
Abstract
To be effective, school health instruction should be taught by health educators who have graduated from accredited health education teacher education programs and are certified in health education. Unfortunately, the nation has failed to ensure that all those who teach health in schools are well prepared. States vary in the required coursework for health teachers in terms of initial licensure and continuing education for licensure renewal; most elementary teachers are not required to receive preparation in health education; health education and physical education are often viewed as synonymous disciplines; support for in-service education of health teachers is often lacking; and more research is needed in professional preparation and development of school health educators. This article provides a call to action in five areas to strengthen both the professional preparation and professional development of school health educators. Given that education is a social determinant of health, public health educators must become stronger allies in supporting school health to promote health equity. Public health practitioners can advocate to state and community school decision makers for comprehensive school health education taught by teachers with appropriate professional preparation and certification in health education. Public health faculty can educate their students about the Whole School, Whole Community, Whole Child framework and effective strategies for its implementation, and seek rigorous professional preparation and certification and accreditation standards for their school teacher preparation programs. National health and education organizations can call for new leadership and investments in health education teacher preparation and development for a brighter future.
Keywords
The health education profession is committed to quality assurance and credentialing of both individuals and higher education professional preparation programs (i.e., teacher education programs) for all health educators, including those who teach health in schools. Maintaining high standards for the professional preparation and professional development of school health educators ensures they are well-prepared to help preK–12 students acquire the health-related knowledge and skills they need for a safe and healthy life. Although this goal is not new, the nation has failed to ensure that all those who teach health in schools are well prepared (Allegrante et al., 2004; Hammig, Ogletree, & Wycoff-Horn, 2011; Smith, Potts-Datema, & Nolte, 2005). This article and the complementary articles also found in this issue suggest some reasons for this failure (Mann & Lohrmann, 2019; Videto & Dake, 2019). This article proposes five recommendations for strengthening both the professional preparation (i.e., preservice) and continuing education (i.e., in-service) of health education teachers.
Background on Teacher Professional Preparation
According to Darling-Hammond (2010), quality teacher education is “essential to the nation’s future” (p. 36). Based on research findings, both Levine and Grant (2005) and A. Goodwin et al. (2014) concluded that the most important factor related to student learning and achievement was the teacher. Thus, higher education must equip teacher candidates with the pedagogy and skills they need to teach in contemporary classrooms.
Both individual (e.g., teacher candidates, practicing teachers) and institutional stakeholders (e.g., state boards of education, higher education institutions preparing teachers, school districts, and professional development providers) have a responsibility to assure the quality of the health instruction children receive in school. Teacher preparation institutions can demonstrate their commitment to professional standards through state accreditation and/or recognition of their health education teacher preparation program by the Council for the Accreditation of Educator Preparation (CAEP), which over half the states require (CAEP, 2018b). Individuals working in schools as health teachers can contribute to quality assurance by obtaining state teacher certification/licensure, the voluntary Certified Health Education Specialist (CHES/MCHES) designation, and/or the voluntary credential by the National Board of Professional Teaching Standards (2019).
Education leaders recognize that all teacher education programs face some common challenges. These issues include program content, methods, and goals (Arbaugh, Ball, Grossman, Heller, & Monk, 2015; A. Goodwin et al., 2014; Kennedy, 2016); methods for addressing diversity, inequality, and social justice (Mills & Ballantyne, 2016; Tatto, Richmond, & Carter Andrews, 2016); the intersection of technology and teacher education (Arbaugh et al., 2015); professional development needs of teacher educators (Loughran, 2014); and the identification of needed research directions (Cochran-Smith & Villegas, 2015; Tatto et al., 2016). Because accreditation of teacher education programs and the related certification requirements vary by state, achieving uniform national professional standards for teacher preparation is a daunting task (Taub et al., 2014).
The above challenges apply to all teacher preparation programs, including health education. Yet there are also issues unique to health education such as the limited health education presence in the professional preparation of elementary education and special education majors as well as misunderstanding about the distinction between health education and physical education. This article identifies specific challenges related to the quality assurance of professional preparation and professional development of school health educators, provides pertinent background information, and recommends actions for addressing the challenges.
