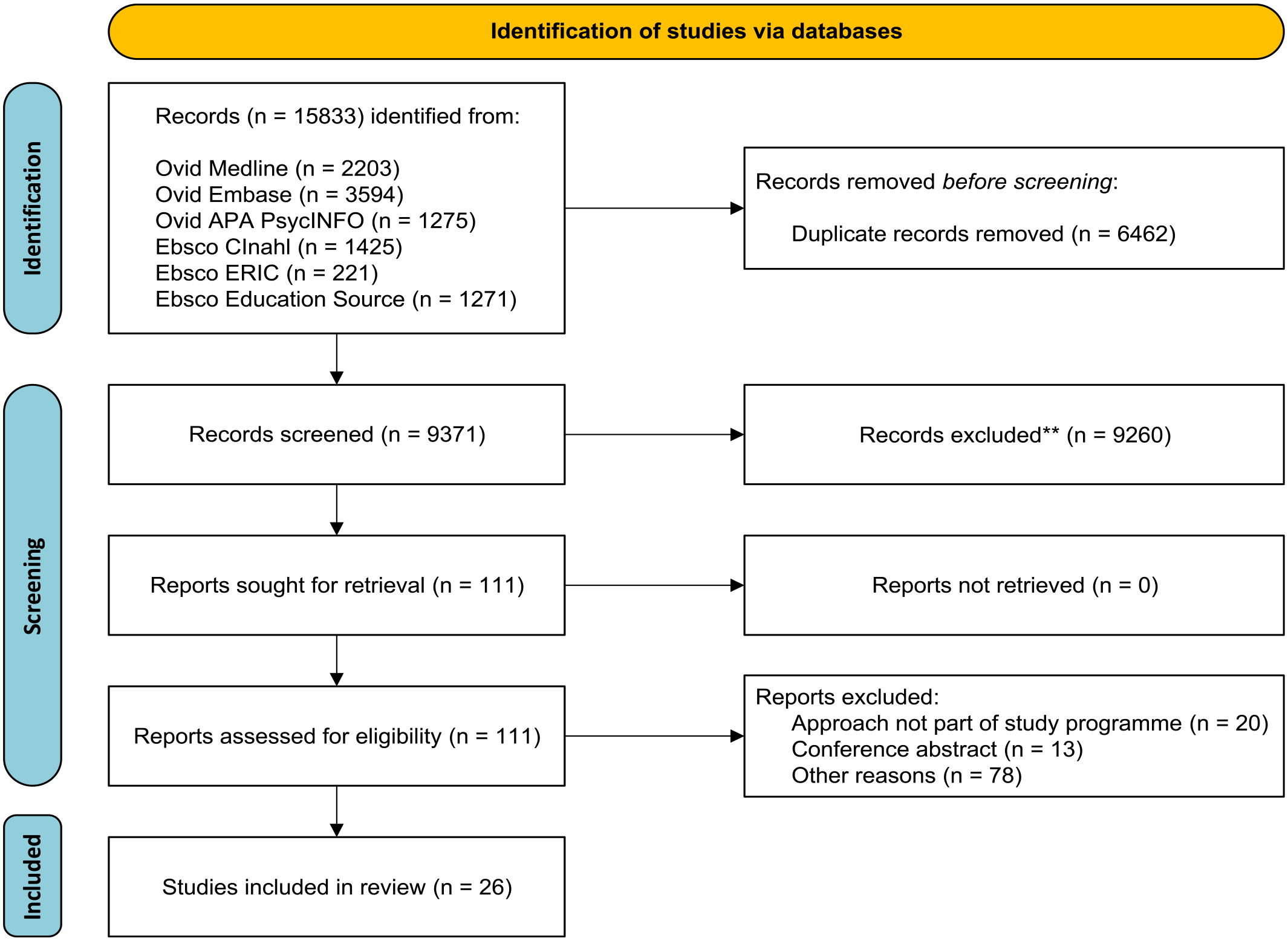
Prisma flow diagram displaying the inclusion of studies.
