
Abstract
The COVID-19 pandemic has tested health care professionals to the extreme. This study investigated the re-enchanting effect of shared leadership and passion at work in the context of public health care. This study advances on the Self-Determination Theory to suggest that shared leadership has a positive effect on resilience and performance through passion at work at different levels of analysis. A sample of 518 physicians working in Spanish public hospitals was used. The results showed that shared leadership was associated with team and individual outcomes via passion at work at team level, while no significant mediating effect was found for passion at work at the individual level. The theoretical and practical implications of the findings are discussed, limitations are considered, and future research directions are suggested.
Introduction
More than any other crisis, the COVID-19 pandemic is probably the greatest global challenge in recent times, involving deep shifts in social, economic, and political relations. COVID-19 is testing the health and well-being of people around the globe. Besides serious perils to social stability, economic development, and human health, patient care is accompanied by huge stress on health care professionals. Given that caring for patients requires physicians to be physically and mentally healthy, the ability of the health care system to remain a healthy place to work is currently at stake. Before the COVID-19 pandemic, exhaustion and depersonalization were frequent among public health care physicians. The situation causes worry, as doctors in particular are known to be more vulnerable to ill-being and even suicide than most other professions (Gerada, 2018). These issues have increased during the pandemic, as COVID-19 has stretched the medical profession physically and mentally, reaching crisis point. Some physicians are even considering leaving the profession, as they feel “the loss of a deeply meaningful relation with one’s surroundings” (Endrissat et al., 2015, p. 1558), namely, they feel disenchanted. The main objective of this research is then to offer a model to re-enchant public health care organizations.
Several studies have revealed that physicians are suffering from depression and anxiety as a consequence of the coronavirus pandemic (Rimmer, 2020). At the same time, physicians are responding with an extraordinary demonstration of altruism by delivering optimum patient care even though they are at serious risk of becoming infected. The main objective of this research is to offer hospital managers a tool to reinvigorate positive attitudes toward the health care profession. Against the absurdity of the hyper-rationality of the modern world (Wallace, 2011), an enchanted view of institutions is possible through the power of human enthusiasm, reflection, or what Suddaby et al. (2017) call, magical thinking. In particular, we propose shared leadership and passion at work as central mechanisms to re-enchant public health care workers. We understand re-enchantment as the emergence of resilience and improved performance through passion at work.
The impact of the pandemic on the reality of physicians’ work has been dramatic. Physicians from all specialties have had to stop their normal activities to treat COVID-19 patients. They have had to update their knowledge about the virus, and they have had to follow strict protocols to protect themselves when dealing with infected patients. They have also faced the added pressure of COVID-19 being an unknown disease with very limited treatment options and an unpredictable patient evolution, coupled with the constant tension of whether they will be infected and pass on the infection to their families. To prevent this, many of them have decided to isolate themselves to protect their families, resulting in them not being able to be with their young children.
Considering the complexity of this context, physicians are basically asking for increased autonomy, competence, and relatedness (Hartzband & Groopman, 2020). They need autonomy to decide how to organize their schedule to enable different styles of practice and patient interaction. This is especially valuable considering the challenges involved in the unpredictable effects of COVID-19, ranging from asymptomatic patients to those whose health suddenly worsens. However, physicians also need to acquire new knowledge quickly and to put it in practice. The pandemic makes rapid and simple access to updated knowledge and medical protocols even more critical. In this sense, medical units that share knowledge and receive support from colleagues seem to have not only reduced COVID-19 contagion among medical staff but also improved the quality of patient care (Salas-Vallina et al., 2020). Finally, physicians lack a feeling of interpersonal attachments and connection to the social organization and their work units. Feelings of support and connection are fundamental to them, as they are suffering from exhaustion, the loss of many patients, and isolation from their own families. Autonomy, competence, and relatedness become central to physicians’ psychological well-being (Hartzband & Groopman, 2020).
According to the Self-Determination Theory (SDT) (Deci & Ryan, 2000), human motivation emerges by fulfilling individuals’ basic, innate psychological needs for autonomy, relatedness, and competence. Collective forms of organization, such as shared leadership, involve carrying out leadership tasks and participating in decision-making (Shane & Fields, 2007), which entails a sense of autonomy and competence. Yet shared leadership also fosters interaction and social networks, and generates mutual responsibility and a common identity, thus creating a context where positive feelings and passion emerge.
The benefits of shared leadership have been highlighted as a means of fostering a number of team and individual outcomes (Wang et al., 2014; Zhang et al., 2012). Rodríguez-Sánchez et al. (2020) suggested that self-managed ad hoc teams, involving shared beliefs, visions, and cognitions, led to improved performance. However, this has not always been the case, and the effects of shared leadership remain, to some extent, ambiguous (D’Innocenzo et al., 2016; Lorinkova & Bartol, 2021). Recent research has tentatively shown the relevance of health care teams in improving effectiveness, yet a more hierarchical approach still prevails in literature (Lowe et al., 2017). As shared leadership has been found to have several effects on different types of outcomes, it is our aim to untangle these by considering consequences in terms of improved capacities (resilience) and performance at both the individual and team levels of analysis.
Recent calls have been made to explore the potential role of resilience to bounce back from adversity (Stoverink et al., 2020). However, there are still considerable inconsistencies regarding temporal issues and the role of adversity in resilience studies (Fisher et al., 2018). In addition, other recent research calls have been made to explore the mechanisms and factors that individuals and teams use to manage adversity (Hartmann et al., 2020).
Empirical works have underlined the need to explore the potential capacity of collective forms of leadership, such as shared leadership, to achieve positive outcomes in stressful and complex contexts (Mitchell & Boyle, 2020; Q. Wu et al., 2020). Shared leadership can lead employees to have a stronger connection and feel more identified with their jobs, making them more passionate at work, in turn fostering resilience and performance. This is because passion is a major motivational force that helps to deal with exhausting medical practice activities. Passion is a useful concept to explain persistence despite obstacles and adverse experiences, and can be defined as “the coincidence of commitment and high arousal approach motivation” (Moeller, 2014, p. 13). However, scarce evidence can be found on how passion drives the effect of shared leadership on job outcomes.
Shared leadership involves carrying out leadership tasks and participating in decision-making (Shane & Fields, 2007), which entails a sense of autonomy and competence. Yet shared leadership also fosters interaction and social networks and generates mutual responsibility and a common identity, thus creating a context where positive feelings and passion emerge.
To fill these gaps, and advancing on the SDT, we propose a time-lagged multilevel model which aims to shed light on (1) the effect of shared leadership on resilience and performance at team level, through passion at work at team level, (2) the effect of shared leadership on resilience and performance at individual level, through passion at work at team level, and (3), the effect of shared leadership on resilience and performance at individual level, through passion at work at individual level (Figure 1).
