
Abstract
In recent years, health equity has become a universal goal. 1 However, when compared with investments in biomedical innovations, investments in interventions to achieve health equity have received little attention.2,3 Understanding how structural racism and systemic racism operate and affect health is important, but those insights alone will not lead to health equity. 1
According to the Centers for Disease Control and Prevention, health equity science is “science that investigates the underlying contributors to health inequities and builds an evidence base that will guide action across the domains of programs, surveillance, policy, communication, and scientific inquiry to move toward eliminating, rather than simply documenting, inequities.” 4 A fundamental challenge of health equity science is how to increase the capacity of individuals and groups to apply scientific principles and tools with a clear vision of what the nation and the world would look like after health equity is achieved. 5 In addition to the goal of removing structural and systemic barriers, the other goal of health equity science is to marshal knowledge, resources, and power to create a nation and world where race, ethnicity, place (location and caste), and other socially meaningful characteristics have no bearing on opportunities for people or populations to achieve optimal health and well-being.6,7
So far, an agreed-upon framework that operationally defines what it means to achieve health equity does not exist. 1 Antiracism is an educational and organizing framework that seeks to help individuals and communities create a vision of their goals and objectives, not simply to identify the problem or obstacles to health equity. 8 An antiracism approach often includes a structural analysis that recognizes that the world is controlled by systems and structures with traceable historical roots that unfairly disadvantage some, unfairly advantage others, and sap the strength of the whole society through the waste of human resources. 9 The components and processes for developing the lens, tools, and approaches to achieving health equity have not been well articulated.1,8 To help mitigate this problem, in this commentary, I argue for the need to integrate health equity science and antiracism to inform public health research and policy efforts to achieve health equity. I describe fundamental challenges in health equity science, outline an antiracism approach to health equity science, and identify key remaining questions and opportunities to facilitate the achievement of health equity.
Obstacles to Achieving Health Equity
Race continues to be a social category that precisely captures the effects of racism and the differential access to power, social and economic resources, and other desired resources in society rather than a biological construct that reflects innate differences. 9 Structural racism reflects the totality of ways that ideologies of inherent racial inferiority of socially defined groups (ie, races) create ranking or caste systems that differentially allocate societal resources and advantages. 10 Structural racism illustrates how ideologies (ie, cultural racism) operate through mutually reinforcing sectors of society (eg, health care, housing, education, criminal–legal system) in ways that determine population-level patterns of health and well-being (ie, the experiences of health, happiness, and prosperity).10,11
Racism vs Race
Historically, public health, medicine, nursing, and the social sciences have fixated on defining and addressing race, not racism. According to Dr William “Bill” Jenkins et al, 12 focusing on race instead of racism “has helped to reify the notion of race and obscure the underlying role of racism in producing the patterns of health inequities that persist in our society.” Characterizing racism as a fundamental determinant of health reminds us of why racism has been characterized as a “wicked problem” 13 : a scientific problem for which the causes and paths for resolving the problem are not clear. Racism is a wicked problem because (1) the effects of racism on health cannot be eliminated by addressing the mechanisms that seem to link them to outcomes; (2) as one mechanism linking racism to health declines, another emerges and becomes more prominent; (3) the relationship between racism and health will endure because the ability to access and use resources is transferrable to new situations and contexts; and (4) racial health inequities are rooted in differences in social, political, and economic power. 14 Racism has driven race and ethnicity to be markers of self-reported discrimination 15 and to be factors that influence social class, economic position, and other social determinants of health.16,17
Because the focus on race instead of racism has shaped how some researchers, public health practitioners, and policy makers understand why racial differences in health outcomes exist, some public health professionals tend to view the populations of interest through a deficit lens.18,19 By viewing a population group as being devoid of assets, strengths, and resources from which to build, public health professionals can become a part of, and not solve, problems for the population of interest.18,19 Strategies to intervene to improve the health of a population of interest can be limited by framing its determinants of health and intervention foundations through a comparative lens (eg, by comparing the population with people racialized as White in the United States). Thus, interventions must be anchored in the voices, perspectives, insights, and expertise of people who have lived experiences of the problem in context and have ideas about what is needed to mitigate or remedy the determinants of health inequities.20-24
The information needed to understand and achieve health equity is integrally intertwined, limiting the ability to characterize and define intervention approaches in such a way that would guide us toward a solution. 13 Tested interventions and efforts to achieve health equity have been limited by resources, time, and other considerations external to the problem; these contextual factors are often outside the scope and skill set of public health professionals.10,25 Achieving health equity is further complicated by the challenge of effectively framing racial and ethnic health inequities 26 and communicating to decision makers the problem’s logic, status, complexity, and depth.13,22
When and Why Should We Compare?