Challenge #1: Ensure that Teachers Delivering Health Instruction have had Quality Preservice Education in Health Education
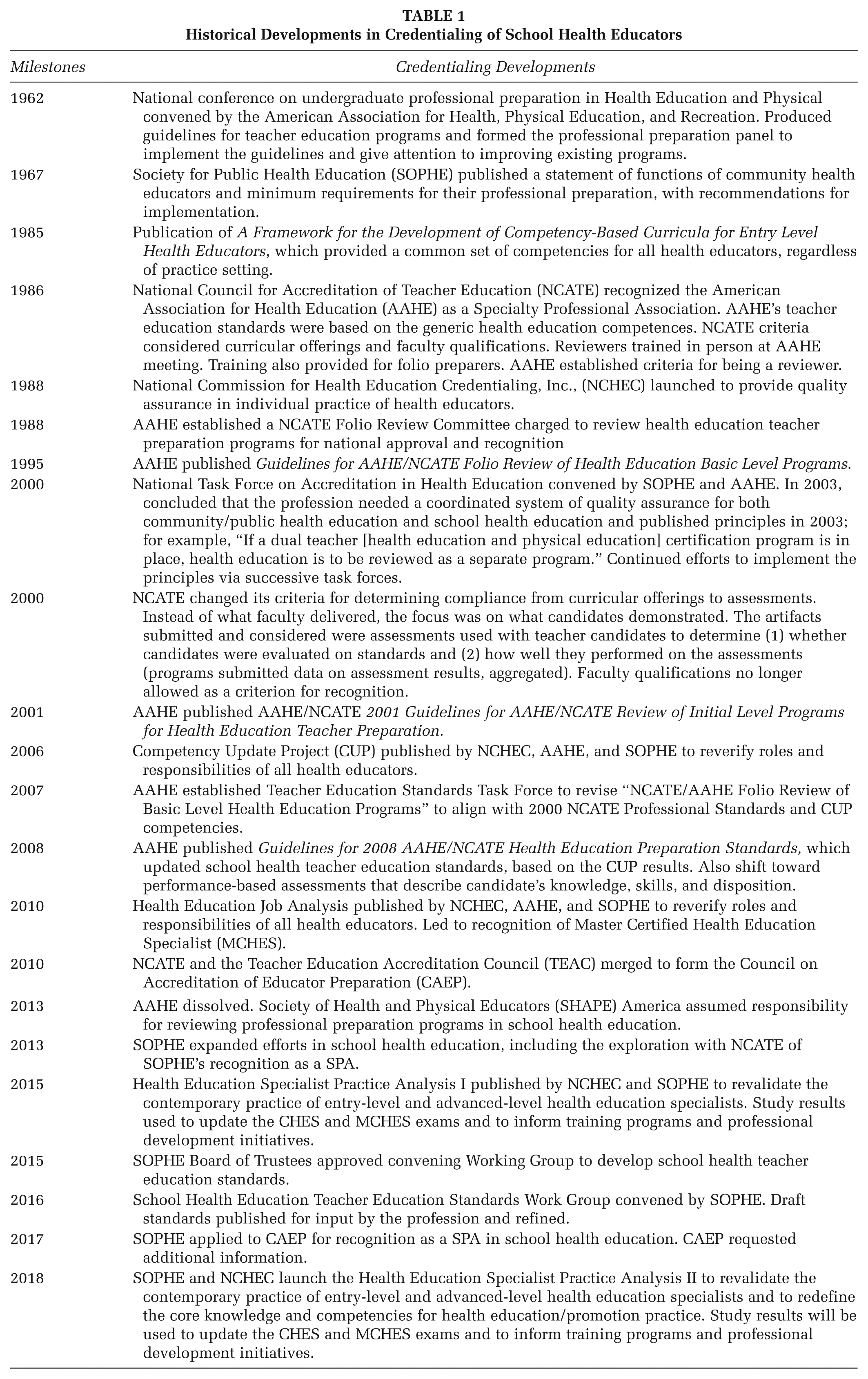
Until the 1980s, no national standards existed for training school health education teacher candidates nor did qualifications exist for higher education faculty preparing school health teachers. Beginning in the 1980s, the American Association for Health Education (AAHE)–led profession-wide efforts to set standards that guided curricula for preservice school health education. In 1986, The National Council for the Accreditation of Teacher Education (NCATE) recognized AAHE’s parent organization, the American Alliance for Health, Physical Education, Recreation and Dance (AAHPERD), as the Specialized Professional Association (SPA) for health education professional preparation (Taub et al., 2014). SPAs set standards and review teacher preparation programs for compliance with the standards. Initially, NCATE accepted the competencies expected of all health educators as the standards for preparing school health education teacher candidates 1 (Hillman et al., 2010). While some states adopted the NCATE competencies for health educators, other states set their own requirements for approving professional preparation programs. State education agencies also set certification standards for individual health teachers. The U.S. Department of Education and the Council for Higher Education Accreditation recognized several accrediting agencies for higher education programs preparing either school or public health educators (see Figure 1). Table 1 presents a chronology of other major milestones in the evolution of credentialing of the school health education profession.