All studies were extracted by two authors (YR and KR). A preliminary chart to extract the data was set up and further refined during the extraction. The findings were synthesized and presented in the form of a narrative summary and a table. Firstly, we provided a summary of the characteristics of the studies. Secondly, we reported on the health literacy educational content. In the third step, we summarized the learning activities employed in the educational approach, specifically highlighting any pedagogical use of technology, feedback mechanisms utilized in learning, and references to pedagogical models or frameworks.
Findings
Altogether, 26 studies on health literacy training in higher education study programs were included (Table 1). Of these studies, 24 took place in the United States, one in the Netherlands and one in Canada. Eight studies were published in 2020 or later, indicating an increasing publication rate. The most frequent study programs were medicine and pharmacy, each represented in eight studies. Nine other studies were conducted in other health sciences education or public health programs, while one study within an interdisciplinary context. Of the included studies, 12 described educational approaches at the bachelor’s level and 13 at the master’s level, while one study did not specify the level.
Characteristics, Educational Content and Learning Activities of Selected Studies.
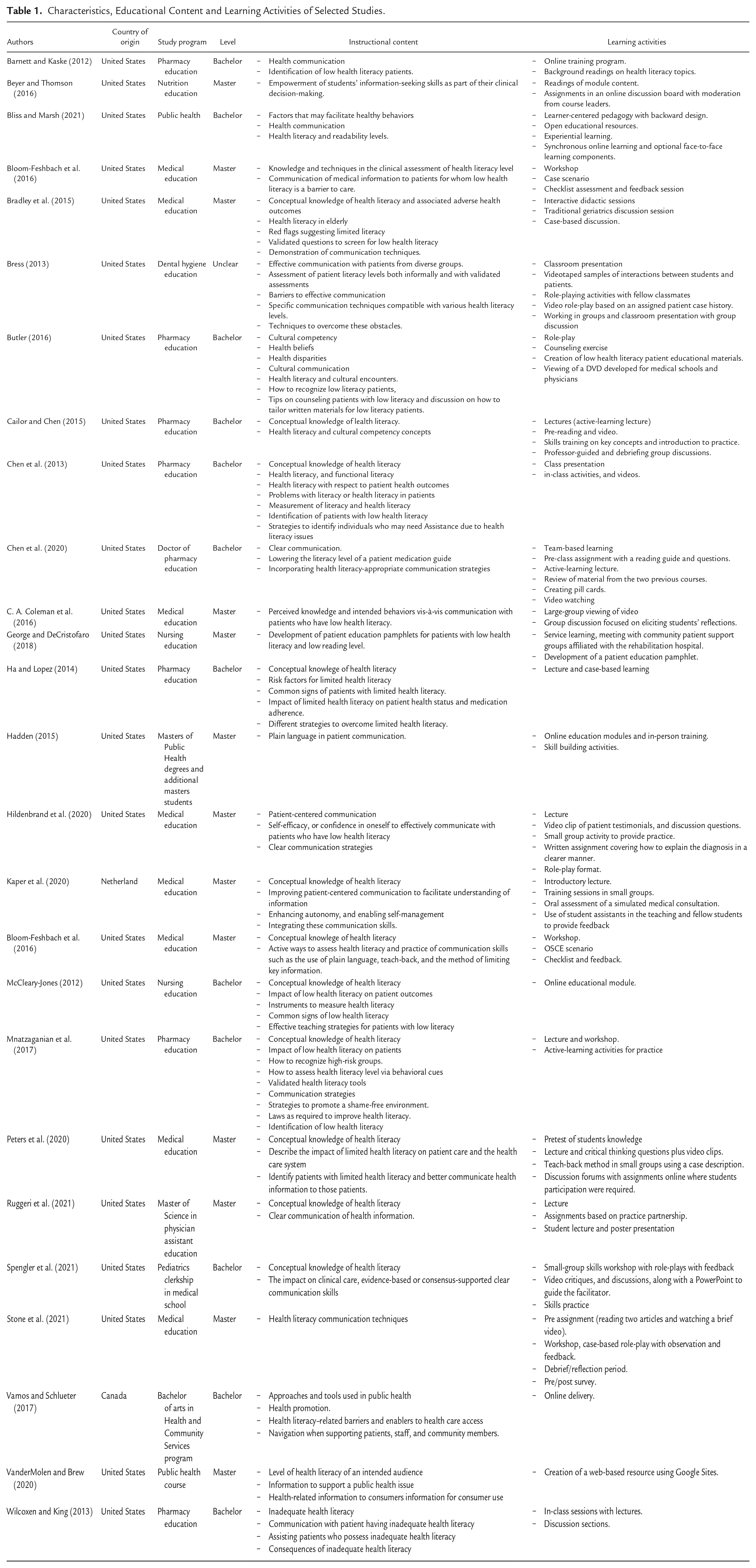
A wide range of educational content that focuses on health literacy skills, was extracted from the studies (Table 1);by far the most frequent was patient communication, which was identified in 20 studies, followed by the identification of patients with low literacy in 12 studies and conceptual knowledge of health literacy in 11 studies. Assessment of literacy level, implications on health outcomes and health promotion/empowerment were other frequent health literacy–related concepts included in the programs. Only two studies targeted specific population groups (elderly and diverse populations). Four studies referred to validated measures of health literacy, while several others referred to identification of health literacy level by behavioral signs or by other means.
All studies except one reported using student active learning as part of the educational approach (Table 1). A range of theoretical and practical active learning methods were mentioned (e.g., pre-class assignments, online discussion boards, case scenarios and role-playing). Moreover, an overwhelming majority of studies reported the use of creative and evaluative learning activities, which were often linked to real-world problems, such as simulation of communication with patients with low health literacy.
Of the included studies, 17 reported the use of educational technology, including basic learning activities such as watching videos. Of these, two were designed as online modules, while the rest combined digital material with in-person learning. Seven studies explicitly mentioned feedback methods, such as moderation from the course leader or the use of student assistants to provide feedback. Only one study, which drew on team-based learning, reported the use of a specific pedagogical model in the design.
Discussion