Uncertainty remains on when a racialized group should be compared with a standard 19 (eg, people racialized as White in the United States, the group with the best outcomes) or when a “minority health” approach 2 that focuses on the population of interest is preferable. A comparative approach is useful to identify a problem, need, or method for evaluating the differential benefits of an intervention but is not useful for explaining “why,” “how,” or “under what conditions” differences between groups exist. 27 Comparative approaches often parse cause without appreciation of context.19,26,27 As a result, public health professionals may erroneously conclude that patterns of variation (ie, what distinguishes 2 groups) are patterns of causation (ie, why 2 groups are different) 27 ; comparative approaches provide a flawed foundation on which to inform or build an intervention strategy. A comparative approach is not useful for identifying the assets and sources of strength that exist in a community or population, the unique aspects of the population relevant to an intervention approach, or the full range of modifiable determinants of poor health in the population of interest that have led to the existence and persistence of the modifiable difference in health.19,21 Similarly, intervention approaches that assume everyone will benefit equally often fail to do so and, in some cases, have exacerbated, rather than mitigated or eliminated, health inequities. 28
Benefits of Intersectionality for Health Equity Science
In the development of new approaches to health equity science, 7 the use of an intersectional lens is critical to ensure that health and structural or social determinants of health are identified and documented in populations that are not usually included through the traditional strategy of presenting race and ethnicity and sex and gender separately.29,30 Health equity research tends to focus on one socially defined characteristic at a time (eg, race or ethnicity), while not recognizing that other structures or aspects of identity are relevant (eg, gender, sexual orientation, gender identity, educational attainment). We continue to do a poor job of considering gender, men, and LGBTQIA+ (lesbian, gay, bisexual, transgender, queer, intersex, asexual, and other identities) health in conversations and efforts to achieve racial and ethnic health equity, including health equity science. As seen during the COVID-19 pandemic and at other points in the 2 decades since 2000, closing racial or ethnic gaps does not necessarily close gaps by gender within racial or ethnic groups. 30 One of the primary outcomes of health equity science is collective identification, or creating feelings of solidarity, collective efficacy, and shared culture and goals. 8 However, if done poorly, health equity science can make sociopolitically racialized and marginalized communities feel invisible and that their goals, dreams, and aspirations in achieving health equity are not to be realized.
Charting a Path to Health Equity
Countless resources have been invested in health disparities (now health equity) research and programs, but so far health equity has never existed. We may claim expertise in any number of disciplinary areas, analytic skills, and other aspects of health equity science, but we have no individual or collective proof that the goal that we are pursuing is in fact attainable. 1 Creary coined bounded justice as a conceptual framework that fundamentally challenges the assumption that health equity is achievable in the current context of structural inequities. 8 Creary noted that health equity is often presented as an ideal or a policy goal but is one that is imagined unrealistically. 8 If health equity is achieved, we also have to ensure the culture and political will to sustain equitable and just opportunities and outcomes.