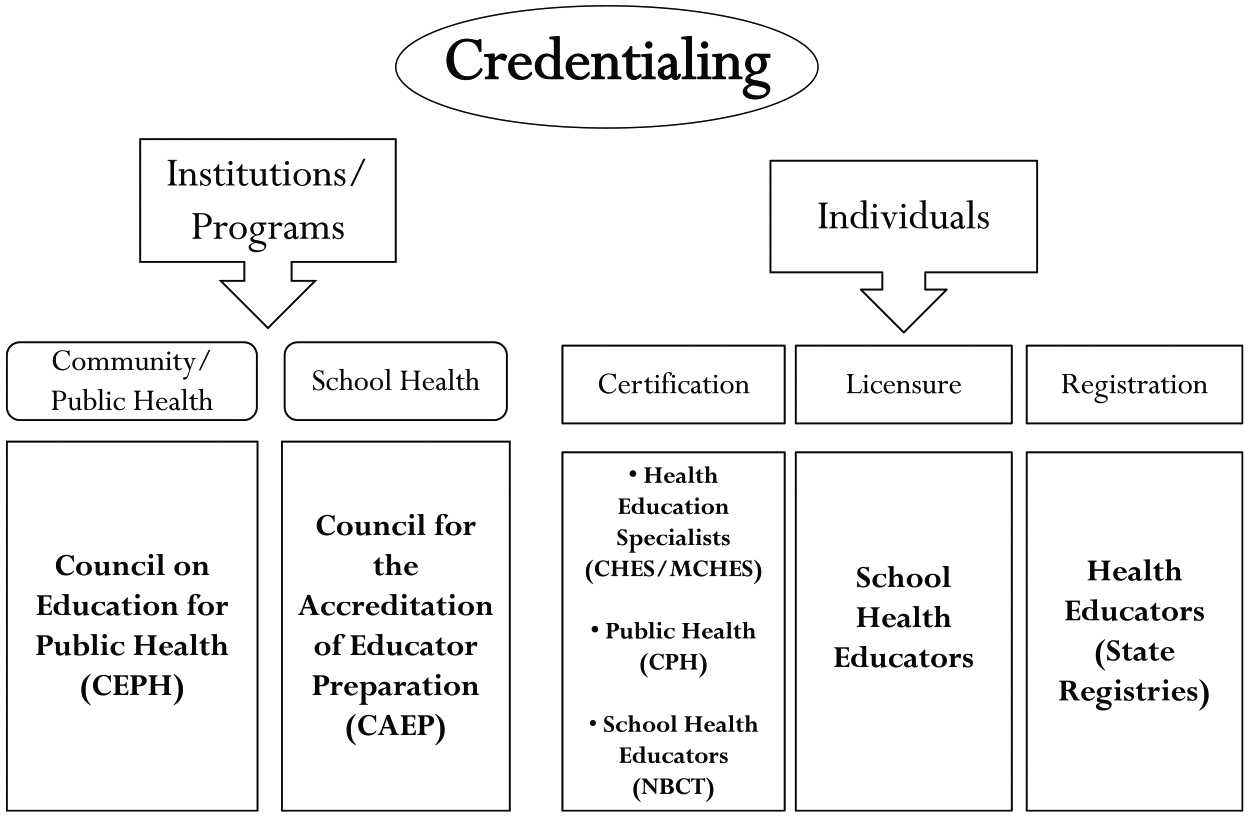
Overview of Health Education Credentialing in the United States
Historical Developments in Credentialing of School Health Educators
Although national standards now exist for professional preparation of health teachers and although most states require newly hired health teachers to be credentialed in health education, states vary in the required coursework for initial licensure and continuing education for licensure renewal. Data from the Centers for Disease Control and Prevention (CDC) School Health Policies and Practices Study (SHPPS) indicate that of districts that had adopted specific staffing policies for newly hired staff, only 67.8% required those who teach middle school health to be licensed, certified or endorsed in health education and only 78.4% required that of high school health teachers (CDC, 2016). Some states required licensure, certification or endorsement in health education only for those middle or high school teachers whose primary responsibility was health education instruction. If an educator taught only one or two health classes, and the remainder of the teaching load was in another content area, the teacher might not need any health education training.