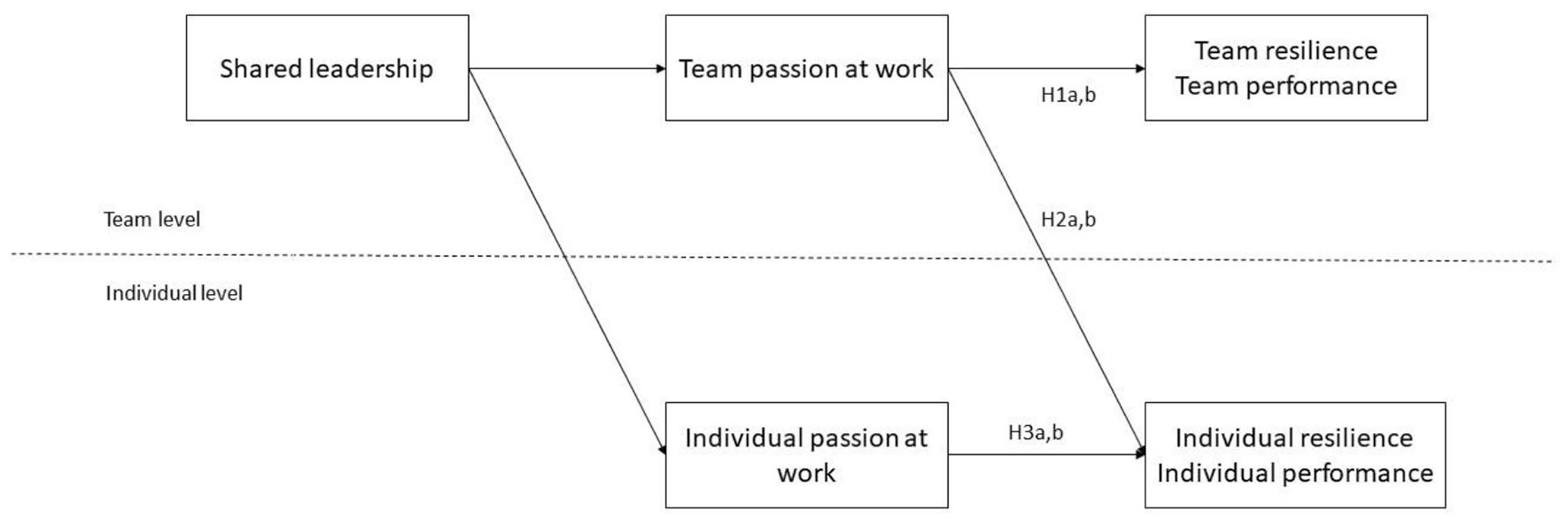
Theoretical model.
To further unfold this unresolved connection, we draw on SDT (Deci & Ryan, 2000), as a large amount of studies confirm the relevance of positive emotions for building resilience (Loh et al., 2014) and performance (Fan et al., 2014).
First, we argue that the apparent influence of shared leadership on team performance and team resilience is unraveled by passion at work at team level. Physicians dealing with COVID-19 patients suffer from fatigue, exhaustion, and a sense of helplessness, and the power of collective forms of passion in their work unit could re-enchant them. Under extreme working conditions, where physicians experience the continuous death of patients, group support and shared identification with the profession and the power and strength of colleagues could help to overcome the negative circumstances. We also focused on passion at team level because the team is a central component of health care. Patient care depends on the quality of teamwork, since communication and coordination in health care units are crucial mechanisms to address complex therapies (Rosen et al., 2019). We argue that passion at team level provides energy-building engagement in valued activities.
While teamwork has been linked in some ways to positive effects on team performance (D et al., 2016) and team resilience (Hartwig et al., 2020), the role of particularly energizing, intense experiences, such as passion, has received scarce attention in health care. In this vein, Chummar et al. (2019) pointed out that there are limited studies addressing the effect of passion at work on performance. Until recently, passion has received scarce attention, with studies focusing on related constructs placed under the umbrella of attitudes and emotions, such as engagement, happiness, vigor, enjoyment, and thrills (Ancarani et al., 2019; Ehrnrooth et al., 2020; Fisher, 2010; Mousa et al., 2020; Rodríguez-Sánchez et al., 2020). Passionate health care work units are expected to create stronger teams which are capable of overcoming the challenges inherent to COVID-19 and reporting improved unit performance. Accordingly, our first objective is to examine the mediating role of passion at work at team level, in the relationship between shared leadership and team-level outcomes (resilience and performance).
Second, given that scholars have emphasized that research on leadership is intrinsically multilevel in nature (Bliese et al., 2002), we propose that passion at work at team level has positive effects on team- and individual-level outcomes. We posit that team passion positively mediates the relationship between shared leadership and individual outcomes, namely individual resilience and performance. Passion has demonstrated positive effects not only on teams but also on individuals (Brief & Weiss, 2002), having beneficial effects on individuals’ actions at work (Tims et al., 2013). However, we wonder if these benefits also occur in an exceptional crisis context. Passionate health care work units involve high-quality interactions and support for physicians, given that commitment and motivation are central components in the concept of passion (Moeller, 2014). In times of COVID-19, health care units are made up of physicians from different specialties who need training in COVID-19 procedures. Physicians ask for second opinions and require access to updated knowledge and procedures. Highly committed and motivated work units could have an impact on how physicians feel individually, as they could spread their positive energy and support to other individuals, thus making them more resilient. Nonetheless, it has recently been argued that scholars have focused on a single level of analysis when exploring the antecedents of resilience. Based on the above, our second objective is to assess the mediating role of passion at work at team level, in the relationship between shared leadership and individual outcomes (resilience and performance).
Third, beyond the team-level mediating effect of passion at work, the SDT provides a theoretical base to explore passion at work at individual level. Shared leadership is expected to foster the motivation and commitment components of individual passion at work, in turn acting as job resources that result in positive job outcomes, namely individual resilience and performance. However, is individual passion at work enough to address highly demanding circumstances, or is a higher level of passion, such as passion at team level, more effective? Positive emotions can develop resources for improved performance and well-being (Meneghel et al., 2016), and physicians experiencing higher levels of vitality and vigor might experience increased individual resilience. As a third objective, we suggest checking the mediating role of passion at work at individual level, in the relationship between shared leadership and individual outcomes (resilience and performance).
In sum, we propose that this is the time for collective forms of leadership to contribute to performance as well as to healthier organizations through passion at work. The multilevel approach proposed offers some advantages in shedding light on how to re-enchant health care organizations. First, we show whether physicians at individual level can benefit from shared leadership and passion at work at team level in the same way as medical work units at the unit level. As explained later, individual and team resilience and performance are different constructs, and the mechanisms affecting work units as a whole can differ from those influencing individuals. However, a pathway that fosters both individual and team-level outcomes would be a major step forward. Second, by considering the mediating role of passion at work at individual level, we could clarify and compare the effect of a collective form of passion that is related to individual passion. Accordingly, the issue could be resolved if strong shared emotions such as passion were more effective than individual emotions in high-pressure, extreme working circumstances.
This article is organized as follows: the first section reviews the literature related to understanding the relationships between the main variables. This is followed by an explanation of the research methods used. The next section outlines the results of the fieldwork. Then, the implications for theory and practice are presented. The final section focuses on limitations and future research directions.
Shared leadership
The concept of shared leadership has been defined in numerous ways by researchers. It was Gibb (1954) who first introduced this concept. Pearce and Conger’s definition conveyed the common core of these definitions as the distributed, collective, and/or mutual influence of team members (Q. Wu et al., 2020). According to Pearce and Conger (2003, p. 1), shared leadership refers to “a dynamic, interactive influence process among individuals in groups for which the objective is to lead one another to the achievement of group or organizational goals.”
Unlike formal leadership, which is based on vertical interaction among the formal leader and his or her followers, shared leadership involves distributed informal leadership arising from team members, who influence each other in a way that helps to achieve team-level outcomes (S. Liu et al., 2014). In this vein, shared leadership involves interactions among team members that collectively make use of leadership influence, perform tasks typically restricted to the formal leader, and participate in the decision-making process (Shane & Fields, 2007). According to Ali et al. (2020), shared leadership involves a social interaction process where team members play both leading and following roles, and share power and responsibility to achieve team objectives (C.-M. Wu & Chen, 2018). Under this perspective, shared leadership is a complex interaction process, especially developed in knowledge-intensive professions (Scott-Young et al., 2019), such as the medical sphere. Physicians need to make complex decisions based on in-depth knowledge. In contrast, traditional leadership theories, based on individual and hierarchical formal leadership, might be more appropriate for jobs in other time periods of history (Ali et al., 2020).
Shared leadership has been related to individual and team effectiveness (Chiu et al., 2016; Somech, 2016) and team pro-activity (Erkutlu, 2012). Interaction and social networks create opportunities for team members to discuss problems and find solutions (Ali et al., 2020), and the involvement of team members in participative decision-making can reinforce and reinvigorate employees’ energy and motivation. However, improved team effectiveness is not always guaranteed by shared leadership (Ali et al., 2020; Boies et al., 2011). There remain decisive challenges for research on the complex connections between leadership and healthy workplaces (Nielsen & Taris, 2019). Therefore, prior studies leave room to consider a more human approach as an explanatory mechanism whereby shared leadership might influence work outcomes. Particularly energizing positive attitudes, such as passion at work, might explain how shared leadership positively affects effectiveness and employees’ capacity to address complex situations, namely resilience.
