
Abstract
Recent attention to issues of systemic and institutional racism have resulted in renewed calls for antiracist teaching and learning in the health sciences. Concurrently, there is an emerging socio-political mobilization to pass legislation that limits the teaching of systemic racism. We argue that teaching and learning about racism in academic health professional curricula often has serious limitations—stagnating in a place of teaching about the social and structural determinants of health, yet emphasizing health education and individual behavioral interventions as solutions to health inequities. We present a framework that explains essential components of antiracist knowledge and action that we argue must be implemented across health sciences curricula. Using this framework, we call on health sciences educators to examine how learners engage with racism as a determinant of health and to make curricular changes that provide opportunities to learn about and engage with antiracist actions.
Introduction
The call to differentiate between race and racism as determinants of health is not new in the health sciences (Braveman & Parker Dominguez, 2021; Came & Griffith, 2018; Ford & Airhihenbuwa, 2010; LaVeist, 1996). However, increased national attention to issues of systemic and institutional racism have resulted in renewed calls for antiracist teaching and learning in higher education, specifically in the health sciences (Burnett et al., 2020; Choo, 2020; Coleman, 2020; Wandschneider et al., 2020). While much has been written about the need for antiracist education, there are few published examples of programmatic or curricular change (Afolabi et al., 2021; Hagopian et al., 2018). For instance, research suggests that the implementation of antiracist pedagogy in health professional education must include: dialog across social groups (ongoing student group conversations to foster cooperative learning), deconstructing power and privilege, student transformation, and application to practice (identify the role of students, educators, institutions and communities); however, it is unclear what are the antiracist curricular building blocks to be implemented in the practice of antiracist pedagogical approaches (Diffey & Mignone, 2017). At the same time, there is an emerging movement in the United States to limit teaching about systemic and institutional racism—with multiple states (Arizona, Florida, Idaho, Iowa, New Hampshire, Oklahoma, Tennessee, and Utah) passing legislation to limit curricular content related to racism in public schools (Abramsky, 2022; Gibbons, 2021).
Antiracist teaching is critical to students’ well-being, but also necessary for the formation of health professionals who are responsive to the needs of communities and equipped with the critical analysis skills to question how institutional racism is perpetuated in health systems. While there is an emphasis in many health professions curricula to include culturally sensitive training, there is not only an under-representation of Black, Indigenous, and other students of color within professional health programs, but also a lack of representation of faculty of color limiting student access to supportive mentorship, and a positive educational and training experience (Wilbur et al., 2020). To not include antiracist teaching across health sciences curricula represents a disservice to the lived experiences of students, and the communities they belong to; therefore, curricular changes to engage antiracist epistemological frameworks are fundamental to examine the connection between racism and health outcomes.
We believe that teaching and learning about racism in the health professions often has serious limitations across the curriculum. While social determinants of health may be introduced to students, in-depth examinations about social and structural determinants of health, especially racism, relevant theories, and the positionalities of learners and their teachers are missing (Tsai et al., 2021). Instead, we argue that there is an over-reliance on health education and individual behavioral interventions as solutions to health inequities, which can result in a deficit mindset about individuals, communities, and populations (Westbrook & Harvey, 2023).
Health systems (e.g., medicine and public health) have a long and well documented history of racism in the U.S., with healthy bodies being defined within western dominant scholarship in terms of purity, whiteness, class, and cleanliness—contributing to the dehumanization of people based on race, gender, sexuality, class, and ability (Bashford, 2003; Berthold, 2010). According to theorist and abolitionist, rks that help eHarrison (2021) historical health conceptualizations have depended on the idea that “for race to be constructed, the Slave had to exist—and had to exist as the antithesis of health—so that European physicians, anthropologists and other eugenicists could determine what set the Slave apart from the Caucasian” (p. 34). In our own professional experiences, we continue to witness how clinical, research, and public health professionals conceptualize the connection between race, health, and disease based on pathologized racial differentiations. The ongoing practice of attributing risk factors based on “inert” and “biological” racial differences has resulted in violent and racist clinical and public health interventions such as the underfunding of HIV care in the 1980s or the health and economic impacts of “public safety” measures such as mass incarceration among racialized communities (Fleming, 2020; Malawa et al., 2021). The response to (or lack of) care within racialized communities during the COVID-19 pandemic is an undeniable example of structural violence driven by institutional racism in U.S. systems of health and public service. For instance, at the beginning of the pandemic, Black, Latinx, Indigenous, and Asian communities experienced disproportionate infection, transmission, hospitalization, and mortality rates, while tacitly being expected to risk their lives in low wage service jobs to ensure the survival and comfort of others, and thrive in a pandemic under conditions of inequity in housing, employment, education and health care (Aleligne et al., 2021; Lopez et al., 2021; Smith, 2020).
In this paper, we discuss how traditional health sciences programs may perpetuate racial stereotypes and inadequately prepare students to dismantle racism. Our recommendations are based on our training, learning, teaching, and personal lived experiences in health professions such as nutrition and dietetics, nursing, medicine, occupational therapy, public health, and health equity research. We have chosen to focus on health sciences curricula broadly because being prepared for action against racism is relevant to all health professions. There is evidence of structural racism across disciplines and settings (Hamed et al., 2022; Sim et al., 2021). We believe that the lack of commitment and capacity to create and implement an institutional plan that formalizes an antiracist curricular change across health sciences programs will continue to sustain harmful examinations of race and health, and therefore, the potential for future health professionals to engage in violent practices in the direct service of communities. One first step, however, to antiracist teaching is for researchers, practitioners, educators, and leadership to unravel and reject potential racist scholarship informing health sciences curricula that can contribute to the formation of ill-equipped health professionals.
