
Abstract

Health equity is the state in which everyone has a fair and just opportunity to attain their highest level of health, and no one is disadvantaged from achieving this potential because of social position or other socially determined circumstances. 1 Science is a cornerstone of public health and central to efforts to achieve health equity. Science designed to generate knowledge to advance equity can improve population health and promote health for all members of society. 2 In contrast, science and interventions not designed and implemented with equity in mind may inadvertently perpetuate or widen disparities, even while fostering overall improvements in population health. 3
Health equity science provides a conceptual framework for scientific endeavors that are designed and conducted to advance health equity. 4 Health equity science investigates patterns and underlying contributors to health inequities and builds an evidence base that can guide action across the domains of the public health program, surveillance, policy, communication, and scientific inquiry to move toward eliminating, rather than simply documenting, inequities.
Building on extensive work in developing the importance and application of equity concepts in public health practice,5-7 we describe an equity-focused scientific framework and set of principles to guide public health efforts to fulfill the health equity mission of the Centers for Disease Control and Prevention (CDC). 8
Principles of Health Equity Science
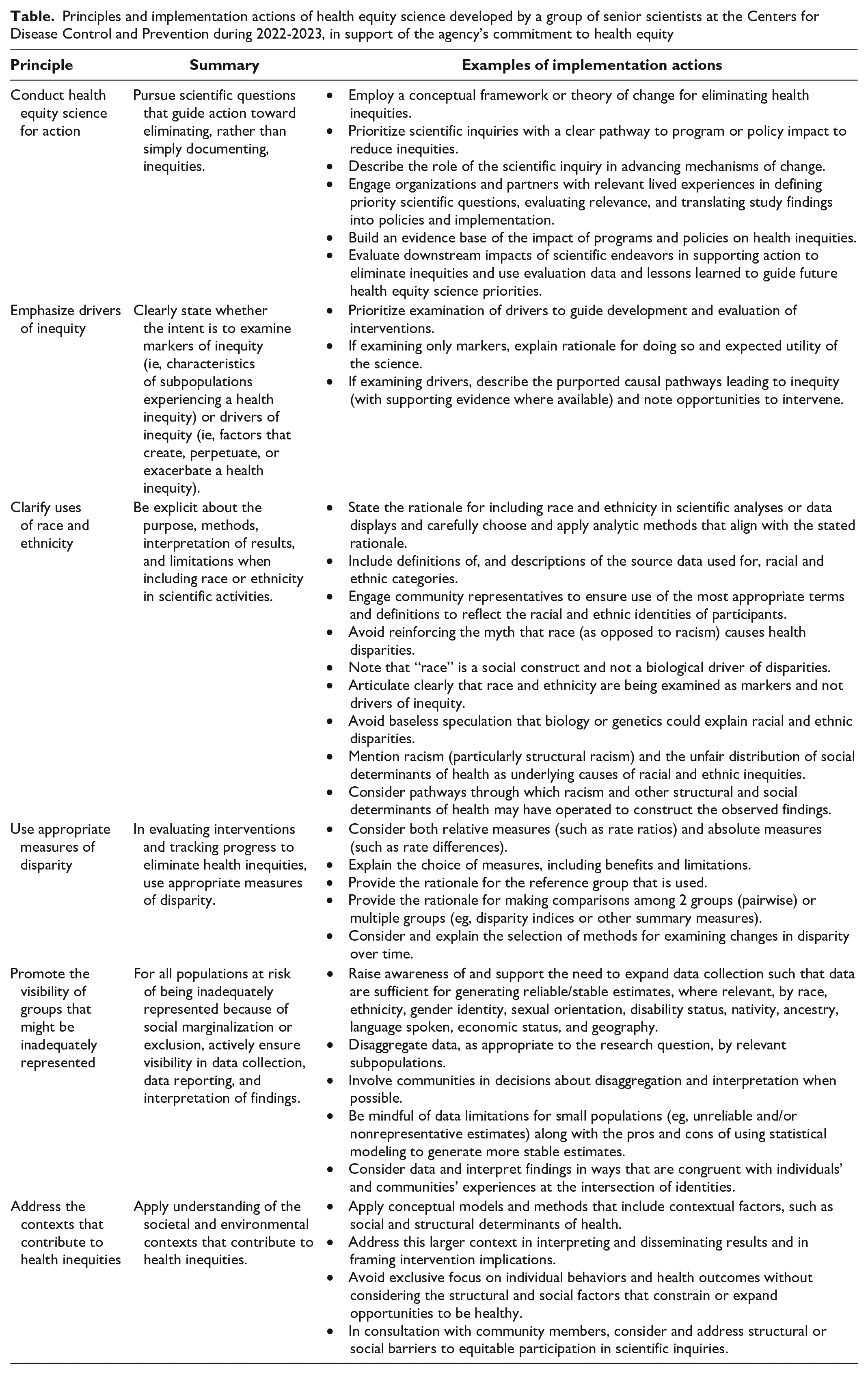
Based on the recommendations in a report by the Commission on the Social Determinants of Health of the World Health Organizaton, 9 we describe 6 high-level principles to guide the development, implementation, dissemination, and use of effective health equity science (Table). These principles were developed by a group of senior scientists at CDC in support of the agency’s commitment to health equity 8 and can be applied by the broader public health scientific community to foster equity. In particular, as the nation works to fortify the public health infrastructure, these principles could provide a guiding framework to help shape public health priorities at local, state, and national levels in support of health equity.