The mediating role of passion at work at team level in the relationship between shared leadership at team level and team outcomes
This study aims to provide evidence for the mediating role of passion at work at team level that may explain the relationship between shared leadership at team level and team outcomes. Two team outcome indicators were used: (1) team resilience, understood as a team’s belief that it can assimilate and manage pressure and stress, as well as a team’s ability to handle, recover, and adapt positively to adversity (Carmeli et al., 2013) and (2) team performance, which involves team in-role or formal team behaviors and team extra-role or behaviors that exceed what the team is expected to do.
Defining passion at work at team level
Vallerand et al. (2003) suggested a dual model for passion, which includes harmonious passion and obsessive passion (Mageau et al., 2009). Harmonious passion involves free engagement in a favorite activity, which does not have an uncontrolled effect on the individual’s life, yet it remains consistent with all other aspects of one’s life. Conversely, obsessive passion makes individuals engage in an activity controlled by external factors, thus taking up an unbalanced space in one’s life. Subsequent research extended the concept of passion to strong motivation and commitment toward an activity, involving four components: (1) continuous attempt to engage in the activity, (2) identification with the activity, (3) goals referring to the activity, and (4) intense motivational approach to the activity (Moeller, 2014). Compared to related constructs, such as work engagement, passion at work involves the task becoming part of an employee’s identity (“I am a human resources manager who loves his or her job”), while engagement is seen as a state of mind resulting from one’s positive experience at work (i.e., “I feel energetic and dedicated to my work”).
Employees experiencing passion at work can fully concentrate on their work, enjoy it, and at the same time can focus their attention and energy on non-work-related tasks, in such a way that they do not need to constantly think of their work (Vallerand & Houlfort, 2003). This research focuses on the positive side of passion at work, developed by Moeller (2014), which is more consistently related to positive outcomes, such as resilience and performance. In particular, we initially propose the mediating role of harmonious passion at work at team level, in the relationship between shared leadership and two outcomes, namely, team resilience and team performance.
The team level within health care is important because the quality of teamwork is related to the quality and safety of patient care. In public health care, teams have become increasingly important in developing the ability to effectively respond to and promote positive adaptation changes. Communication failures among team members are directly associated with patient harm. Miscommunication of critical information about the patient status can lead to wrong treatments. In health care, coordination and teamwork have been ignored as central mechanisms to address complex work tasks (Heath & Staudenmayer, 2000). Therefore, teamwork is fundamental, as no individual can guarantee the best standard of care, or protection from potential errors, derived from challenging and sophisticated therapies (Rosen et al., 2019).
Because passion has not been clearly defined at team level, we propose a definition based on Cardon et al. (2017) and Vallerand et al.’s (2003) conceptualization of passion at work. We define team passion as the intense, positive, shared feelings experienced by members of a team, which show a strong connection with a preferred and valued activity that is incorporated into a team’s identity. Team passion has a close connection to the concept of enchantment. Enchantment has been defined as an “aura of authentic presence, resisting rationalization and promoting creative social connection,” and is related to the meaningful and captivating aspects of a job or organization (Endrissat et al., 2015, p. 1556). The magic felt by passionate employees who feel the “magic of the clan,” or the emotional connection experience by a group, shows that passion at the team level has a strong linkage with work enchantment. Team passion, therefore, could be a proxy of a re-enchanted workplace.
Team passion is captured by asking individual team members what the team is passionate about and to what extent (Chan, 1998). Therefore, the team is the reference point for passionate feelings and identity. It is team passion which includes the collective identity and shared feelings of the team and is disjointed from individual identities or feelings. Team-based variables (referent-shift consensus constructs) are conceptually different from individual-level constructs in the same field. Individuals can show little passion for a particular task, but may admit that the team has strong feelings of passion for that activity.
Shared leadership and passion at team level
The SDT (Deci & Ryan, 2000) states that human motivation is the result of fulfilling individuals’ basic, innate psychological needs for autonomy, relatedness, and competence. In addition, humans need to engage in constant exchanges to meet those needs. In the health care context, autonomy, relatedness, and competence become even more important, as physicians work in teams, yet also have a significant degree of autonomy. Physicians require a high level of competence and expertise, as they have an immense responsibility to improve the quality of life of patients. They have to make critical decisions based on their own knowledge, but they also need to exchange knowledge with colleagues, to support them, and to receive support from them.
Shared leadership involves carrying out leadership tasks and participating in decision-making (Shane & Fields, 2007), which entails a sense of autonomy and competence. Yet shared leadership also fosters interaction and social networks, and generates mutual responsibility and a common identity, thus creating a context where positive feelings and passion emerge.
SDT identifies controlled (extrinsic) regulation and autonomous (intrinsic) regulation. Controlled regulation relates to engagement in an activity for instrumental reasons (rewards, fear of causing disappointment, status). Autonomous regulation is related to an individual’s engagement in an activity for its own significance, pleasure, or enjoyment (Meyer et al., 2010). In this sense, passion at work is said to emerge as a result of autonomous internalization of behavioral regulations, which leads to a strong, yet controllable, desire to become immersed in an activity, generating a sense of volition about performing it (Mageau et al., 2009). Vallerand et al. (2003) argued that when people value their activity for autonomous reasons (the satisfaction it brings), this creates harmonious passion at work. According to Vallerand et al. (2003), the dimension of value is particularly relevant to the concept of passion because it differentiates passionate activities from other engaging but irrelevant activities toward which individuals are intrinsically motivated. According to SDT, this internalization occurs in environments where individuals feel connected and supported by others, namely, within teams.
Team members’ autonomy should contribute to team passion because autonomous individuals take initiatives and seek challenging activities, thus fostering passion (D. Liu et al., 2011). In addition, it has been argued that, in public health care, positive relationships between physicians and their immediate superior and with their working group lead to positive attitudes (Ancarani et al., 2019). Shared leadership, therefore, fosters social connections and the magic of positive attitudes, while promoting effectiveness. This is what Endrissat et al. (2015) called the “fusion of rationalization and enchantment,” which open new ways of managing human resources. In this vein, a team environment of shared leadership exerts higher proximal influence on team members than an individual scenario, in turn creating and integrating team members’ feelings, resulting in collective passion at work.
Passion at work at team level and team-level outcomes
In turn, we propose that team passion is a major motivational force that enables teams to endure long and exhausting medical practice activities, and that it contributes to the attainment of high levels of team resilience and performance. Team resilience can be defined as “the capacity of a team to withstand and overcome stressors in a manner that enables sustained performance; it helps teams handle and bounce back from challenges that can endanger their cohesiveness and performance” (Alliger et al., 2015, p. 177). Team performance refers to formal team behaviors at work (in-role behaviors) along with those behaviors that go beyond what is expected from the team (extra-role behaviors). Resilience enables the team to be prepared for upcoming events (Egeland et al., 1993). However, how teams’ collective resources influence their capacity to adapt to adversity has traditionally been overlooked (Morgan et al., 2013). In this vein, identifying the variables that develop team resilience is crucial to be ready to respond to unfavorable future public health situations. Resilience is boosted by the presence and quality of relationships (Gittel et al., 2006), involving coordinated activities in which physicians complement and support each other, thus representing a collective approach to passion (team passion). Affective reactions and emotions among team members can be concurrent, and the team can attain a collective mood. It is not only individual passion but also the combined and composite feelings of passion that improve team resilience. Therefore, collective positive emotions are related to the greater availability of team resources and resilience to adversity (Meneghel et al., 2016). Following the propositions of the job demands-resources (JD-R) model, we argue that shared leadership fosters team passion, thus strengthening team resilience. Job demands, represented by the stressful and highly adverse conditions experienced by physicians during the COVID-19 pandemic, could be counteracted by the job resource of shared leadership, and its effect on team passion. Furthermore, job demands could improve the effectiveness of job resources (Demerouti et al., 2001).