This systematic scoping review aimed to investigate health literacy educational approaches in higher education study programs and extract their content and the educational methods. Interestingly, the included studies showed a skewed representation, as medical and pharmacy education accounted for almost two-thirds of the studies. Although we expected health sciences education to be dominant, we also anticipated to find some representation of health literacy education within other higher education disciplines. With the recent discourse in health literacy research on the importance of reducing health inequities and empowering communities to exert control over the determinants of their health, a more heterogeneous representation of study programs and disciplines might have been expected (Smith & Ireland, 2020). However, it seems that the recent research discourse in health literacy has not yet been adopted by higher education disciplines which are more population-, or system focused.
In terms of the educational content covered in the studies included in this review, the most frequent concepts were patient communication, identification of patients with low literacy and conceptual knowledge of health literacy. All these concepts are also suggested as learning scopes in the proposed conceptual framework for health literacy training in higher education (Saunders et al., 2019). It should be noted, however, that another learning scope in the framework (Saunders et al., 2019), measurement and comparison with validated measures, was only found in four of the studies (Bradley et al., 2015; Bress, 2013; Chen et al., 2013; McCleary-Jones, 2012). In contrast, several other studies referred to the use of non-standardized methods, such as the identification of common signs of low health literacy. We would recommend that future educational approaches rely on validated measures in the identification of low health literacy.
Recent understandings emphasize that health literacy research consists of both personal competencies and organizational structures, resources and commitment (Santana et al., 2021; Sørensen et al., 2021). The organizational component comprises the degree to which organizations equitably enable individuals to find, understand, and use information and services to inform health-related decisions and actions for themselves and others (Santana et al., 2021). Nevertheless, this component was rarely described in the material. Except for two studies that included laws as required to improve health literacy (Mnatzaganian et al., 2017) and the impact of limited health literacy on patient care and the health care system (Roberts et al., 2012), all the content covered by the educational approaches belonged to the individual component (Santana et al., 2021). It has been recommended as a research priority to improve the quality of health communication to attend to the diversity of populations and engage those population groups disproportionately affected by low health literacy (Nutbeam & Lloyd, 2021). The studies included can be criticized for failing to address vulnerable population groups in their educational content. Drawing on the knowledge base in health literacy research, we recommend that future educational approaches to health literacy strengthen the focus on health systems and population groups to increase students’ knowledge and critical understanding of diversity.