Then, we present and recommend a framework of antiracist curricular change for university health sciences educators to engage with racism as a determinant of health and to create curricular content that fosters critical thinking and advocacy among students. Finally, we provide ideas for course activities and potential learning outcomes across the framework.
Process and Positionality
This paper emerged from the ongoing mutual reflections between a public health master’s student and a health sciences professor at Northern Arizona University (NAU) about the limitations of learning and teaching about health equity and institutional racism in the classroom. The exchange of knowledge, feelings, and frustrations between the graduate student and her professor prompted the collaboration with other academic professionals to brainstorm a framework for antiracist curriculum development. The writing process of this paper required open and transparent conversations about positionality and power difference given the multiplicity of lived experiences among the authors.
This collaboration required the acknowledgment of our positionalities, the allowing for multiple and different kinds of expertise, and the relinquishment of traditional power dynamics. Black feminist theorist, Bell Hooks argues that teachers require courage to transgress the boundaries of learning, approach students with a desire to respond to their unique beings, and ultimately see the classroom as a space of collective critical awareness and active participation—requiring the mutual labor of both teachers and students (Hooks, 1994).
The ongoing exchange of knowledge that took place in the completion of this paper is evidence of the value in dismantling the boundaries of learning between teachers and students. Given the co-authorship of this paper, it is crucial to honor the positionalities that permeate each author’s conceptualization of and proximity to issues of health equity and racial justice. Each author’s writing was informed by our lived experience, collaborative dialog, and a review of literature about antiracist curriculum in the health sciences. We believe that our intersectional identities helped us imagine what an antiracist curricular change can look like and therefore, delineate each of the antiracist components presented. We intent to share our experience of participatory collaboration in hopes to provide an example for other health sciences educators and students to engage in, and identify opportunities for curricular change within their own health professional programs. An extended statement of each author’s positionality and lived experience is in Supplemental Appendix A.
Theoretical Frameworks
The proposed antiracist framework for curricular change is informed by theoretical models and pedagogical epistemologies such as: Critical Race Theory (Crenshaw, 2010), centering the margins (Hooks, 1994), and problem posing education (Freire et al., 2014). We wanted to prioritize the exposure of students to concepts that problematize the categorization of race and ethnicity as biological traits, essential risk factors and therefore as indicators for health disparities. Crenshaw’s work, creates a clear definition of race as a social construct and positions race within a system of institutional power (Crenshaw, 2010). Given the active collaboration of authors in the design of each of the antiracist components of curricular change, the pedagogical and epistemological work of Bell Hooks was critical to create a framework that gave educators and students the flexibility and freedom to center non-dominant narratives of health. This framework is intended to create a classroom that focuses attention on “the margins” and engages students in active “de-marginalization”—the inclusion of experiential and cultural knowledge from students and local communities in curricular material as viable, legitimate, and creative foundations to social change to address health inequities (Hooks, 1994, p. 64).
Finally, Freire’s “problem-posing education” approach represents a pedagogical method that invites learners to encounter an issue as fully formed persons, albeit persons who can become more agential (Freire et al., 2014). In other words, problem-posing education empowers learners to see themselves as active advocacy agents for change, and reflect about how they can affect challenging situations such as racism in healthcare. For this reason, we see an antiracist framework for curricular change as having a focus on advocacy, so that students are familiar with the knowledge and tools necessary to create tangible and reliable health equity solutions.
The Racial Health Disparities and Health Deficit Loop
Figure 1 depicts a model of how health sciences curricula often engage and teach content related to race and racism, based on our diverse and multiple experiences. In this model, students are presented repeatedly with statistics and narratives that highlight racial health disparities—reinforcing the myth that racialized communities are unhealthy because of individual behavior choices, genetics, and/or cultural factors. These narratives misrepresent, omit, or gloss over constructive discussions regarding the root causes of the disparities (Amutah et al., 2021). Instead, disparities are often incorrectly attributed to genetic racial variation, culture, or individual choice(s). Additionally, due to curricular constraints and a potential lack of knowledge among faculty, lessons related to racial health disparities are disjointed, intellectually shallow, and low stakes (Chandler et al., 2022).