In addition, over the last two decades, there has been open debate on the issue of how health care can be managed to improve performance (Reibling et al., 2019). In this respect, recent calls underline the need to examine the potential effect of variables on organizational performance (DesJardine et al., 2019). Passion produces a strong motivating force to participate in team activities (Vallerand et al., 2003). In addition, passion can make a difference in team performance because passion is stronger than intrinsic motivation, and passionate team members internalize team tasks as part of their identity (Amabile & Pillemer, 2012). While pessimism is likely to produce negative self-fulfilling prophecies that lead to contagious dissatisfaction and disengagement, thus affecting co-workers in a downward spiral of negativity, shared team passion can address the damaging factors resulting from active participation in team activities, making passion a central factor for hard work to achieve success. Thus, our first hypotheses are as follows:
The cross-level mediating effect of passion at work at team level in the relationship between shared leadership at team level and individual outcomes
According to Brief and Weiss (2002), affect, identity, and passion have a powerful effect not only on teams but also on individuals. This study assumes cross-level effects between shared leadership at team level and individual job outcomes (individual performance and individual resilience), as mediated by passion at work at team. Individual resilience is understood as the belief that one can assimilate and manage pressure or stress, as well as one’s capacity to handle, recover, and adapt positively to adversity (adapted from Carmeli et al., 2013). In health care, individual resilience refers to the capacity to address complex clinical issues, conflict with patients or colleagues, lack of resources, organizational pressures, or a combination of the above. Individual performance refers to individuals’ in-role or formal behaviors (comply with the work schedule, remaining up to date in medical practice, attending research sessions, etc.) and individual extra-role or behaviors that exceed what the team is expected to do (extending the working day, reducing patient bureaucracy, providing support to colleagues outside working hours, etc.).
As we have argued before, team passion is expected to emerge when team members feel ties in an environment of collaboration. Shared leadership is particularly aimed at fostering social connections and a positive atmosphere that integrates mutual and shared positive feelings among team members, thus resulting in team passion and passion at work.
At the same time, in team settings, physicians need to share ideas and knowledge when making decisions about the team’s activities, which might have an effect on individual actions at work (Tims et al., 2013). Teamwork involves mutual influence that could explain why team members’ affective experiences, such as passion at work, are related to individual affective experiences and behaviors (Torrente et al., 2012), including resilience and performance.
In examining how passion at team level influences individual resilience and individual performance, we rely on social psychological theories of social norms, modeling, and emotional contagion. Modeling involves acquiring fundamental skills and strategies rather than literally imitating others’ behaviors. Team members’ passion can fuel individuals’ energy, vigor, and vitality to face complex situations and recover successfully from them. Emotional contagion affects team members’ affective states, judgments, and behaviors (Ilies et al., 2007). Bakker and Xanthopoulou (2009) suggested that an individual becomes stronger (vigorous) through modeling when employees imitate each other’s movements, language, and expressions and, consequently, experience similar feelings. The power and strength provided by a passionate team might help to address work intensification and the increased pressure of specialized medical units. Thus, we argue that organizations can effectively support their employees in overcoming difficulties and bouncing back from adversity through team passion.
Regarding the effect of team passion on performance, we used the social psychological theories of social norms and modeling. Norms refer to shared beliefs that guide individual behaviors (Taggar & Ellis, 2007), and can be very effective as team members push each other to follow the norms. When physicians face team challenges, and the team reacts proactively, exhibiting motivation, energy, and identification with the task, namely, team passion, this team might be signaling proactive behavior aimed at fostering individual performance. In this sense, shared beliefs and feelings in a passionate team of physicians could channel and spread these intense, positive feelings and attitudes, thus improving individual performance.
Modeling is related to observational learning and enables individuals to deduce which behaviors are appropriate at work (Tims et al., 2013). By observing team members’ attitudes, individuals engage in roles which have a significant impact on the performance of individual team members. Accordingly, we posit that physicians working in the same team act as role models, whereby high-performance team members encourage other team members engage in this behavior. For all the above, our second hypotheses are as follows:
The cross-level mediating effect of passion at work at individual level in the relationship between shared leadership at team level and individual outcomes
Shared leadership and passion at work at individual level
We have previously argued that shared leadership exerts a positive effect on team passion, as shared leadership fosters a mutual identity and shared purpose that is expected to have a motivational effect on employees (Cardon et al., 2017). Beyond this team-level effect, it is our aim to delve deeper into the effect of shared leadership on passion at work at individual level and the consequent effects on individual resilience and performance. Team passion and individual passion are different constructs, as the former refers to the collective level, where individuals share intense, mutual feelings and motivations, and the latter is limited to the particular case of each employee. A similar mediating effect could be expected of both team and individual passion at work, as they derive from the general definition of passion. However, passion at work at team level is different from individual passion at work. Passion at team level is a new form of the construct of individual passion, which is aggregated to a higher level based on within-group consensus. Team-level passion changes the reference for its conceptual definition and operationalization. Therefore, the examination of its cross-level effect leaves room to analyze potential differences in the mediating role of passion, depending on the level of analysis. Passion at work at team level involves an individual description of other team members’ perceptions of passion. Although the original construct, passion, remains unchanged in this variable, the reference context has changed (Chan, 1998). Conversely, individual passion at work assesses one’s own perceptions of passion at work and lacks the social connections inherent to team passion.
Passion at work explicitly incorporates motivational and commitment elements (Moeller, 2014), which facilitate the exploration of the mediating role of passion at work at individual level in the relationship between shared leadership and individual outcomes. Passion at work involves an intensive, persistence approach motivation that enables employees to tackle demanding tasks and adverse work experiences. Physicians dedicate a lot of time and effort to carrying out their tasks successfully. They have a special professional vocation involving a strong commitment to their job. Commitment is also considered a central component of work passion, as it contributes to overcoming difficulties (Le & Agnew, 2003).
Team-level shared leadership promotes feelings of a shared purpose, thus heightening the level of motivation (Kirkman & Rosen, 1999), and therefore increasing the commitment toward a job. In addition, shared leadership enables physicians to be autonomous and capable, which affects their motivation toward the activities performed (cognitive). In addition, the autonomy provided by shared leadership increases physicians’ interest in persisting with the activity, thereby fostering a romantic and positive relationship with the task despite adverse experiences such as uncertainty and exhaustion (Moeller, 2014). This, in turn, promotes passion at work (D. Liu et al., 2011). Autonomous individuals undergo a motivational process in which they plan by themselves, and this can strengthen passion at work at individual level (Gao et al., 2019).
Based on the JD-R model, shared leadership can act as a job resource enhancing passion at work at individual level. Under this model, individual positive attitudes are enhanced by job resources (Demerouti et al., 2001). Building on the JD-R model, Ancarani et al. (2019) revealed that a climate of autonomy, empowerment, and integration improved positive attitudes among public health care professionals. At the same time, SDT provides a theoretical framework to explain that by covering the basic psychological needs of autonomy, competence, and relatedness, employees react with positive attitudes. In this vein, we suggest an effect of shared leadership on employees’ passion at individual level. Employees who can draw upon more resources (Rahmadani et al., 2019), and who perceive that their basic needs are satisfied, are expected to be more passionate at work. This is because a work context where individuals voluntarily influence others, and at the same time accept mutual influences, creates feelings of recognition and mutual trust, thus leading to increased intrinsic motivation (Song et al., 2020).