Professional background of faculty assigned to teach certain courses can also be an issue in higher education. Authors of this article who have served as SPA portfolio reviewers for health education teacher preparation programs note that many programs employed no faculty members who had professional preparation as health educators. This might be partially due to fewer doctoral students being prepared in school health education. Kolbe (2019) notes that during the past 30 years, many professional preparation programs related to school health education shifted from colleges of education to colleges of public health and health sciences. Clark and Olsen (2016), in a national study of health education doctoral programs, found that only 6 programs out of a total of 56 doctoral programs offered an emphasis in school health education. Only 3 of the 6 programs had students enrolled in the school health education emphasis. In 2005, AAHE recommended that “All persons who are responsible for teaching health education at the middle and high school levels should be required to have a separate certification in Health Education” (American Association for Health Education, 2007-2008, p. 7). The AAHE Position Statement also addressed professional preparation, declaring, . . . Far too many school districts across the nation hire teachers of health education who are inadequately prepared. Many of the nation’s health education teachers have their primary credential in an area other than health, leaving students with health teachers with expertise in physical education, history, math, science or other subjects. (p. 7)
This is of concern given that positive student outcomes are more likely to be achieved when students are taught by teachers who teach a subject for which they are prepared (Stronge, 2018). The 2016 SHPPS found that less than 70% of a representative sample of school districts within the United States required that newly hired staff who teach health at the high school level had academic training in health education and less than 60% at the middle school level (CDC, 2016). This is consistent with the 2014 SHPPS school-level data, which found that 70% of high schools, 54% of middle schools and 36% of elementary schools required that newly hired health teachers have “undergraduate or graduate training in health education” (CDC, 2015).
Recommendations for Addressing Challenge #1
At the secondary level, hire professionals who are both certified in health education and have an academic major in health education for positions that include teaching health.
At the professional preparation level, hire faculty for health education teacher preparation programs who are professionally prepared school health educators and who have experience teaching health education in the middle or secondary school settings.
Select cooperating/supervising teachers for health education student internships (i.e., student teaching) who are professionally prepared in health education, ideally from an institution with a CAEP and/or state-recognized program.
Advocate with teacher certifying bodies for proper credentialing and professional preparation for those assigned to teach health.
Challenge #2: Ensure that Classroom Teachers at the Elementary Level who teach Health Receive Professional Preparation that includes Health Education
In 2010, NCATE and the Teacher Education Accred-itation Council (TEAC) unified to become the Council on Accreditation of Educator Preparation (CAEP; Taub et al., 2014). CAEP published new accreditation standards and processes in 2013 requiring educator preparation programs to provide evidence of educational outcomes. CAEP’s review includes all specialty areas that prepare candidates to work in preK–12 settings and lead to a professional license, certificate, or endorsement; it also includes graduate and noncertification programs for licensed educators who are extending their knowledge and skills for working in school settings (CAEP, 2016). Although CAEP’s Elementary Education teacher preparation standards include competency in teaching many subjects, health is not one of the specified subjects (CAEP, 2018a).
While certification in health education usually focuses on middle school and high school teachers, elementary teachers also provide health instruction and need professional preparation in the discipline (Benes & Alperin, 2016; English, 1994; Hausman & Ruzek, 1995; Patterson, Cinelli, Sankaran, Brey, & Nye, 1996; Seabert et al., 2002; Thackeray, Neiger, Bartle, Hill, & Barnes, 2002; Ubbes et al., 1999). Elementary teachers who received preservice education in health education and in physical education taught more health topics and taught health for more time than teachers not receiving such education (Seabert et al., 2002). Yet elementary teachers report a lack of preservice training in health education, low confidence in their ability to teach the subject, and discomfort with certain subject areas (C. Davis, Jelsma, & Van Valey, 1985; Hausman & Ruzek, 1995; Patterson et al., 1996; Thackeray et al., 2002; Ubbes et al., 1999). Elementary teachers reported being least comfortable teaching HIV/AIDS prevention, drowning first aid, sexual abuse, and stress and disease (Hausman & Ruzek, 1995). Special educators also lack training in health education because it is not considered an essential professional competency (Blanchette, 2002).
Although specific national health education standards exist for preK to Grade 2 and Grades 3 to 5 (American Cancer Society and Joint Committee on National Health Education Standards, 2007) and although Healthy People 2020 (Office of Disease Prevention and Health Promo-tion [ODPHP], 2019) includes an objective (EMC-4.1.1) supporting quality elementary health instruction (i.e., Increase the proportion of elementary schools that require newly hired staff who teach health education to have undergraduate or graduate training in health education), the quality of elementary health instruction in many school districts is insufficient.
Elementary classroom teachers have responsibility for multiple subjects and are proficient in working with young children. They could, thus, be appropriate health teachers at the elementary level (Benes & Alperin, 2016; Evans & Sims, 2016; Patterson et al., 1996). Few prospective elementary classroom teachers, however, receive professional preparation in health education; many lack both the content knowledge and health-related pedagogical skills needed to provide quality health instruction (Benes & Alperin, 2016; Hausman & Ruzek, 1995; Patterson et al., 1996; Seabert et al., 2002; Thackeray et al., 2002; Ubbes et al., 1999).