Principles and implementation actions of health equity science developed by a group of senior scientists at the Centers for Disease Control and Prevention during 2022-2023, in support of the agency’s commitment to health equity
Conduct Health Equity Science for Action
Health equity science can guide transformative change that enables progress toward the elimination of health inequities. Elimination, as defined traditionally in public health, is the maximal reduction of “the incidence of a specific disease in a defined geographical area as a result of deliberate efforts; continued measures to prevent reestablishment are required.” 10 Public health programs pursuing disease elimination have succeeded by setting a clear goal and implementing data-driven plans and evidence-based interventions that lead to sustained improvements in a specific outcome.11,12 Similarly, robust health equity science is grounded in and informs public health practice; findings illuminate ways to advance concrete reductions in health inequities. The aim of results-focused health equity science is to generate evidence that can be readily translated into programmatic interventions, policies, or systems changes, with the goal of eliminating health inequities.13,14
Conducting health equity science for action can help ensure that public health addresses appropriate scientific questions and uses appropriate data and methods to identify, implement, and evaluate program and policy interventions that support elimination, rather than just documentation, of health inequities. A health equity science agenda that provides the range of information needed by decision makers, such as disease burden and drivers, implementation evaluation, unintended consequences, cost and cost-savings, and impact, can provide useful evidence to inform interventions and policies needed to address the root causes of inequities.15,16 Practice-based research, which enhances external validity by examining associations and the implementation of interventions in real-world conditions, may incorporate a variety of disciplines and approaches, extending beyond randomized controlled trials and prospective cohort studies to proof-of-concept studies, case studies, evaluations, economic analyses, community-based participatory research, and formative assessments using a mixture of methods. 15
To conduct health equity science for action, public health practitioners can employ a conceptual framework, or theory of change, 9 for eliminating health inequities and describe the role of the scientific inquiries in advancing mechanisms of change. This framework will support the prioritization of scientific inquiries with a clear pathway to program or policy impact to reduce inequities. In addition, scientific inquiries are strengthened when they engage and seek input from communities, organizations, and partners with lived experiences and expertise to define priorities, interpret outcomes, and translate findings into action. 17 Robust evaluation of the impact of products generated by these scientific endeavors in supporting action to reduce inequities can guide future health equity science priorities and contribute to an evidence base on health equity change.
Emphasize Drivers of Inequity
Markers of health inequity are characteristics of population subgroups that are experiencing a health inequity. Examples of markers are race, ethnicity, and nationality. Drivers, on the other hand, are factors that create, exacerbate, and perpetuate health inequities. Drivers can operate at multiple points along the causal pathways leading to health inequities and can be mutually reinforcing, such as racism and other systems of oppression and discrimination, residential segregation, inequity in income, and inequity in health insurance coverage. 18
Examining markers of health inequity can help to document trends in known disparities and identify previously undescribed disparities. However, a scientific agenda that focuses only on markers can lead to stigmatization of populations experiencing health inequities. 19 Identifying and describing markers alone is also insufficient to support action to eliminate health inequities, whereas examination of drivers of inequity can guide development and evaluation of interventions. When examining drivers, public health scientists are encouraged to explore the purported causal pathways leading to inequity with supporting evidence where available and note opportunities to intervene.