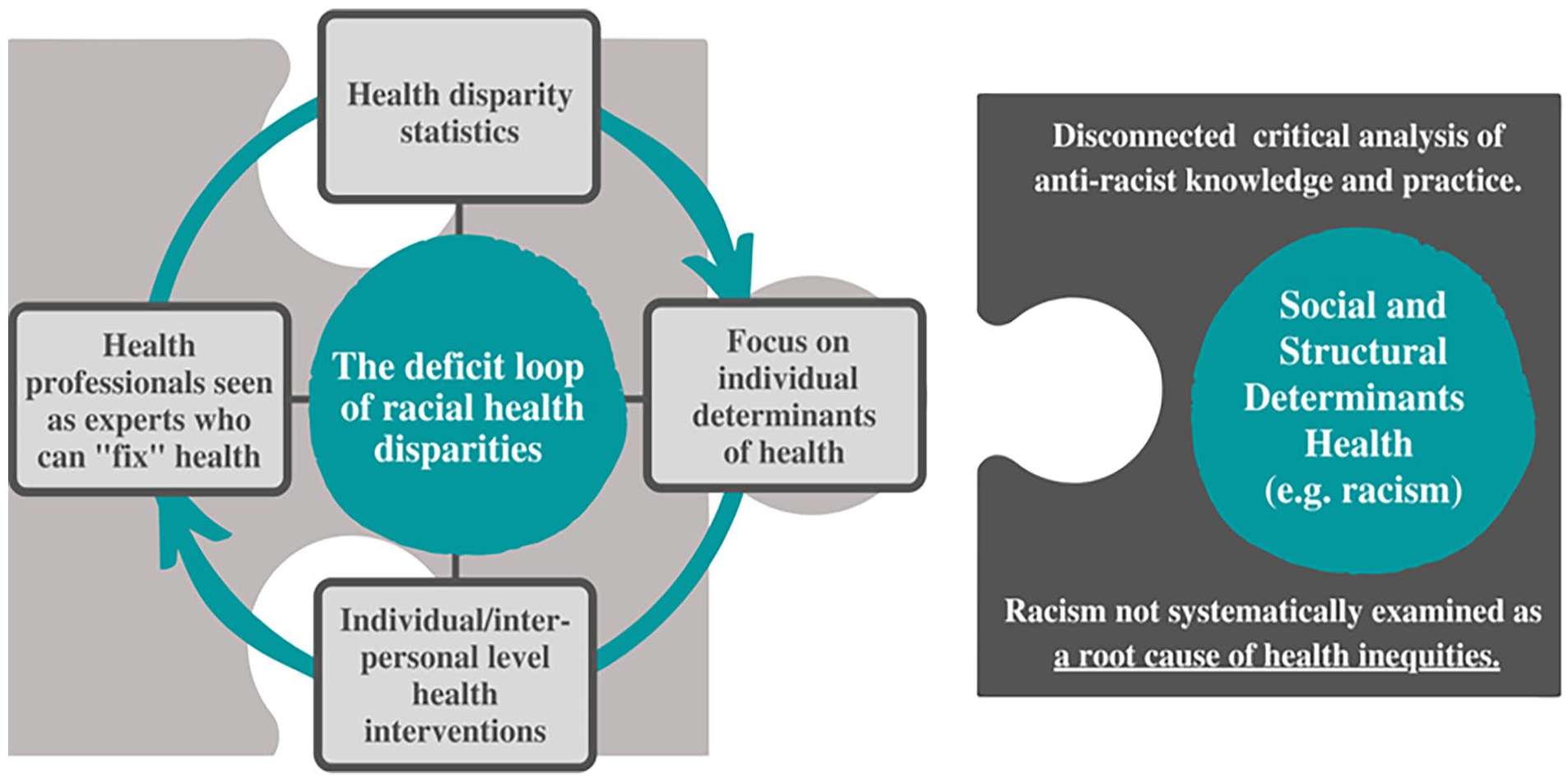
The racial health disparities and health deficit loop in health sciences pedagogy.
While social and structural determinants of health, including racism and discrimination, may be part of the curriculum they are rarely systematically examined as a root cause of health inequities and students are not given an opportunity to engage with interventions that address racism to promote health equity (Chandler et al., 2022).
In the cycle depicted in Figure 1, students are tasked with designing individual interventions to fix disparities. For example, a course may examine differential rates of diabetes among Indigenous and white populations in the U.S. and even possibly include a discussion of historical and present-day trauma, colonialism, forced removal, and racism. However, when asked about strategies to reduce the prevalence of diabetes, students will suggest and prioritize health education interventions that teach individuals to eat healthier foods and engage in more physical activity, instead of interventions which address the social and structural determinants of diabetes (e.g., poverty, transportation, infrastructure). The instructor will not take the opportunity to redirect learners toward solutions that are sustainable for communities experiencing inequity or target structural level interventions.
Teaching that reinforces individual responsibility for health perpetuates a deficit narrative of health. Making health disparities the central story in teaching about health outcomes and race risks the construction of racialized communities as lacking health and/or the ability to be healthy—an approach which hyper-focuses on community deficit instead of community assets or strengths. When students are led to believe that individual and interpersonal-level interventions are the primary mechanisms to eliminate health inequities—they have missed an opportunity to question how structural racism impacts health, and create structural level solutions to eliminate racist policies and institutional practices harmful to the well-being of racialized communities.
A Framework of Antiracist Knowledge and Action for the Health Sciences
The antiracist framework in Figure 2 includes four components necessary to antiracist health education. The four components are: (1) defining and contextualizing race and racism, (2) shifting the focus from health disparities to health equity, (3) integrating the contributions of social, cultural, and critical theories, and (4) engaging in advocacy and action for social change.