In 1992, a joint committee of AAHE and the American School Health Association (ASHA) released Health Instruction Responsibilities and Competencies for Elementary (K-6) Classroom Teachers. The joint committee recommended that elementary education majors take a three-credit preservice course focusing on health education in elementary schools and a three-credit personal health course that would provide the background information elementary school teachers need for teaching health education content. Both Ubbes et al. (1999) and English (1994) recommended that teacher training institutions require prospective elementary teachers to have the same level of course work in health education as they do in subjects such as math and reading. English recommended that this health education training include a personal health course as a prerequisite for a health education methods course. Hausman and Ruzek (1995) further recommended that state teacher certification require evidence of such training.
Recommendations for Addressing Challenge #2
Require preservice elementary education teacher preparation to include at least one preservice course that focuses on health literacy, the health needs of elementary school students, and elementary-age appropriate health content knowledge, plus at least one course that focuses on the pedagogical knowledge and skills needed for teaching elementary health education content (Association for the Advancement of Health Education and American School Health Association, 1992; Telljohann, Symons, Pateman, & Seabert, 2016).
Include in state elementary education certification requirements a three-credit preservice course that focuses on the role of health education in elementary schools; and a three-credit personal health prerequisite course with the background information necessary for teaching elementary health education content.
Challenge #3: Reduce the Acceptance of Dual Certification for Health Education and Physical Education and Dual Majors
Although school health education and physical education differ regarding national standards, student learning outcomes, instructional content and methods, and student assessment (Birch, Mitchell, & Priest, 2015), the two disciplines have a long relationship based on a common goal of promoting students’ health. S. C. Goodwin (1993) presented examples of the relationship between “hygiene” and physical education that were documented as early as 1838. In an historical perspective on the connection between the two disciplines for much of the 20th century, T. M. Davis and Hensley (1997) described the disciplines as “connected, even overlapping in the school curriculum” (p. 370). In a current context, health education and physical education are both included but are clearly distinct components of the Whole School, Whole Community, Whole Child (WSCC) framework developed collaboratively by CDC and ASCD and cited separately as distinct subjects in the 2015 Every Student Succeeds Act (ESSA) legislation (Lewallen, Hunt, Potts-Datema, Zaza, & Giles, 2015; Society for Public Health Education, 2017, 2019).
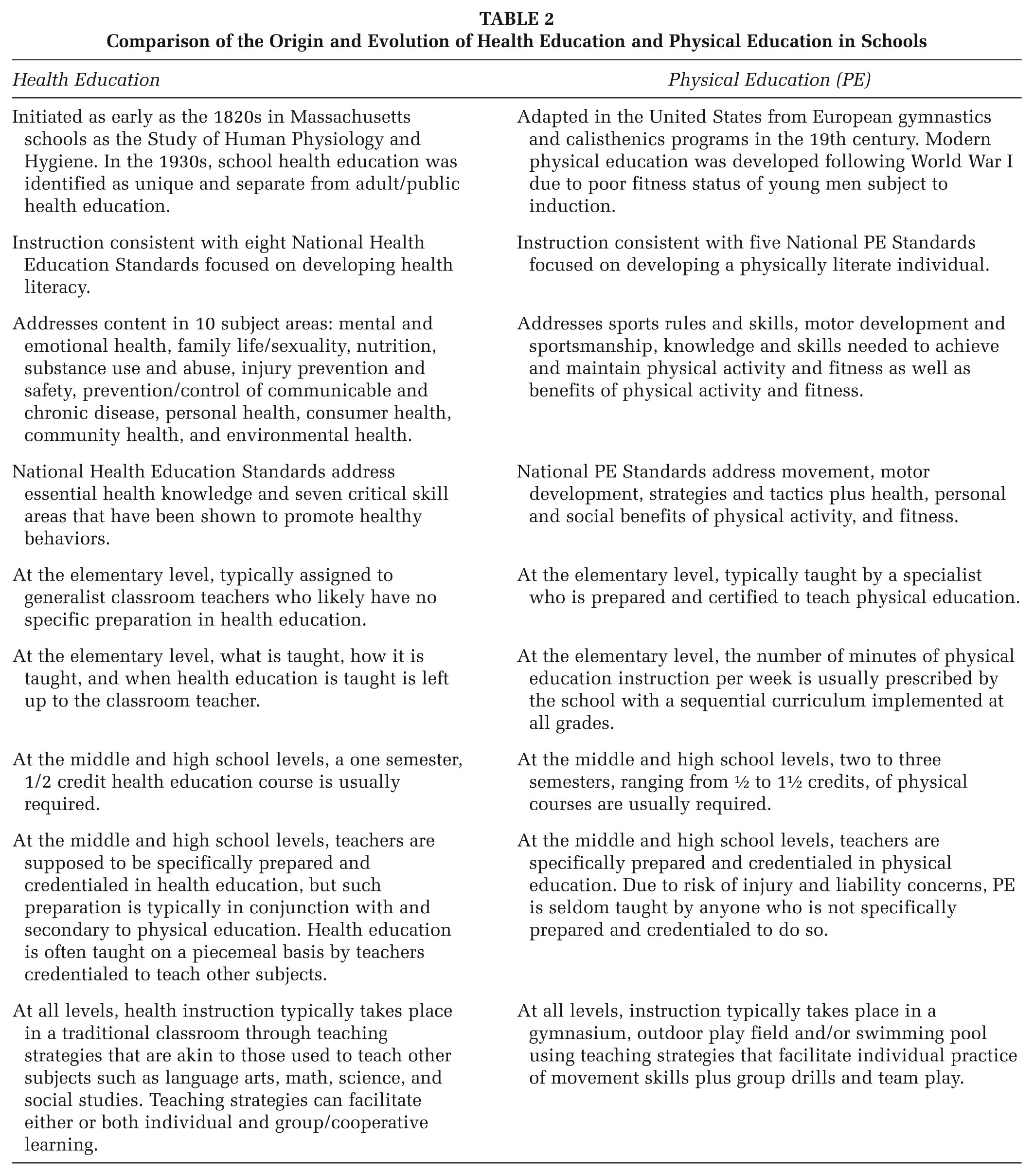