Passion at work at individual level and individual outcomes
In turn, passion at work at individual level can positively influence both resilience and performance at an individual level of analysis. In general, we can argue that positive attitudes, such as engagement, predict lower levels of burnout and improve performance (Bakker et al., 2004). Passion for one’s work has mainly been related to positive outcomes, such as persistence, enthusiasm, and overall success (Vallerand & Houlfort, 2019). According to Fredrickson’s broaden-and-build theory (Fredrickson, 2001), positive emotions can develop resources for long-term success and well-being. In particular, the broaden-and-build theory posits that positive emotions build enduring personal resources, such as resilience (Fredrickson et al., 2003; Meneghel et al., 2016). All of this leads us to argue that extra doses of energy, derived from the voluntary internalization of an activity, foster individual resilience.
Recent research provides theoretical foundations that connect passion and performance (Chummar et al., 2019), yet more empirical evidence is needed, particularly when differentiating between levels of analysis, and considering knowledge-intensive and challenging contexts, such as health care, and especially at the current time. Team-level shared leadership fosters feelings of being competent, autonomous, and empowered, thus enabling employees to improve their performance. In addition, positive appraisals of work environment characteristics lead to positive work intentions to use discretionary effort and improve performance (Thibault-Landry et al., 2018). Studies have found that these intentions deriving from psychological processes are reliable predictors of both in-role and extra-role behaviors (Dubinsky & Skinner, 2002). Therefore, we expected to find the following:
Method
Sample and procedure
We used a two-wave field survey of specialty medical units in Spanish public hospitals. Heads of medical units were contacted and provided support for our research. They informed their teams about the aims of the study and the significance for managerial research. The participants were told that they would receive a final report of the study results to improve their involvement. In Time 1 (November to January 2019), physicians were asked to respond about their shared leadership perceptions in their work units. In Time 2 (June to August 2020), physicians were asked about their passion at work and team resilience perceptions, and heads of medical units were asked about their team performance. In Time 2, physicians were also asked about their individual passion at work, resilience perceptions, and their individual performance. During Time 2, the physicians acquired experience on how to treat COVID-19 patients and how to leverage their resources so as to foster community ties and partnerships. As of June 2020, the pressure on hospitals decreased returning to more acceptable levels. All of this made it easier for them to participate in this research despite the pandemic.
To participate in the study, 70 hospitals and 210 medical units were invited. A total of 518 questionnaires were returned, from 121 medical units in 49 hospitals, which corresponds to a response rate of 19.36% of total public hospitals (253) in the Spanish National Health System (in accordance with the Spanish Ministry of Health Care, Consumer Affairs, and Social Welfare). The medical units which completed the questionnaire were allergy (12), dermatology (11) emergency (19), hematology (9), infectious diseases (12), internal medicine (17), obstetrics (8), surgery (26), and urology (7). Table 1 shows descriptive statistics of gender, job stability, age, and tenure.
Gender, job stability, age, and tenure.

Measurement
Shared leadership was measured at the team level using Chiu et al.’s (2016) measurement scale, which consists of five items in a Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). The scale is based in the social network approach, which means that it considers the density of the leadership network. The greater the density, the greater the shared leadership. Physicians rated the extent to which they rely on their peers in the following functions: facilitating planning in the organization, aiding in problem-solving, providing personal support and consideration, and fostering development and mentoring (i.e., “the members of my team give support and consideration to other team members”). A final item based on an overall evaluation of leadership was used. The degree of inter-rater reliability among raters was checked using intraclass correlation coefficient 1 and 2 (ICC1 and ICC2) (LeBreton & Senter, 2008). In addition, the inter-rater agreement index (rWG(J)) was calculated to evaluate consensus between ratings. The results indicated ICC1 standing at .53 and ICC2 at .90, and the median level of rWG(J) was .91, ranging from .88 (strong) to .97 (very high), thus providing support for the aggregation of this construct at the unit level.
Team passion at work was measured through Vallerand et al.’s (2003) measurement scale, also implemented by Ho et al. (2011), and reworded at the team level. This is a six-item Likert-type scale, ranging from 1 (strongly disagree) to 7 (strongly agree) (i.e., “My team is completely taken with this activity”). The principal component analysis showed that the six items loaded satisfactorily onto one factor. ICC1 and ICC2 values were .44 and .87, respectively, and the median level of rWG(J) was .89, ranging from .83 (strong) to .92 (very high), which supports data aggregation at the unit level. The scale’s α reliability was .899.
Individual passion at work was measured through Vallerand et al.’s (2003) measurement scale used for the team level, and reworded at the individual level. This is a six-item Likert-type scale, ranging from 1 (strongly disagree) to 7 (strongly agree) (e.g., “This activity is in harmony with the other activities in my life”).
Team performance was measured through the three-item Goodman and Svyantek (1999) scale, which ranged from 1 (strongly disagree) to 7 (strongly agree), adapted and reworded at the team level for both in-role (e.g., “My team performs all the functions and tasks demanded by the job”) and extra-role performance (e.g., “My team performs roles that are not formally required but which improve the organizational reputation”), and altruism (“My team helps colleagues when they have too much work to do”).
Team resilience was measured with a scale composed of seven items, which ranged from 1 (strongly disagree) to 7 (strongly agree), each of them based on one of Mallak’s (1998) principles for implementing resilience in organizations, for example, perceive experiences constructively, perform positive adaptive behaviors, and develop tolerance for uncertainty. Conversely to previous measures of team resilience (see, for example, West et al., 2009), this scale was developed specifically referring to teams in an organizational context. A sample item is “In difficult situations, my team tries to look for the positive side.” ICC1 and ICC2 values were .59 and .86, respectively, and the median level of rWG(J) was .80, ranging from .79 (strong) to .91 (very high), which supports data aggregation at unit level.
Individual performance was measured by means of the three-item Goodman and Svyantek (1999) scale, which ranged from 1 (strongly disagree) to 7 (strongly agree), including in-role (i.e., “I perform all the functions and tasks demanded by the job”) and extra-role performance (i.e., “I perform roles that are not formally required but which improve the organizational reputation”).
Individual resilience was measured using the three-item resilience subscale from the Psychological Capital Questionnaire (PCQ 12), which is a reduced version of the original scale developed by Luthans et al. (2007). Employees were asked on a seven-point Likert-type scale (i.e., “I can get through difficult times at work because I’ve experienced difficulty before”), where 1 corresponds to strongly disagree and 6 to strongly agree. Appendix I shows the details of the mesasurement scales.
Analysis
We followed a two-step approach as suggested by Gerbing and Anderson (1988) to check the theoretical model. First, exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were used to check the psychometric properties of the measurement scales. Then, we performed an ordinary least squares (OLS) regression-based analysis using SPSS to check T1 shared leadership at team level on T2 team outcomes, mediated by T2 passion at work at team level. Next, a multilevel analysis was conducted through hierarchical linear modeling (HLM). The direct and mediated cross-level effects of T1 shared leadership at team level were assessed on each of T2’s individual job outcomes, as mediated by T2 team passion at work and individual passion at work. Finally, the robustness of the results was checked by means of the Monte Carlo test using R software (Hofstede & Hofstede, 2005).
Results
Preliminary analysis and psychometric properties
EFA was performed to determine the dimensionality of all the scales. Cronbach’s α coefficients were also used to determine the reliability of the instrument. Factor loadings equal to 0.40 or greater are considered basically significant (Hair et al., 2018). The results show that the internal consistencies revealed by the scales were good, and the correlations exhibited significant direct connections between all measures. Table 2 shows factor loading and Cronbach’s α, and Table 3 shows means, standard deviations, and correlations.
Principal component analysis (with varimax rotation) loadings.