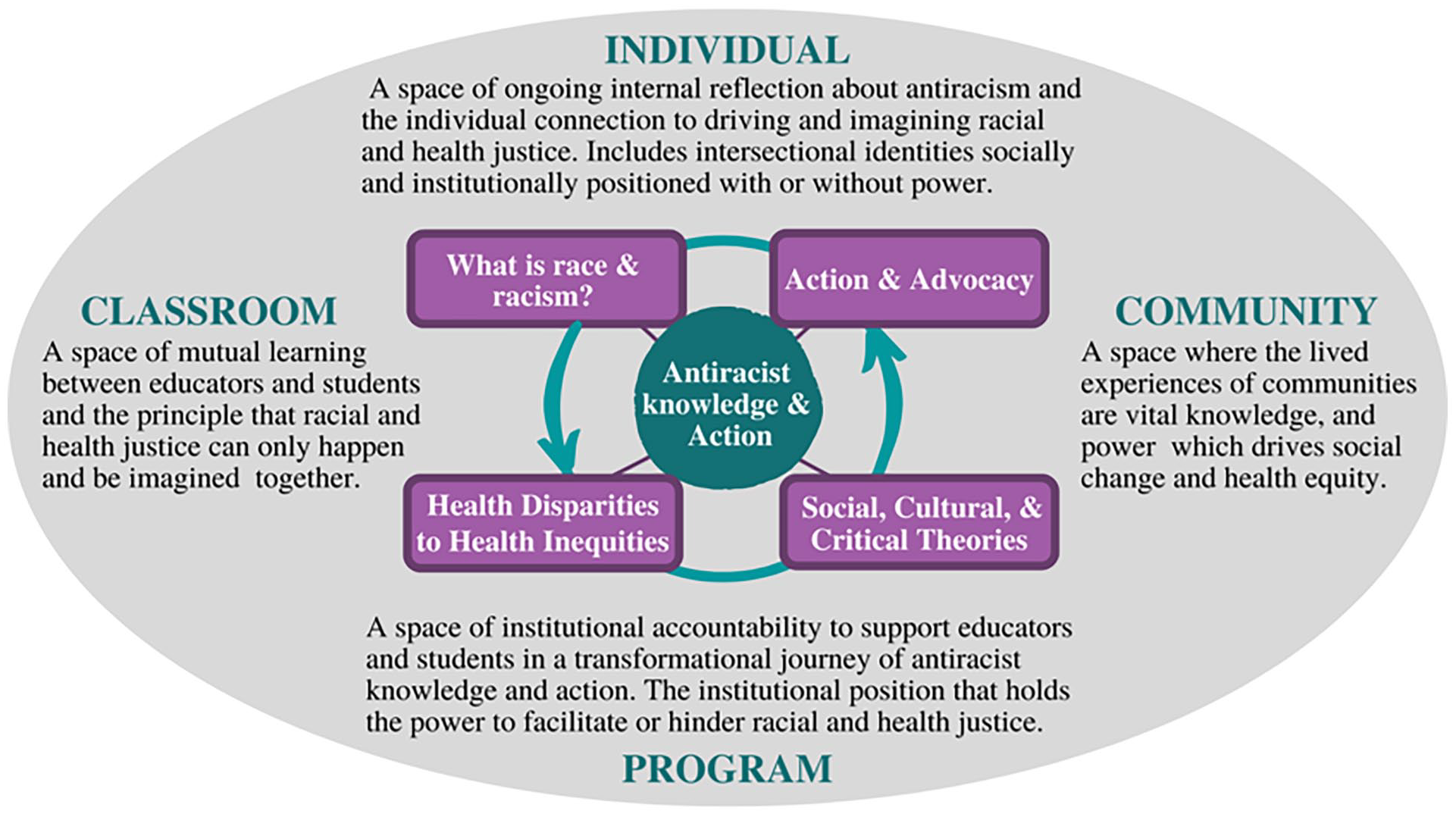
A framework of antiracist knowledge and action for health sciences programs.
We posit that these components are embedded within different levels of positionality that represent spaces of power and impact (Figure 2). Therefore, when examining how the components are taught across the curriculum, it is important to consider teaching in the context of the classroom, program, community, and individual. We ask educators to cognize the classroom as a space not independent from active systems of power and inequity, but a place where a multiplicity of positionalities and power differences exist and are actively impacted by institutional racism. Therefore, we encourage teachers and students to fearlessly engage in collaborative reflections about the positionalities in the classroom and the systems of inequity impacting the learning experiences of students.
Component #1: What is Race and Racism?
To analyze how racism is a determinant of health, students need foundational knowledge that covers (1) how race is socially constructed in the health sciences, (2) how race functions as a power structure, and (3) how racism operates as a modality of structural violence to protect and sustain institutionalized white supremacy in the health professions and beyond.
Race is a Social Construct
Race as a social construct represents a social, political, and institutional process that creates racial categories to determine who has access to resources, social, institutional, and political power. While it is well documented that race is a social construct, health professionals and health care systems continue to construct race as a biological trait. To categorize race and ethnicity as biological characteristics reinforces the notion of race as an inherent risk factor for poor health outcomes (an example of racial essentialism) and ignores the social and structural determinants of health (SDoH) (Braun & Saunders, 2017; Nuriddin et al., 2020).
In the health sciences, racial essentialism fosters a narrative of health hegemony, which describes how “healthy” bodies must biologically and physiologically function, behave, and appear (e.g., skin color, hair texture, body shape). A health hegemony depends on the pathologized differentiation between who is healthy or diseased, safe or unsafe, clean or dirty and even infected or immune, which poses the risk to describe people as the “other” or non-human (Bashford, 2003). The state management of reproductive health among women of color in the U.S. is an example of how the construction of Black and Brown bodies as non-human, at the intersection of gender and sexuality, has driven the design and implementation of inequitable health interventions. While there are many examples, in 2020, reports of forced sterilization among Mexican and Central American immigrant women came to light after several non-consensual hysterectomies were performed by medical providers at Irwin County Detention Center in Georgia (Lenzer, 2020). This is a prime example of how racial essentialism socially constructs women of color as hypersexual, unfit to parent, and/or part of a population that needs to be managed and controlled rather than deserving of care (Nuriddin et al., 2020; Roberts, 1997; Sankaran, 2020).