While few would argue against the potential benefits of a well-conceived partnership between health education and physical education, many educators do not understand the distinction between the two subjects. Professionals familiar with both disciplines recognize the differences between the two subjects and the importance of separate teacher education programs (Cleary & Gobble, 1990; T. M. Davis & Hensley, 1997; Sondag & Burns, 1998). In a 1981 Journal of School Health article, Cobb (1981) described the difference between the two disciplines: “each is a distinct area of instruction that requires special and unique professional preparation” (p. 603). In 2013, SOPHE’s School Health Education Accreditation Working Group reaffirmed that, “School health education and physical education are separate and unique disciplines and require distinct quality assurance standards and processes. All those assigned to teach health education in schools should be professionally prepared in health education” (Taub et al., 2014, p. 355). Table 2 describes some of the differences between the academic courses of health education and physical education.
Comparison of the Origin and Evolution of Health Education and Physical Education in Schools
Two authors of this article have decades of experience as official reviewers of teacher preparation program applications for recognition in health education as part of the NCATE and then CAEP accreditation processes. They have observed that teacher preparation programs in health education require substantially more health courses than do dual degree programs in health and physical education.
Representatives of the 2013 SOPHE School Health Education Accreditation Working Group said, The knowledge and pedagogical skills for teaching physical education and classroom-based health education are distinct. Also, the current health education and physical education PreK-12 student standards defining what students should know and be able to do have few similarities. Providing prospective teachers with adequate opportunities to become proficient in both physical education and health education requires more than the traditional 4-year undergraduate teaching course of study. (Taub et al., 2014, p. 352)
Health education and physical education have distinct national standards for instruction and for accreditation of teacher education programs, theoretical bases, instructional content and methods, and student assessment methods.
Cardina (2014) compared academic majors and subject-area certifications reported in the 2012 CDC SHPPS with the data from the U.S. Department of Education’s Schools and Staffing Survey 2011-2012. Both studies found that approximately 30% of health education classes were taught by teachers with an undergraduate or graduate degree in health education. Both studies found that secondary health education teachers often had academic degrees in physical education. This combined focus has resulted in teachers with varying levels of preparation in both subject areas. Often these combined programs place more emphasis on physical education and do not adequately prepare candidates to teach health education (Cleary & Gobble, 1990; Cottrell, Girvan, Seabert, Spear, & McKenzie, 2018; T. M. Davis & Hensley, 1997; Fetro, 2000; Sondag & Burns, 1998).
Recommendations for Addressing Challenge #3
Develop a national education campaign for school administrators, deans, and faculty members in schools of education, and leaders in state education agencies focusing on the unique characteristics of health education and physical education disciplines and their contributions to academic success.
Mobilize major health and education professional organizations (e.g., SOPHE, ASHA, American Public Health Association, ASCD, the National Association of Secondary School Principals, The School Super-intendents Association, National Association of State Boards of Education, National School Boards Asso-ciation) to advocate that those who teach health education in schools should be licensed/certified health teachers and have majored in the discipline to teach preK–12 health education.