Clarify Uses of Race and Ethnicity
Health inequities among racial and ethnic groups in the United States are pervasive and persistent.20,21 Health equity science can support ending these inequities by elucidating the processes and systems responsible for the associations among race, ethnicity, and health and by informing and evaluating interventions to disrupt the causal drivers of racial and ethnic health inequities. However, inclusion of race and ethnicity in scientific activities without appropriate context can undermine health equity efforts by unintentionally reinforcing misperceptions about the causes of racial and ethnic health disparities among policy makers, medical and public health practitioners, and the public. 22 Although the concept of race is a social construct, the myth persists that racial categories indicate biological or genetic differences that cause health disparities.23-25 This myth is both a product and an enabler of systemic racism.26-28 It causes harm by reinforcing tropes of racial superiority and inferiority; undercutting commitment across public health, health care, and other sectors to end inequities through portraying health differences as stemming from innate, nonmodifiable factors; and distracting public health and other practitioners and policy makers from devising and implementing interventions to address the actual drivers of health inequities, including racism, which CDC has declared a serious public health threat.26-29
To avoid perpetuating false racial narratives and to effectively develop strategies to end health inequities, the use of race and ethnicity in scientific work should be carefully reasoned, implemented, and articulated. 30 In particular, public health practitioners can state the rationale for including race or ethnicity in scientific analyses or data displays and explain how their analytic methods align with the stated rationale. For example, practitioners can consider stating explicitly that race and ethnicity are being examined as markers and not drivers of inequity and that analytic methods have been selected that meaningfully incorporate data on suspected causes of racial and ethnic health disparities. Likewise, public health practitioners are encouraged to include definitions and descriptions of the source data used for racial and ethnic categories. Practitioners may consider the benefits of engaging representatives of the communities to be included in scientific activities to receive input on the most appropriate terms and definitions to reflect the racial and ethnic identities of the participants and to develop hypotheses, analytic plans, data interpretations, and dissemination/translation approaches that appropriately address these identities. Making the conceptual and methodologic underpinnings of the scientific inquiry explicit can support readers to interpret the findings in ways that are consistent with the study objectives, methods, and data sources, rather than leaving readers to interpret the study findings on their own in ways that might be influenced by inherent biases and assumptions about causation. 26 This effort can also lead to constructive discussion about the appropriateness (including potential for benefit or harm) of the rationale that has been described.
When discussing the results of scientific inquiries that examine racial or ethnic health inequities, public health practitioners can avoid reinforcing the myth that race, as opposed to racism, causes health disparities by noting that race is a social construct and not a biological driver of disparities, and by avoiding baseless speculation that biology or genetics explain observed racial or ethnic disparities. Practitioners also can include discussion of racism (particularly structural racism) and the unfair distribution of social determinants of health as underlying causes of racial and ethnic inequities and consider pathways through which racism and other structural and social determinants of health might have operated to construct the observed findings.28,31 Reports simply describing racial and ethnic health disparities can be useful because they can uncover hidden disparities among subpopulations, raise public awareness, and monitor trends, but descriptive reports alone are insufficient. Purely descriptive data that are not contextualized might inadvertently “reify race as a biologic category and affirm social stratification as a normative aspect of civil society, leading to the conclusion that observed inequalities are simply the nature of things.” 26 In keeping with the previous principle emphasizing drivers over markers of inequity, effective health equity science explicitly frames descriptive examinations of racial or ethnic health disparities within larger efforts to understand and rectify the social forces and contextual factors that create and perpetuate racial and ethnic inequities.
Use Appropriate Measures of Disparity
The use of appropriate measures of disparity in evaluating interventions and tracking progress to eliminate health inequities is critical because their selection directly affects the analyses and the conclusions. Some recommendations include using both relative measures (eg, rate ratios) and absolute measures (eg, rate differences) in analyses, explaining the choice of measures (including benefits and limitations), providing the rationale for the reference group that is used, providing the rationale for making comparisons among 2 groups (pairwise) or multiple groups (eg, disparity indices or other summary measures), and considering and explaining the selection of methods for examining disparity trends (eg, use of shortfall/adverse or attainment/favorable measures, 32 use of relative vs absolute measures of disparity over time).33,34
Furthermore, proper interpretation and communication of health equity science findings require acknowledgment, and ideally discussion, of limitations inherent in the selected measures. Clear articulation of the rationale for the selected measures and comparison groups can further assist audiences in determining the implications of the health equity science findings for devising programmatic interventions and policy actions aimed at eliminating inequities. Carefully chosen measures that are suitable for tracking progress over time also support the evaluation of projects addressing health inequities.
Assessing progress toward elimination of health inequities requires a holistic understanding of disparities uncovered through quantitative measurement. To that end, qualitative and mixed-methods approaches are useful for exploring personal and community experiences related to health inequities.
Promote the Visibility of Groups That Might Be Inadequately Represented
The health of the US population depends on the health of all subpopulations. Beyond the obvious ethical imperative to serve all groups, it is necessary to monitor and enhance the health status of subpopulations to maximize the health of the entire population. For populations at risk of being inadequately represented in public health data because of social marginalization or exclusion, it is particularly important to purposefully and actively ensure visibility in data collection, data reporting, interpretation of findings, dissemination, and translation.