Race is a Power Structure
Once learners analyze race as a social construct, they can interrogate how race is used to systematically oppress and harm groups of people. To do this, we must teach how race functions as a power structure. We propose teaching about race as a categorical structural power that conceptualizes, (1) institutional racism as a structure of violence harmful to health and (2) institutional racism as a modality enforced by white supremacy.
We encourage educators to teach about institutional racism as a mode of structural violence producing harmful living conditions that can lead to poor health outcomes and quality of life among racialized communities. Dr. Camara Phyllis Jones (2000) explains that institutional racism manifests in material conditions (quality housing, gainful employment, appropriate medical facilities, and clean environment), and access to power (access to information, resources, and voice). Institutional racism functions through the production of policies and practices that sustain racial power difference. As a system of structural violence, institutional racism causes lingering harm and injury (e.g., trauma, chronic disease, physical neglect, or assault) that creates poor health outcomes among racialized communities that experience inequity (Marya, 2021; Nuriddin et al., 2020; Roberts, 1997).
To see race as a power structure requires the unveiling of white supremacy institutionally (public service, medical, or public health), and recognize that race is not just an abstract, inconsequential way to categorize individuals, but it is also about power differences that produce undesirable health outcomes. The Black feminist scholar, Smith (2020), explains how institutionalized white supremacy creates a “universal operating system that relies on entrenched patterns and practices to consistently disadvantage people of color and privilege whites.” Therefore, an antiracist curriculum must include education that exposes students to examine how white supremacy informs the institutions (e.g., education, health care, transportation, housing) that directly impact the lives of historically disenfranchised communities. An antiracist framework in the health sciences requires the eradication of white supremacy.
Component #2: Shifting From Health Disparities to Health Inequities
The second component of the framework distinguishes between health disparities and health inequities when examining differences in health outcomes. By training health professionals to critically analyze differences in health through an equity lens, we can create a culture in which we learn about differences in health behaviors and health outcomes in their larger social and structural contexts, including racism. Medical and public health interventions that attempt to advance health equity from a health disparities approach pose the risk of creating a narrative of racial essentialism.
The term health disparities describes population-specific differences in health outcomes, while health equity refers to the provision of the conditions needed to ensure optimal health for everyone (Jones, 2000). Differences in health outcomes are often presented by indicators such as gender, race, ethnicity, age, and/or socioeconomic status, but omit underlying assumptions about the root causes of disease and exclude explanatory or contextual information about health inequities. Teaching health professions to distinguish between health disparities and outcomes that are unfair, changeable, and rooted in inequitable systems (health inequities) is essential. Doing this helps break the cycle described in Figure 1—where individual and interpersonal solutions are suggested repeatedly to tackle health inequities. Instead, educators can guide students to identify and interrogate the conditions that allow differences in health outcomes to exist. The antiracist framework represents an opportunity for professionals to step away from the over-reliance on personal responsibility and individual blame embedded in the intervention design process.
Component #3: Contributions of Social, Cultural, and Critical Theories
Education and training of future health sciences professionals do not operate in isolation from other systems of knowledge and power. They are interdependent with political and social modes of knowledge production and must be contextualized as such in antiracist education. The third component of the framework highlights the need for interdisciplinary scholarship that includes formation in community grounded knowledge, humanities, and the social sciences and also considers the intersectional implications of antiracist knowledge and practice. We argue for integrating interdisciplinary concepts across multiple courses to train future health professionals to critically examine the relationships between power and knowledge. Examples of frameworks that help elucidate relationships between racism and health include (but are not limited to): biopower, marginalization, critical race theory, and experiential knowledge (see Table 1). In addition, we believe the feminist work of queer and women of color such as Lorde (2011), Bell Hooks (2015), Anzaldúa (2012), and Moraga and Anzaldúa (2015) among others, can inform a health sciences curriculum that honors the power of communities’ stories, capacity and agency to thrive under conditions of inequity—experiential knowledge that must inform the design and implementation of health approaches and interventions.
Supplemental Materials and Texts on the Contributions of Social, Cultural, and Critical Theories.