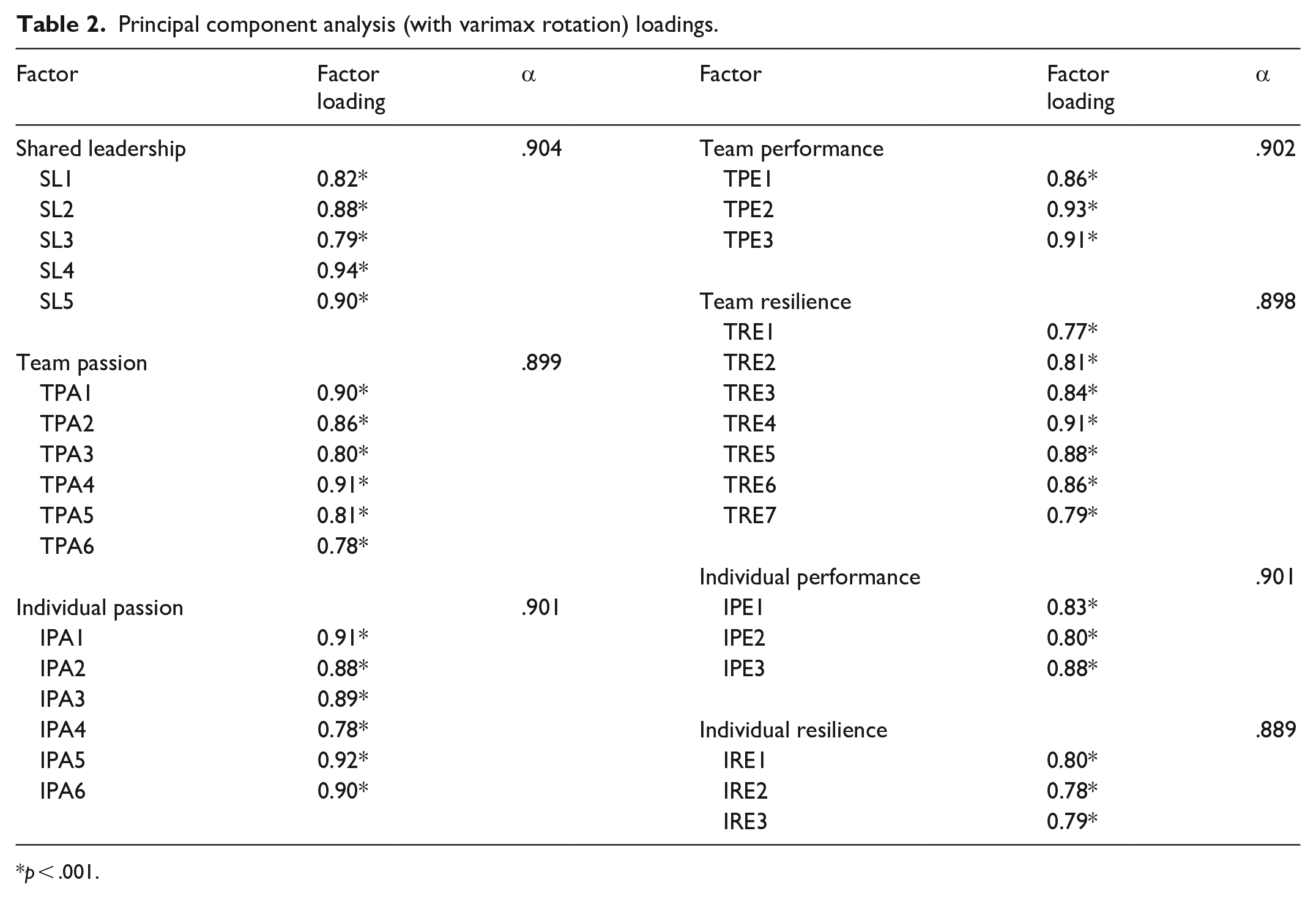
p < .001.
Means, standard deviations, and correlations.
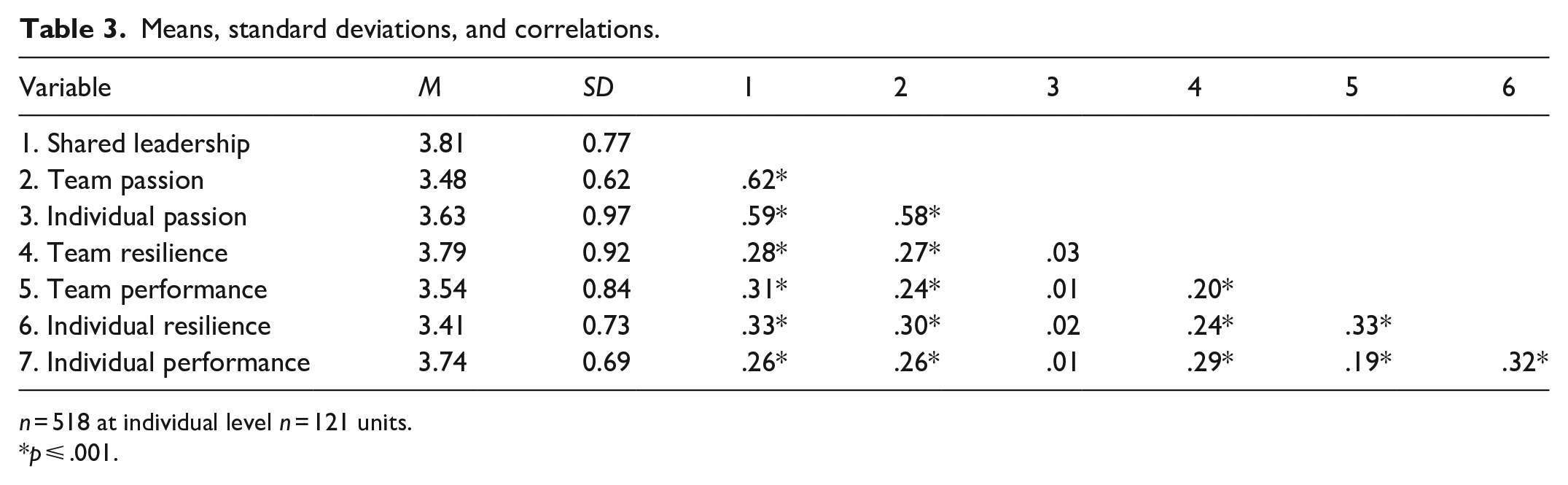
n = 518 at individual level n = 121 units.
p ⩽ .001.
CFA was performed to determine construct dimensionality, content, and convergent and discriminant validity (Gatignon et al., 2002; Gerbing & Anderson, 1988).
First, the one dimensionality of the measurement scales of all the measurement scales was checked. Table 4 shows the correct fit of the measurement scales. The p value of the chi-square statistic was below the significance level value of 0.05 for all the measurement scales. The other indicators confirmed the correct dimensionality of the constructs.
Fit values of the measurement scales.
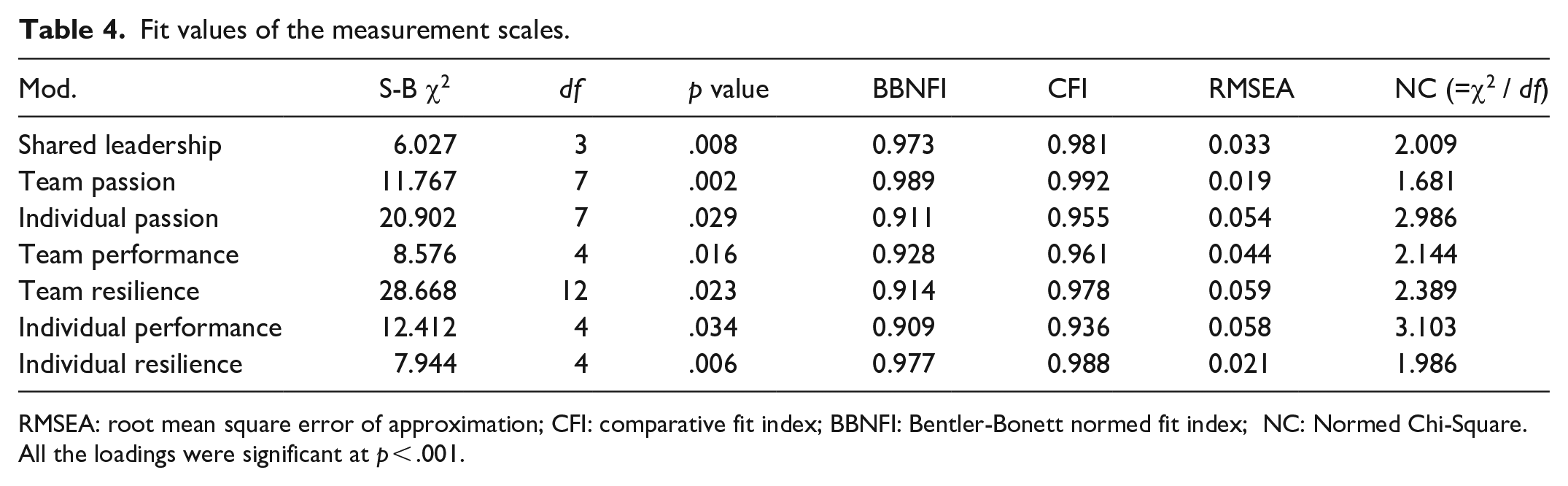
RMSEA: root mean square error of approximation; CFI: comparative fit index; BBNFI: Bentler-Bonett normed fit index; NC: Normed Chi-Square.