Recruit additional health organizations such as the American Association of Diabetes Educators, American Cancer Society (1994), American Diabetes Association, American Heart Association, and the American Lung Association to partner in these advocacy efforts. This campaign would align with a Local Education Agency Action Step presented in the National Health Education Standards, “Ensure that health education is taught by licensed/certified health education teachers” (American Cancer Society and Joint Committee on National Health Education Standards, 2007, p. 65). The message focus would be the distinction between health education and physical education: that is, distinct national standards for instruction and for accreditation of teacher education programs, theoretical bases, instructional content and methods, and student assessment methods. Another important message in this campaign would be the relationship of healthy children to academic success, especially for disadvantaged students (Basch, 2011; Michael, Merlo, Basch, Wentzel, & Wechsler, 2015).
Challenge #4: Provide Support for Teachers to Receive Ongoing Professional Development
Changes in education, science, demographics, legislation, technology, and other facets affecting society, require that teachers pursue post-baccalaureate training and professional development to provide high-quality education. Professional development of teachers results in enhanced student learning outcomes (U.S. Department of Education, National Center for Educational Statistics, 2017). Expectations for professional development vary by state, school district, and school principal, but the federal ESSA of 2015 (which amended the Elementary and Secondary Education Act of 1965), allows states to use funds for professional development. Very few state plans, however, specify using funds for ensuring that those who teach health receive professional development (Cairn Guidance, 2018). Analyzing data from the U.S. Department of Education’s 2011-2012 Schools and Staffing Survey, Cardina (2018) found that secondary health education teachers reported less support in terms of release time from teaching, reimbursement for conference fees, or scheduled time in the contract year as compared with secondary teachers of all other subjects. Secondary health teachers also were less likely than secondary teachers of all other subjects to be provided opportunities to participate in teacher induction programs, be assigned a mentor or master teacher, or other types of support designed for beginning teachers. According to the recent CDC SHPPS study, which reported data from 2014 and 2015, only 39.6% of districts required those who teach health education to earn continuing education credits on specific health education topics or instructional strategies (CDC, 2016). However, CDC also found that since 2000 the percentage of districts that provide funding for in-service education to those who teach health education has increased in most health topic areas such as emotional and mental health and suicide prevention and for pedagogy topics such as assessment of student learning. The only topic for which more than half of districts required professional development was violence prevention, including bullying. Those topics least often required were chronic diseases, food borne illnesses, oral health, and pregnancy prevention (CDC, 2016).
Recommendations for Addressing Challenge #4
Encourage states to require that teachers complete a minimum number of professional development hours in their area(s) of content expertise for continued state teacher certification, especially those who are content specialists (vs. generalists such as elementary teachers).
Provide support for teachers to earn in-service credits through offerings from professional health education organizations (e.g., SOPHE, ASHA).
Work with national or local voluntary health organizations (e.g., heart, cancer, diabetes, lung) and with state teacher training organizations to develop in-service courses for health teachers in needed content areas (e.g., using data from student assessment to inform instruction).
Challenge #5: Develop, Fund, and Implement Research Focused on Characteristics of and Barriers to Quality School Health Education, with Specific Emphasis on the Preparation of Preservice Elementary Classroom Teachers and Secondary Health Education Specialists
Every field can benefit from new research and teacher preparation is no exception. Although research evidence exists about curriculum effectiveness, little research has addressed persistent barriers to implementation and maintenance of school health education (Birch, 2012). Since the passage of No Child Left Behind (NCLB) and subsequent heavy implementation of high-stakes testing in public schools and then the passage of the ESSA, little research regarding health education teacher preparation has been conducted (Boguslawski, 2018). For the health education profession to better influence teacher preparation programs, the hiring of well-qualified teachers of health education and abilities of teacher candidates to implement instruction that is consistent with the National Health Education Standards, the field needs new research designed to address the following questions:
What courses and experiences are essential to prepare those who teach health education?
What are the best (or effective) modes and approaches for preparing practitioners to teach health skills using active learning teaching strategies?
How effectively can elementary teacher candidates integrate health education instruction with instruction in other academic subjects such as language arts and mathematics?
To what extent do accredited teacher preparation programs provide specific courses and experiences that accepted health education teacher competencies?
What approaches have provided effective support for novice teachers’ ability to implement health education and to use effective instructional approaches for teaching health knowledge acquisition and skills?
Is there a location for the health education teacher preparation programs within academic institutions that yields better prepared health teachers (e.g., schools of education, schools of health science/public health or a collaborative arrangement)?
Does school principals’ interest in hiring teachers who are well prepared in health education affect undergraduate teacher preparation programs?