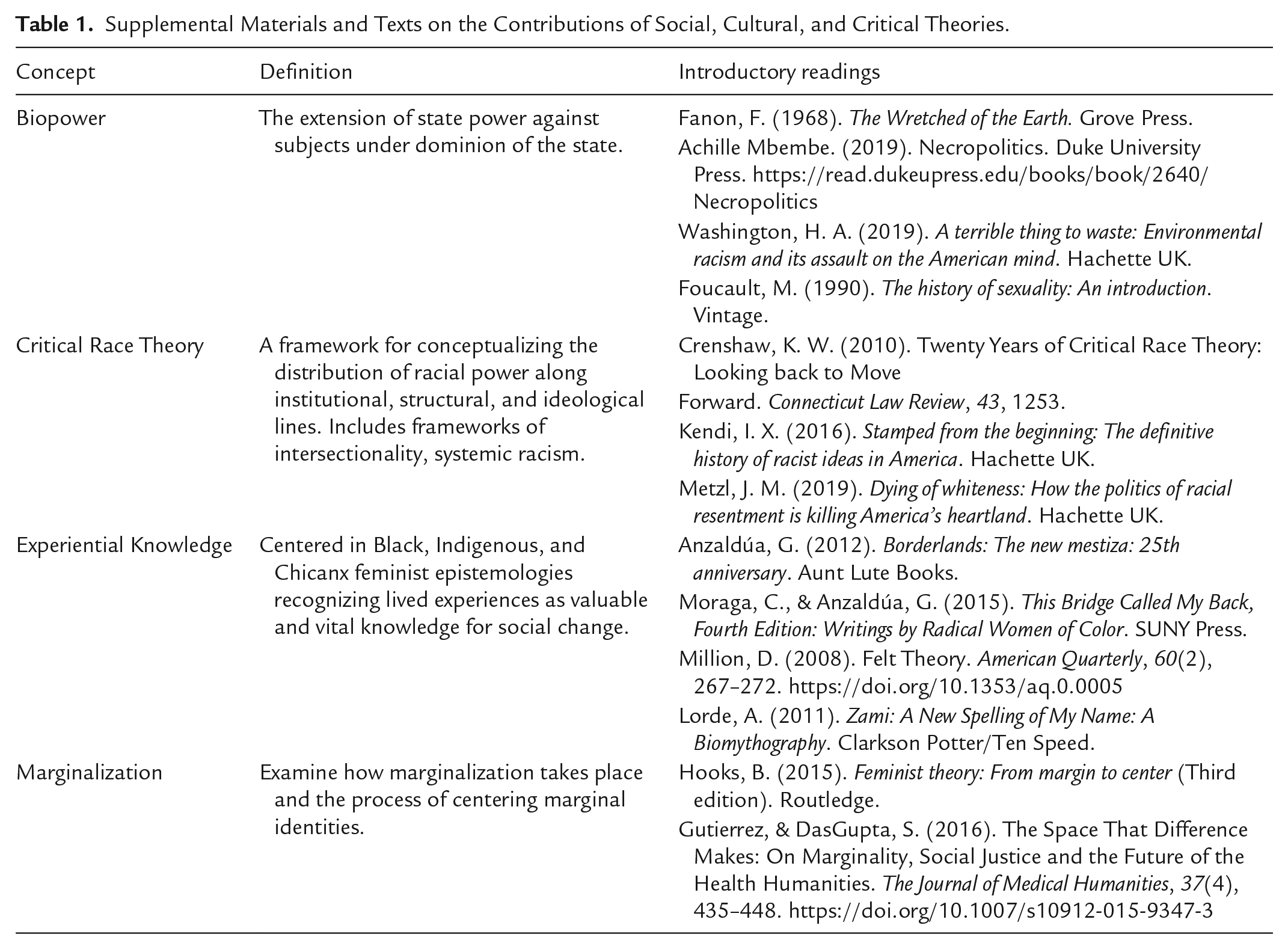
To encourage a comprehensive and grounded knowledge base of structural racism, health science educators can embed these and other critical texts into required and elective coursework. This may also require including interdisciplinary courses that teach these frameworks as part of the curriculum and/or the co-development of interdisciplinary coursework, with an emphasis on incorporating the knowledge and experiences of local and diverse communities. Health professionals who engage interdisciplinary frameworks will be better prepared to identify and challenge instances of structural racism in health systems.
Component #4: Action and Advocacy for Social Change
The final component of the model acknowledges the importance of activities that provide an opportunity for learning, observing, and engaging in actions and advocacy that address racism as a root cause of health injustice. All health professionals should assess both why and how to advocate for programs and policies which address the root causes of health injustice, regardless of their level of practice (individual, family, and/or community health).
To prepare health professionals for action related to the root causes of poor health, including racism, educational programs must provide examples of and opportunities to engage in advocacy. These opportunities should center individuals and populations impacted by health inequity and injustice. In other words, students should not be given assignments that ask them to propose how to solve health inequities without first learning from historical efforts of community-driven actions to address social and structural determinants of health. Learners can engage in activities to better examine how communities organize and create solutions according to their specific needs and realities, while at the same time being critical of evidence that may be biased or ignores social and structural determinants of health. Opportunities to learn from community advocacy efforts to address the root causes of poor health will help health professionals shift from narratives of individual and community deficit to narratives that highlight collective community assets and power.
To practice effective advocacy, learners should have already engaged with the other constructs of this model, including reflecting on individual and institutional positionality, and analyze how the health professions have historically perpetuated and continue to contribute to systemic racism and health injustice. Action and advocacy for students can include many forms, but instructors need to be mindful of the knowledge, skills, and abilities of learners. One strategy for educators is to learn more about the skills and lived experiences of students before planning advocacy opportunities. Critical service learning may also be a useful approach to train and prepare students for advocacy (Derreth et al., 2021). We recommend that programs review and then create or modify their curricula to develop multiple intentional opportunities for students to learn about and engage in actions that address institutional racism.