All the loadings were significant at p < .001.
Content validity can be confirmed when the scale items replicate the construct. All the measurement scales were based on previous empirical research, as well as strong literature background, which allows us to confirm the existence of content validity.
Convergent validity was evaluated by means of the Bentler-Bonett normed fit index (BBNFI) indicator obtained in the CFA. The BBNFI values are above 0.90, and the factorial loads for each construct are above 0.4, which confirms convergent validity (Hair et al., 2006).
Discriminant validity was evaluated by analyzing all possible pairs of constructs in a series of two-factor CFA models (Bagozzi & Phillip, 1982). First, the coefficient phi was constrained to unity and then freed. A chi-square difference test was then performed, and in all the cases, the critical value (Δχ2 > 3.84, p value < .05) was exceeded in all cases.
Common method variance
We followed Podsakoff et al. (2003) recommendations to keep questions simple and specific. We tested the questionnaire among a small sample of 15 physicians, to confirm they understood the meaning of each question perfectly. In addition, a CFA Harman’s single-factor test was run to check for common method biases. The full measurement model was compared to an alternative model with all the indicators loading onto a single factor. The results showed a poor fit in the single-factor model (χ2 = 3,072.376, df = 493, Bentler-Bonett normed fit index [BBNFI] = 0.608, Bentler-Bonett nonnormed fit index [BBNNFI] = 0.598, comparative fit index [CFI] = 0.614, root mean square error of approximation [RMSEA] = 0.144, χ2 / df = 6.232)
Hypothesis testing
H1a suggested a positive effect of T1 shared leadership at team level on T2 team resilience, mediated by T2 passion at work at team level. OLS regression showed a positive and significant mediation effect of T2 passion at work at team level, in the relationship between T1 shared leadership at team level and T2 team resilience (H1a) (β = .44, p < .01). At the same time, the relationship between T1 shared leadership at team level and T2 team resilience was not significant (β = .06, p = .48).
Therefore, T2 passion at work at team level fully mediated the relationship between T1 shared leadership at team level and T2 team resilience, thus supporting H1a.
H1b suggested a positive effect of T1 shared leadership at team level on T2 team performance, mediated by T2 passion at work at team level. OLS regression revealed a positive and significant mediating effect of T2 passion at work at team level, in the relationship between T1 shared leadership at team level and T2 team performance (H1b) (β = .38, p < .01). However, the relationship between T1 shared leadership at team level and T2 team performance was not significant (β = .08, p = .59). Therefore, H1b was supported, as T2 passion at work at team level fully mediated the relationship between T1 shared leadership at team level and T2 team performance.
Tables 5 and 6 show the results of OLS regression for H1a and H1b.
Ordinary least squares (OLS) regression results of team resilience (n = 121 units).
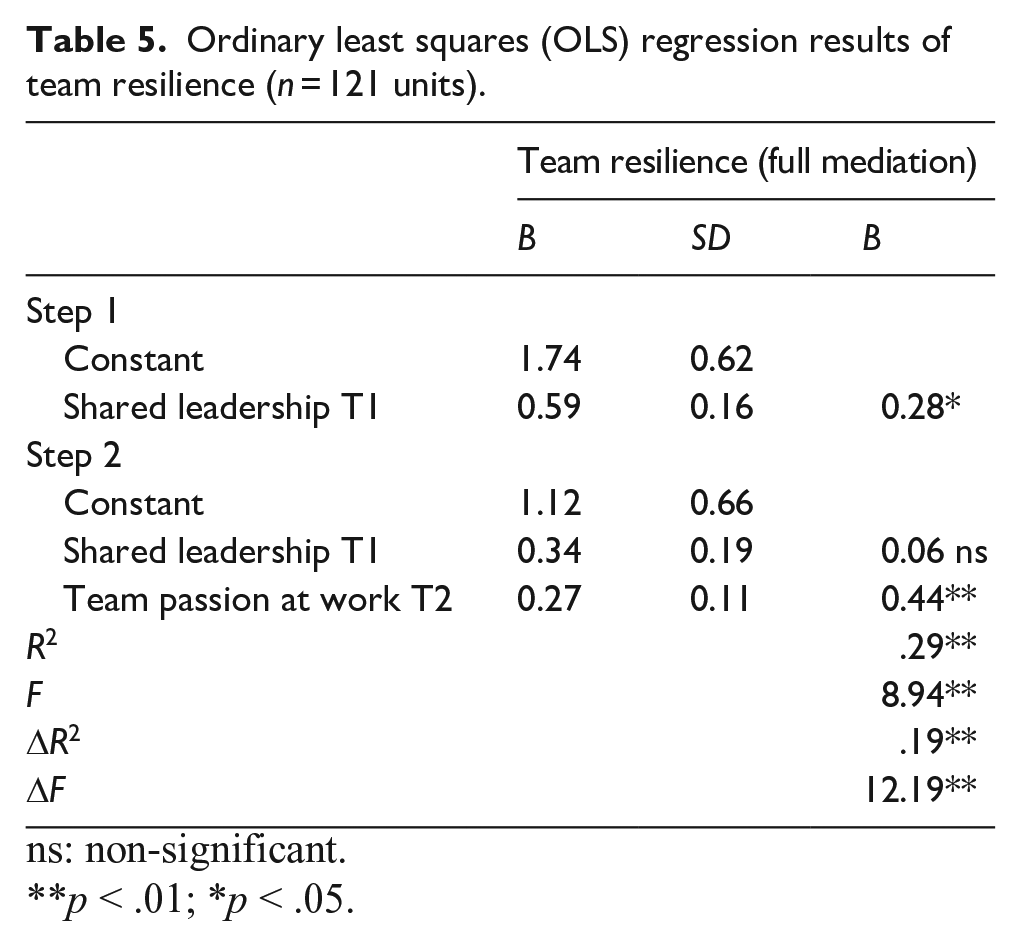
ns: non-significant.
p < .01; *p < .05.
Ordinary least squares (OLS) regression results of team performance (n = 121 units).