What advocacy messages and messengers are most effective at influencing preservice teacher preparation programs regarding health education?
Other considerations include who conducts and funds such research and how to effectively disseminate findings. Kolbe (2019) underscores the need for faculty and universities to pursue more cross-disciplinary collaboration in both research and professional preparation: More broadly, however, the extent to which school health programs can improve both public health and education ultimately is dependent on university programs that respectively train and credential the public health workforce, the education workforce, and each school health component workforce; simultaneously conduct related school health research and development; and provide professional service to sustain and improve school health programs within their own localities, states, nations, and internationally. Faculty who train various school health professionals usually work within one university college, focus on one school health component, and affiliate with one national professional organization. (pp. 455-456)
Teacher preparation program courses of study are determined by administrators and faculty members within schools of education who most value educational outcomes related to language arts, mathematics, and science (i.e., tested subjects) and/or who have a vested interested in requiring course work in their specialty areas (e.g., child development, pedagogical theory, communication, inclusion, technology). Since health education is typically a niche area with a very limited number of faculty members who may have academic appointments in other schools; and justification for inclusion of course work is typically based on child and adolescent health outcomes, schools of education decision makers may not support inclusion of required course work in health education pedagogy. Additionally, school health education research is typically published in health-focused (Herbert & Lohrmann, 2011) or school health–focused journals (O’Neill, Clark, & Jones, 2011), not in mainstream education journals that provide greater exposure to a broader, general education audience. Furthermore, very few new potential higher education faculty members are being prepared to specialize in school health education pedagogy and research (Clark & Olsen, 2016). For these reasons, innovative strategies are needed to illuminate decision makers in teacher education the potential contributions of quality health education to current priorities in preK–12 education such as social–emotional learning and the whole child movement. Health education should be viewed as not only an approach to improving and maintaining students’ current and future health but also as a strategy for supporting students for academic success.
Recommendations for Addressing Challenge #5
Encourage health education researchers to partner with investigators who have expertise in pedagogy, education leadership, and teacher preparation.
Present research findings at conferences attended by, or in journals read by, more generic teacher education and higher education faculty members.
Seek a funder such as a for-profit entity or philanthropic foundation that will support multi-year research studies and thus provide the sustained effort needed for yielding actionable research findings.
Conclusions
Few disagree with the importance of school-age children acquiring the knowledge and developing skills they need to maintain and improve their health. As a component of the WSCC framework, health education plays a key role in promoting not only student health but also academic success and enhances students’ prospects as adults to lead healthier, wealthier, and longer lives (Bradley & Greene, 2013; Kolbe, 2019; Michael et al., 2015). Through Healthy People 2020 (ODPHP, 2016, 2019), the public health sector has recognized the contribution education makes to improved health. Healthy People 2020 includes objectives for expanding preK–12 health education for students and increasing the proportion of instruction that addresses knowledge and skills emanating from the National Health Education Standards. These aspirations will only be reached with quality professional preparation and ongoing professional development for individuals responsible for teaching health education.
Public health educators not only work with schools in topic-specific or grade-specific health education programs but are also key WSCC stakeholders. This work presents the opportunity for advocacy efforts with school decision makers for quality, comprehensive school health education taught by teachers with appropriate professional preparation, and certification in health education. Promoting health education as a component of WSCC can be an important message within these advocacy efforts (SOPHE, 2019). Beyond advocacy focused on preK–12 schools, public health educators also can examine the individual certification and professional preparation requirements in their states and, if necessary, advocate for more rigorous professional preparation, and stronger certification and program accreditation requirements. Recently, there has been increased recognition by public health professionals of the linkage between education attainment and adult health outcomes (Allensworth, 2011; Cohen & Syme, 2013; Hahn & Truman, 2015; Kolbe, 2019; Ruglis & Freudenberg, 2010). The WSCC model presents opportunities for national education and health organizations and public health educators to be engaged more strategically with schools in efforts to promote education and health. Last, faculty members in public health education professional preparation programs can educate their students about school health education; their role as partners in implementing the WSCC framework; and their responsibilities as future advocates for quality school health education and rigorous professional preparation and certification/accreditation standards.
Footnotes
Authors’ Note:
This article is part of a special School Health Collection developed under the guidance of the Society for Public Health Education (SOPHE). SOPHE received funding from the CDC School Health Branch in the National Center for Chronic Disease Prevention and Health Promotion (Grant number 6 NU38OT000315-01-01) to support printing and open access dissemination. No federal funds were used in the development of these manuscripts and the views and findings expressed in them are those of the authors and are not meant to imply endorsement or reflect the views and policies of the U.S. Government.