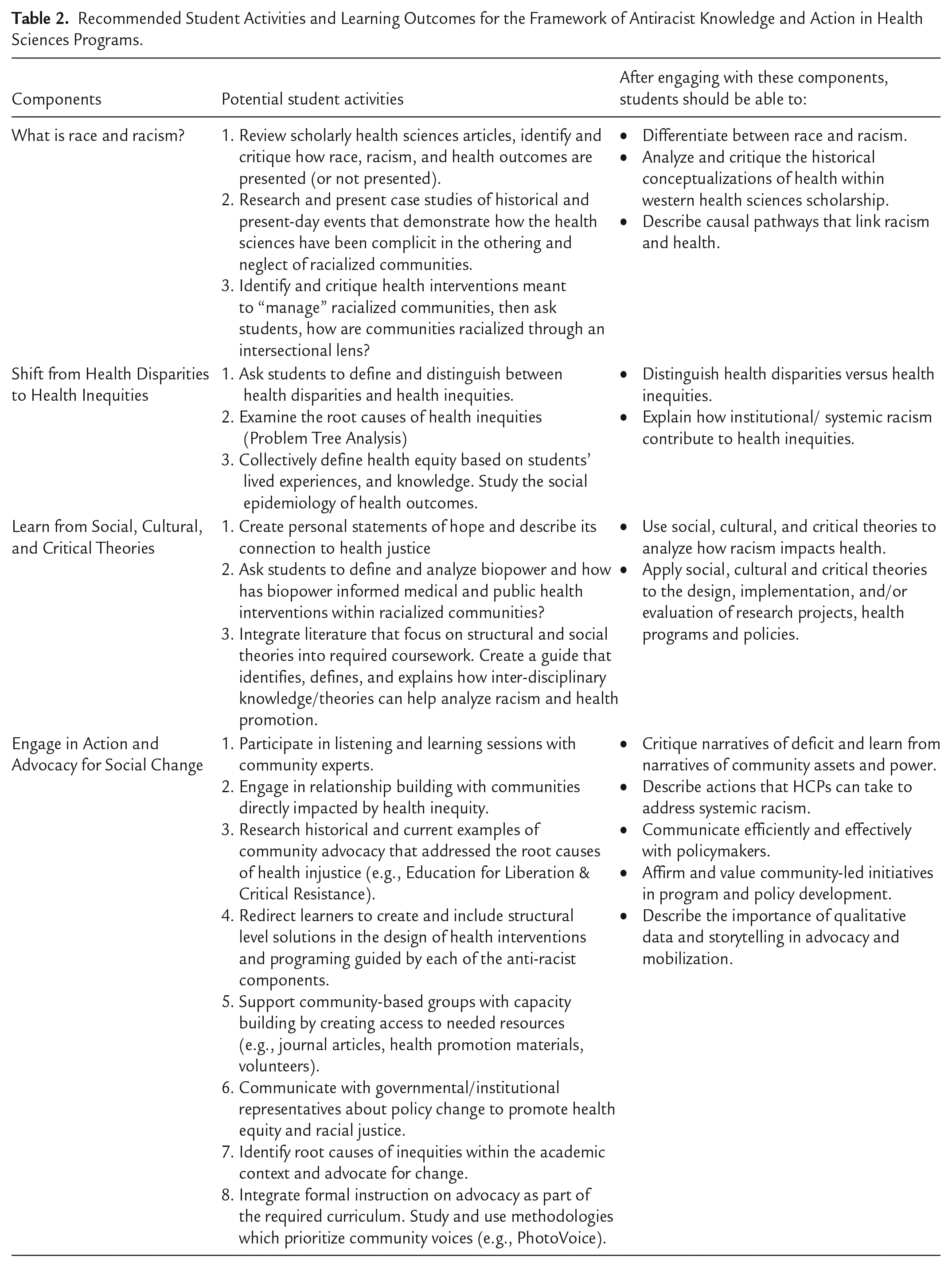
To accompany the antiracist framework, Table 2 provides specific examples of activities and learning objectives related to the four components of the framework. These activities and objectives were created collaboratively by the authors based on our experiences as teachers and students and our engagement with materials about antiracism. The examples in Table 2 are a starting point, to spark additional ideas and adaptations. Programs should consider their communities before adapting activities and learning objectives to ensure they are suited to a particular context.
Recommended Student Activities and Learning Outcomes for the Framework of Antiracist Knowledge and Action in Health Sciences Programs.
Discussion
Racism is an important social and structural determinant of health and special attention to teach and work against racism should be integrated into health sciences curricula. The reliance, comfort, and compliance in using health disparities to learn about health and disease outcomes within racialized communities leads to an uncritical analysis of how structural racism informs health and health systems. This framework urges educators to include content across the curriculum which unpacks racism as a violent power structure that has created conceptualizations of health and interventions harmful to the well-being of racialized communities.
This proposed framework is an attempt to encourage health sciences educators to practice intentional accountability in curriculum design and implementation. Intentional accountability can be an ongoing exercise of reflection and action where educators and students assess how positionality plays a role in the creation of health interventions, identify differences in institutional power, and create tangible plans to address present and/or emerging health inequities. To be intentionally accountable means to be an active participant in antiracist teaching and learning, and create an exchange of experiences and knowledge that fosters an equitable distribution of labor among students, faculty and staff. In our own experiences, we have learned that racialized faculty, staff, and students tend to be relied on as sources of antiracist educational labor. On the other hand, white faculty and staff fall into a tendency of acknowledging their whiteness in a performative checklist manner, letting others “do the work” and taking a step back (characterizing themselves as “non-experts”), all of which take a passive role in the embrace of an antiracist curriculum. It is the responsibility of educators and students to recognize that health sciences programs exist within a system of white supremacy that can produce institutional racist practices harming the learning and teaching experiences of everyone involved.