ABC 2 : A Multipronged Strategy to Achieve Health Equity
Efforts to achieve health equity have typically focused less on the goal and more on documenting and addressing structural and systemic racism as barriers to health equity. This focus has presented a number of challenges, not the least of which is the recognition that racism is a fundamental determinant of health. 14 The goal of health equity tends to be imprecise and lack “SMART” goals (specific, measurable, attainable, realistic, and time-bound), 1 exacerbating the already complex issues that make health equity, not just racism, a wicked problem. 22
In the long history of social change traditions across the globe and in the United States, people of African descent and other populations have defined and focused on the goals that they seek to achieve rather than the barriers to achieving them. 31 In this spirit, I offer an approach to achieving health equity. Rather than conceptualizing efforts to achieve health equity as a single strategy, I argue that achieving health equity will require a structural multicomponent approach that addresses current issues and creates the culture and structures that will achieve and sustain health equity (Figure). I refer to this approach as ABC 2 : adapt to the context, build (community) capacity, change policy, and create well-being.
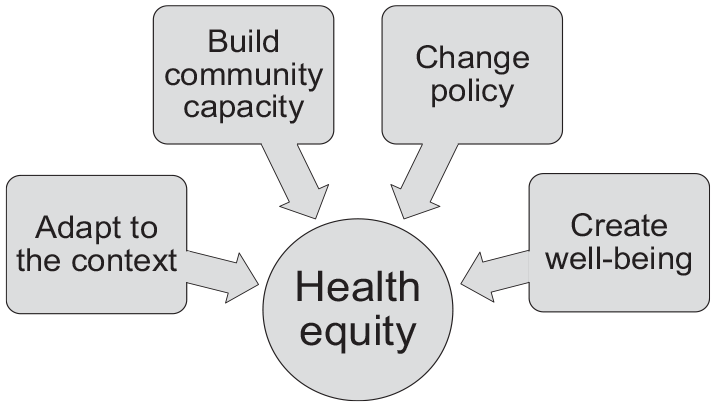
Achievement of health equity through ABC 2 , a multipronged approach that involves the following: adapt to the context, build (community) capacity, change policy, and create well-being strategies.
The ABC 2 approach is grounded in the understanding that poor health is due to structural and social conditions that concentrate risk in certain population groups and structural determinants of health that generate exposure to myriad risks over the life course. 28 The way to modify structures and contexts is by changing culture, practices, and policies that alter the context within which health is produced and reproduced, but this happens only when political will exists. The connective tissue of the ABC 2 approach is the shared conceptualization of the problem, assets, and goals that recognizes that each component of the approach is important. Conversely, it recognizes that each component is insufficient to independently create and sustain the conditions and context to achieve and maintain equity in health and well-being.
In the ABC 2 approach, interventions that help individuals and communities adapt to the context seek to maximize opportunities to be healthy despite poor environmental conditions. Adapting to the context is not merely accepting unhealthy conditions, but recognizing that people need to mobilize the resources and motivation to be as healthy as possible despite their living conditions. While we work to marshal and sustain the political will to achieve these systemic and structural changes, we must develop, implement, and disseminate health-promoting behavior change and community-based intervention programs, policies, and practices. These health-promoting interventions are often housed, implemented, and sustained in community-based organizations.