Strategies promoting active learning can be defined as educational activities involving students in doing things and thinking about what they are doing (Bonwell & Eison, 1991). As mentioned, the majority of the studies had a dominant focus on patient communication and other key clinical skills, with a particular emphasis on active learning methods, such as role-play and discussions. Moreover, with the exception of one study based on team-based learning (Chen et al., 2020), no study referred to specific pedagogical models of teaching and learning. Health literacy education should aim to apply the highest possible pedagogical standards. Our analyses indicate room for improvement in the pedagogical foundations of the educational approaches. As an example, the Bloom’s taxonomy is a valuable tool to map the teaching and learning methods used in a course or unit (Anderson et al., 2001; Krathwohl, 2002). In the taxonomy, learning activities are categorized according to their knowledge dimension (factual, conceptual, procedural and meta-cognitive) and their cognitive process dimension (remembering, understanding, applying, analyzing, evaluating and creating; Anderson et al., 2001; Krathwohl, 2002). We also suggest that students participate in learning activities to construct their knowledge in their context, aligned with intended assessment tasks (constructive alignment; Biggs & Tang, 2011).
In higher education, digital competence is increasingly linked to working relevance, education and lifelong learning for citizens (Digital Education Action Plan (2021–2027), 2021; European Commission Directorate-General for Education, & Culture, 2019; Vuorikari et al., 2022). Within health literacy research, it has been claimed that it is critical not just to provide the information but also utilize digital technology to help receivers seek, evaluate and analyze the quality of information important to improve health literacy and health (Sørensen et al., 2021). From the included studies, we found that more than two-thirds reported on the pedagogical use of technology in educational approaches. Nevertheless, the extent of technology integration in the learning activities was scarcely described. Future educational approaches to health literacy should adhere to this transformation and include the technology in a way that enables students to learn effectively and facilitates their understanding of how the technology might influence health literacy in patients and the population.
This review has some limitations. First, only studies of educational approaches in which health literacy was explicitly used as a dominant concept were included. Consequently, studies using overlapping terms or studies mixing different concepts were excluded. Nevertheless, we think this rather narrow understanding can be justified by the aims of our study and the distinct theoretical underpinnings of health literacy (Sørensen et al., 2012). Second, only educational approaches that were part of a course or study program in higher education were included. This mean that trials including students and educational approaches in health care settings were excluded. Third, the present study does not provide a complete picture because only studies published in peer-reviewed journals were analyzed. Grey literature, such as committee reports, government reports, conference papers, and ongoing research, can make important contributions to a systematic review (Paez, 2017). Thus, the extent to which our findings are representative of all educational approaches is difficult to determine.
Conclusions
According to the content covered, the studies included in this review mainly focus on the individual components of health literacy and fail to address organizational components, or health literacy in vulnerable population groups. Based on the scientific literature, an overwhelming majority of current health literacy educational approaches take place in the United States. Of the study programs researched, medicine and pharmacy education accounted for the majority, while we found no reports on health literacy approaches outside health sciences education. Despite the rather extensive use of active learning, pedagogical foundations were scarcely reported in the studies. In addition, the use of educational technology was barely pedagogically integrated, nor linked to the opportunities and challenges provided by the digital transformation in health care. Hopefully, the findings of the review will inform the future development of health literacy education.
Supplemental Material
sj-docx-1-php-10.1177_23733799231191107 – Supplemental material for Health Literacy in Higher Education: A Systematic Scoping Review of Educational Approaches
Supplemental material, sj-docx-1-php-10.1177_23733799231191107 for Health Literacy in Higher Education: A Systematic Scoping Review of Educational Approaches by Yngve Røe, Astrid Torbjørnsen, Brita Stanghelle, Sølvi Helseth and Kirsti Riiser in Pedagogy in Health Promotion
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.