The inclusion of socially marginalized or excluded populations in the design of research agendas, research studies, public health surveillance systems, and other scientific endeavors may help to ensure that the health-related questions of highest priority to these populations are not overlooked. Early recognition of when enhanced data collection and data management are needed can facilitate reporting of health data for socially marginalized or excluded subpopulations. Community input can be helpful in identifying and providing guidance on closing potential gaps in representation in the data collected for a scientific endeavor.
Study designs and analytic methods that facilitate granular examination, including the intersectionality of data, can help ensure that the science includes the experiences of, and provides actionable results for, all relevant subpopulations. To accomplish this goal, it is important to disaggregate data, as appropriate to the research question, by relevant subpopulations. For example, it can be useful in data analysis to disaggregate data for Asian, Native Hawaiian, and (non–Native Hawaiian) Pacific Islander populations that vary in language, culture, and environmental experiences. 35 It is also important to consider data and interpret findings in ways that are congruent with individuals’ and communities’ experiences at the intersection of identities (such as being Black, female, and living with a disability). 36
While disaggregating data during the analytic stage, it is important to be mindful of data limitations for small populations (eg, the data may not meet criteria for statistical reliability) along with the pros and cons of using statistical modeling to generate more stable estimates. Combining years is an often-used approach but can limit the applicability of findings to current contexts and the ability to track trends over time. Special studies of key subpopulations can be conducted to supplement studies that are not able to have a sufficient sample size for those subpopulations. In the dissemination phase, limitations of the data sources or methods and implications for interpretation (eg, limited generalizability beyond a specified population) should be acknowledged. The dissemination phase of the scientific process also offers an opportunity to highlight the need for improvement of data sources to address the identified limitations. Finally, the inclusion of socially marginalized or excluded populations in the interpretation of results and development of recommendations and translation to action can help ensure that their interests are considered.
Address the Contexts That Contribute to Health Inequities
Health is shaped in many ways by the social and environmental contexts in which people live and work. 37 Health inequities likewise arise within and are influenced by the particular contexts affecting the relevant populations. In scientific inquiries that do not directly examine drivers of health inequities, or for which health disparities among population subgroups are not adequately explained in an analysis, a contextual perspective is important to reduce the potential for victim blaming by acknowledging the ways in which environmental conditions (and the structural factors that contribute to those conditions) influence health outcomes, including by shaping opportunities for health-promoting behaviors. 22 Explicit consideration of current and historical contextual influences also can strengthen the interpretation and dissemination of scientific findings. For example, research examining neighborhood-level assets by the proportion of the population that comprises people from racial and ethnic minority groups is well served by pointing to the larger context of redlining, which has deprived some communities of equitable access to healthy neighborhoods for generations. 38
Incorporating context into public health science also can help to identify and build an evidence base for policy and other systems-level interventions to improve health and eliminate inequities through environmental changes.39-41 Public health practitioners are encouraged to consider and, when possible, address the societal and environmental contexts that contribute to health inequities throughout all aspects of the scientific process. Perspectives of community members and those with relevant lived experience should be included, when possible, in identifying scientific questions and determining appropriate study designs that account for environmental conditions. Considering and remedying barriers to equitable participation in scientific endeavors can enhance scientific validity and promote fairness. Robust conceptual models and analytic methods that incorporate individual and contextual factors (eg, multilevel modeling) also are useful to inform and evaluate intervention strategies.
Conclusions
Science can be a powerful tool to advance health equity. Thoughtful application of the health equity science principles that we have described can improve the quality and impact of health equity science toward elimination of health inequities. These principles are not intended to represent a rigid checklist of features or actions that must be included in every scientific activity. Nevertheless, in situations in which relevant health equity science principles cannot be rigorously addressed, investigators should acknowledge the resulting limitations of the scientific findings.
Public health practitioners are encouraged to generate evidence from and share their experiences in applying and operationalizing these principles and also are encouraged to engage communities experiencing health inequities, as well as federal, state, and local public health agencies and organizations, to refine and expand the principles for use in varied settings. In so doing, an evidence base can be built that advances public health action to eliminate health inequities.
Footnotes
Acknowledgements
For contributions to the preparation and review of this article, the authors thank the CDC Excellence in Science Committee; CDC CORE Leadership Group; CDC subject matter expert reviewers (Renee Calanan, PhD, Randy Elder, PhD, Shambavi Subbarao, PhD, Donna Hubbard McCree, PhD, Kathleen McDavid Harrison, PhD); Michele Casper, PhD; Mary Cleary, MPH; and Schabbethai S. Senesie, MPH.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC)/the Agency for Toxic Substances and Disease Registry.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.