Table 3 presents examples of specific actions and potential activities necessary to move this framework forward.
Activities and Actions for Antiracist Curriculum Development in the Health Sciences.
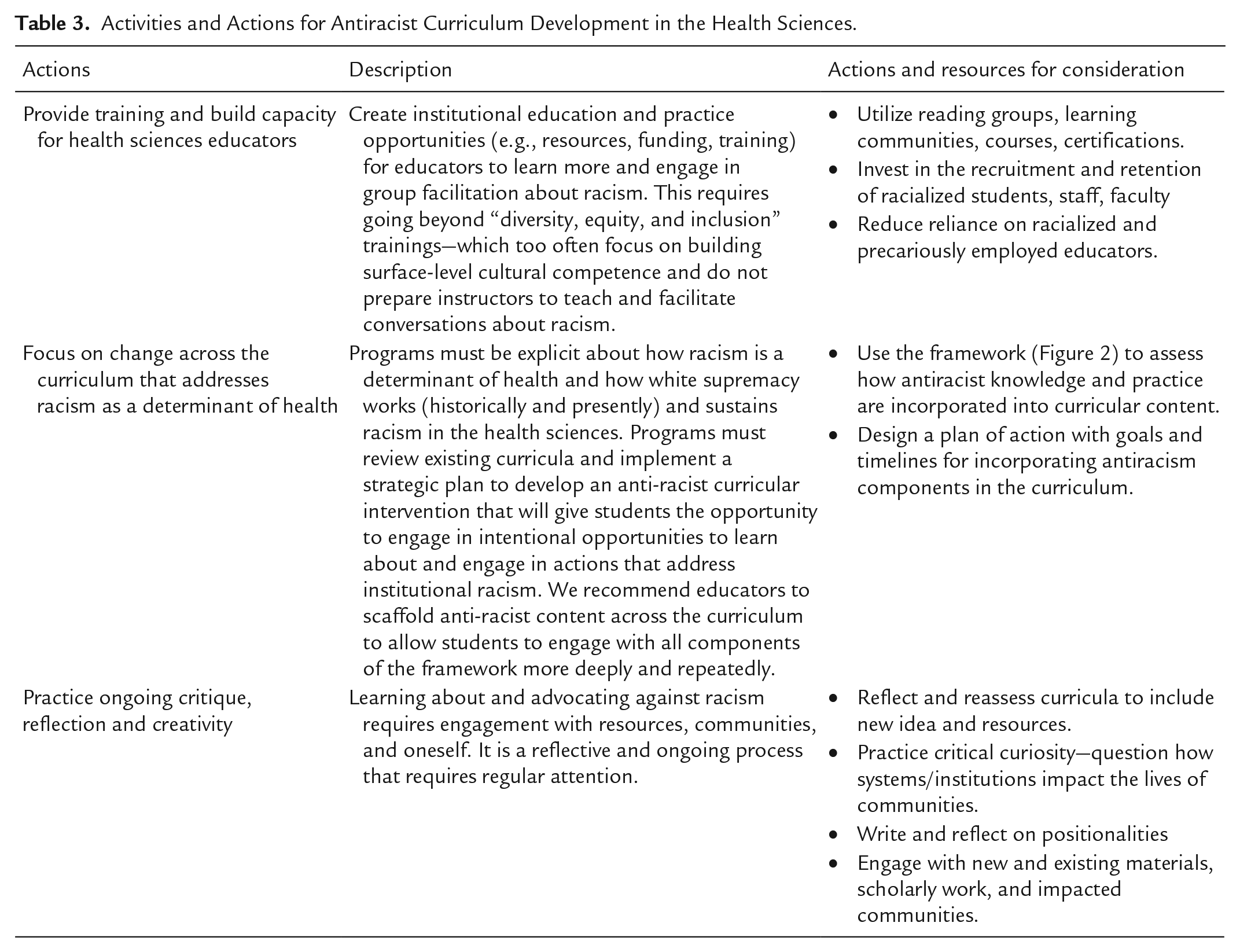
A framework for antiracist knowledge and action requires, as Bell Hooks proposes, the courage to transgress the boundaries of knowledge, the engagement of interdisciplinary scholarship, and the affirmation of grassroots organizing strategies as viable systems of racial and health justice (Blackstock & Blackstock, 2021; Hooks, 1994). Educators can use the framework and the four components as a starting point to plan and modify courses and curricula, with the goal of better preparing future health professionals to address the link between racism and health. The renunciation of a health disparities approach to teach about disease within disenfranchised communities provides an opportunity for collaborative learning about racial and structural violence and what health equity is and can be. An emphasis on health equity means putting a priority on action; the participatory will of educators and students to recognize that health equity and racial justice can have different meanings and visions for different communities.
Supplemental Material
sj-docx-1-php-10.1177_23733799231180614 – Supplemental material for Rejecting a Narrative of Individual Deficit: A Model for Developing Antiracist Curriculum in the Health Sciences
Supplemental material, sj-docx-1-php-10.1177_23733799231180614 for Rejecting a Narrative of Individual Deficit: A Model for Developing Antiracist Curriculum in the Health Sciences by Alexandra Elvira Samarron Longorio, Sara J Shuman, Catherine Lockmiller and Candace Robertson-James in Pedagogy in Health Promotion
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.