Community-based organizations, faith-based organizations, and civic and social organizations within people’s social and environmental contexts have been created or adapted to fill the needs left by gaps in and between health care institutions, public health systems, social services, and public policies.23,32 Building the capacity of these organizations is another key component of a comprehensive strategy to achieve health equity. Community-based organizations often are rooted in a nuanced understanding of the historical, social, political, and economic context that shapes the health of people in communities and the resouces that exist in these contexts. 23 Thus, continuing to invest and build capacity in organizations and efforts that can help friends, neighbors, and loved ones respond quickly and effectively to current and future threats to their collective health and well-being is essential to achieving and sustaining health equity.23,33
Policy change is a primary mechanism through which health equity can be achieved. As we learned from the Civil Rights Movement, cultural norms and shifts in interpersonal and social relations often follow policy change, not vice versa. 34 In addition to efforts to create new policies that promote equity, justice, and well-being, investments in efforts to change policy are needed to eliminate policies, practices, programs, and institutions that create and perpetuate inequity in opportunities and outcomes or that do not positively benefit or serve the populations of interest. 35 Although policy efforts to achieve health equity have tended to focus on the need for new policies, focus is also needed on de-implementing or eliminating policies that are ineffective or harmful (eg, the use of race in measuring kidney function, implicit bias training without other policy or institutional change). 1 Policies that are ineffective and harmful waste resources and often obscure, undermine, or underfund efforts that are promising or actually effective. 35
Finally, the ABC 2 approach includes the need to create well-being by implementing new polices and institutions that develop, monitor, and sustain health and well-being. Even if we eliminate structural and systemic racism tomorrow, we must imagine, develop, grow, and sustain those opportunities and resources that promote well-being and and foster happiness, life satisfaction, meaning, purpose, creative expression, close social relationships, and other aspects of life that make life worth living.36,37 Health is more than a state or status (eg, good or bad health, presence or absence of disease); health is a relational and instrumental concept that describes what one does or is able to do with and for others in one’s family and community.38-40 Well-being and health should be considered equal goals in US health policy.11,41,42 Although the approach to health equity in public health primarily focuses on health promotion, health is a resource for life and not the goal of living. Well-being equity, not health equity, should be the ultimate goal of programs and policies in housing, employment, education, the criminal–legal system, and other sectors of society that are determinants of health.43,44 Public health has focused on ensuring health and survival, but the goal may be larger than that: the goal is to enable well-being and the reasons that one wishes to be alive. 45 Thus, the primary goal of health policy and efforts to achieve health equity is to create a world that adds to the well-being of the population, not simply to help marginalized populations live longer or with greater mental or physical health.
Conclusions
In health equity science, our goal is to assemble innovations into tools, models, and strategies that will help move us past the “sideways” progress of replicating promising interventions in different populations or settings so that progress is made toward health equity. 46 Health equity innovations should be enhanced by recognizing the use of the ABC 2 approach includes multiple strategies to build on the lessons learned from previous efforts to achieve equity and justice. Future efforts should recognize the need to address contemporary conditions and should create future contexts to mitigate racism in all of its forms in order to promote equity in well-being.
Consistent with the principles of health equity science,4,7 antiracism characterizes the art and science of devising strategies to achieve health equity 8 when possible with community members. Art and science remind us to approach public health and health equity science with humility and creativity 22 and to recognize that diverse expertise is needed to devise new strategies to address the dynamic conditions that perpetuate health inequities. Here, “art” highlights the need for innovation and imagination to approach problems and solutions in new and different ways, particularly amid the realization that most public health outcomes are determined by factors outside the traditional scope and roles of public health. We therefore have to find new ways to use our data, influence, relationships, and power to partner with communities and educate those in other professional sectors on how health equity and well-being equity can be mutually beneficial. Health equity science and antiracism can be combined to guide efforts to achieve health equity.
Footnotes
Meeting Presentation
A version of this commentary was presented as a keynote address, “Why Is Health Equity Science a Priority?” at the April 2023 Health Equity Throughout the Science Lifecycle symposium, cosponsored by the Centers for Disease Control and Prevention (CDC) Office of Science, the CDC Office of Minority Health and Health Equity, and the University of California, San Francisco. In addition, elements of this commentary were presented as a keynote address, “Excuse Me . . . Can You Tell Me How to Get to Social Justice?” during the February 2022 Designing Interventions That Address Structural Racism to Reduce Kidney Health Disparities virtual meeting, sponsored by the National Institute of Diabetes and Digestive and Kidney Diseases.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article has been supported in part by the American Cancer Society (RSG-15-223-01-CPPB) and the National Institute on Minority Health and Health Disparities (5U54MD010722-02).