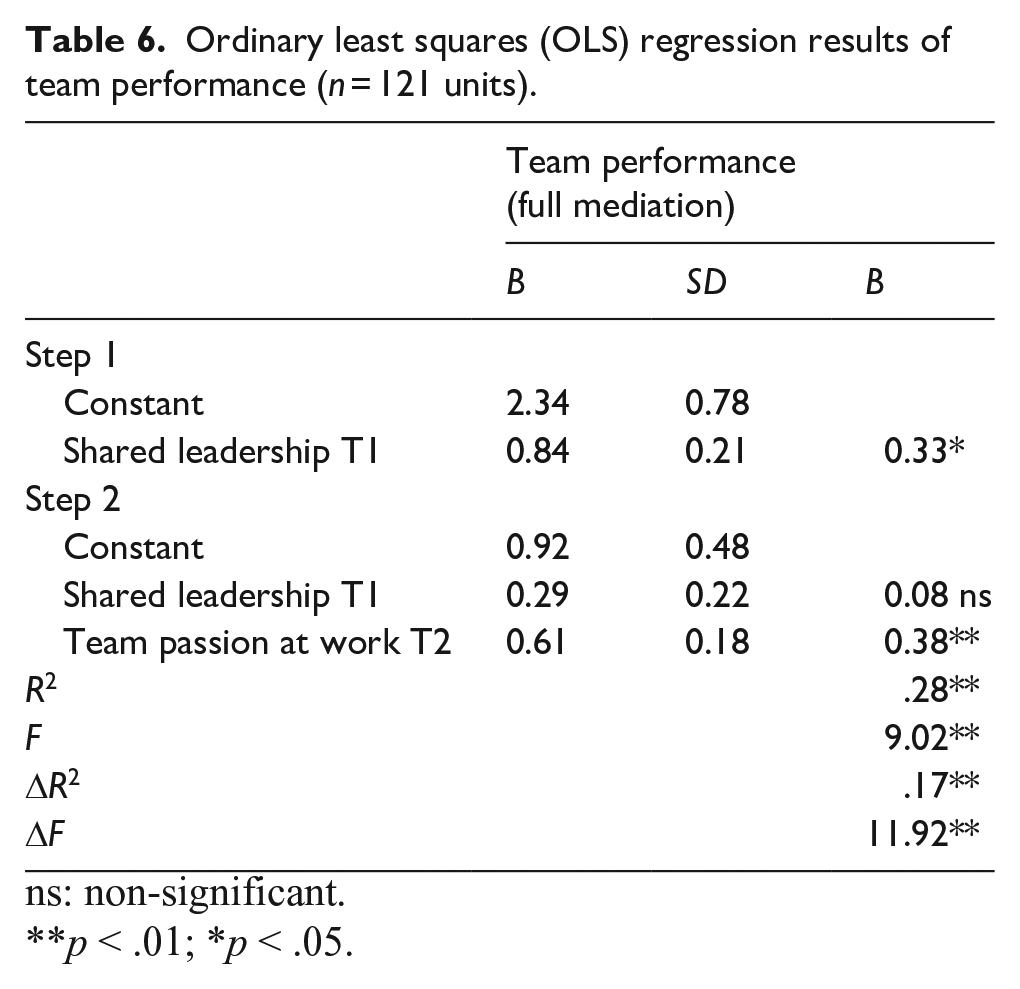
ns: non-significant.
p < .01; *p < .05.
H2a argues that the cross-level impact of T1 shared leadership at team level on T2 resilience at individual level is mediated by T2 passion at work at team level. HLM with random slopes revealed a significant mediating effect of T2 passion at work at team level in the relationship between T1 shared leadership at team level and T2 resilience at individual level (γ = 0.31, p < .01).
H2b states that the cross-level impact of T1 shared leadership at team level on T2 performance at individual level is mediated by T2 passion at work at team level. A significant mediation effect was found for T2 passion at work at team level in the relationship between T1 shared leadership at team level and T2 performance at individual level (γ = 0.39, p < .01). Thus, H2a and H2b were confirmed.
However, HLM with random slopes revealed a significant effect of T1 shared leadership at team level on T2 resilience at individual level (γ = 0.48, p < .01) (Table 7). In addition, the effect of T1 shared leadership at team level on T2 performance at individual level was also significant (γ = 0.62, p < .01). However, no significant mediation effect was found for T2 passion at work at individual level in the relationship between T1 shared leadership at team level and T2 performance at individual level (γ = 0.27, p > 0.05). Similarly, T2 passion at work at individual level did not mediate the relationship between T1 shared leadership at team level and T2 resilience at individual level (γ = 0.23, p > 0.05).
Hierarchical linear modeling (HLM) results of the relationship between shared leadership at team level, passion at work at team level, and individual- and team-level resilience and performance (individual level n = 518, team level n = 121 units).
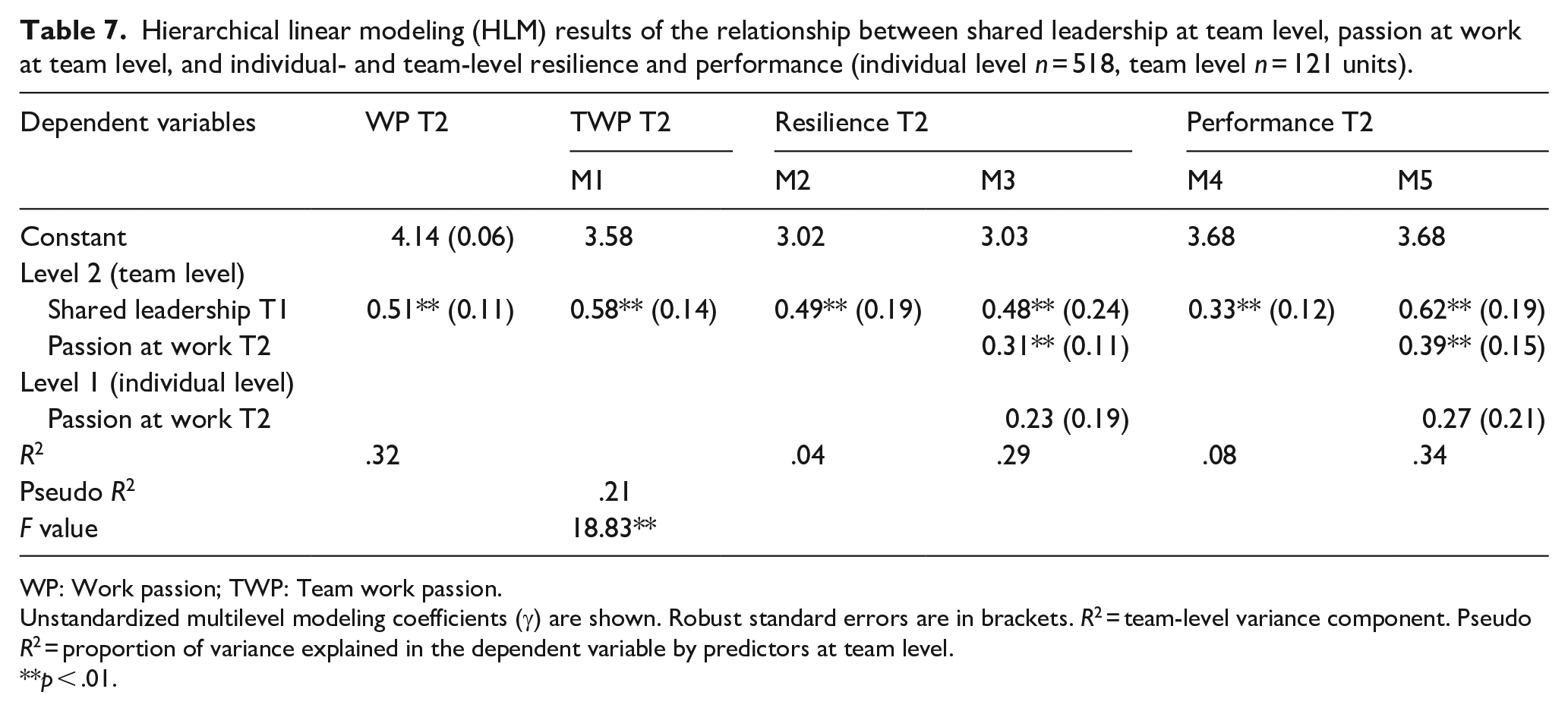
WP: Work passion; TWP: Team work passion.
Unstandardized multilevel modeling coefficients (γ) are shown. Robust standard errors are in brackets. R2 = team-level variance component. Pseudo R2 = proportion of variance explained in the dependent variable by predictors at team level.
p < .01.
To check the robustness of the mediating effects of team passion at work and passion at work, a Monte Carlo test was performed using R. Table 8 shows the results.
Team-level and cross-level direct and mediated effects (N = 518 at individual level; n = 121 units at team level).
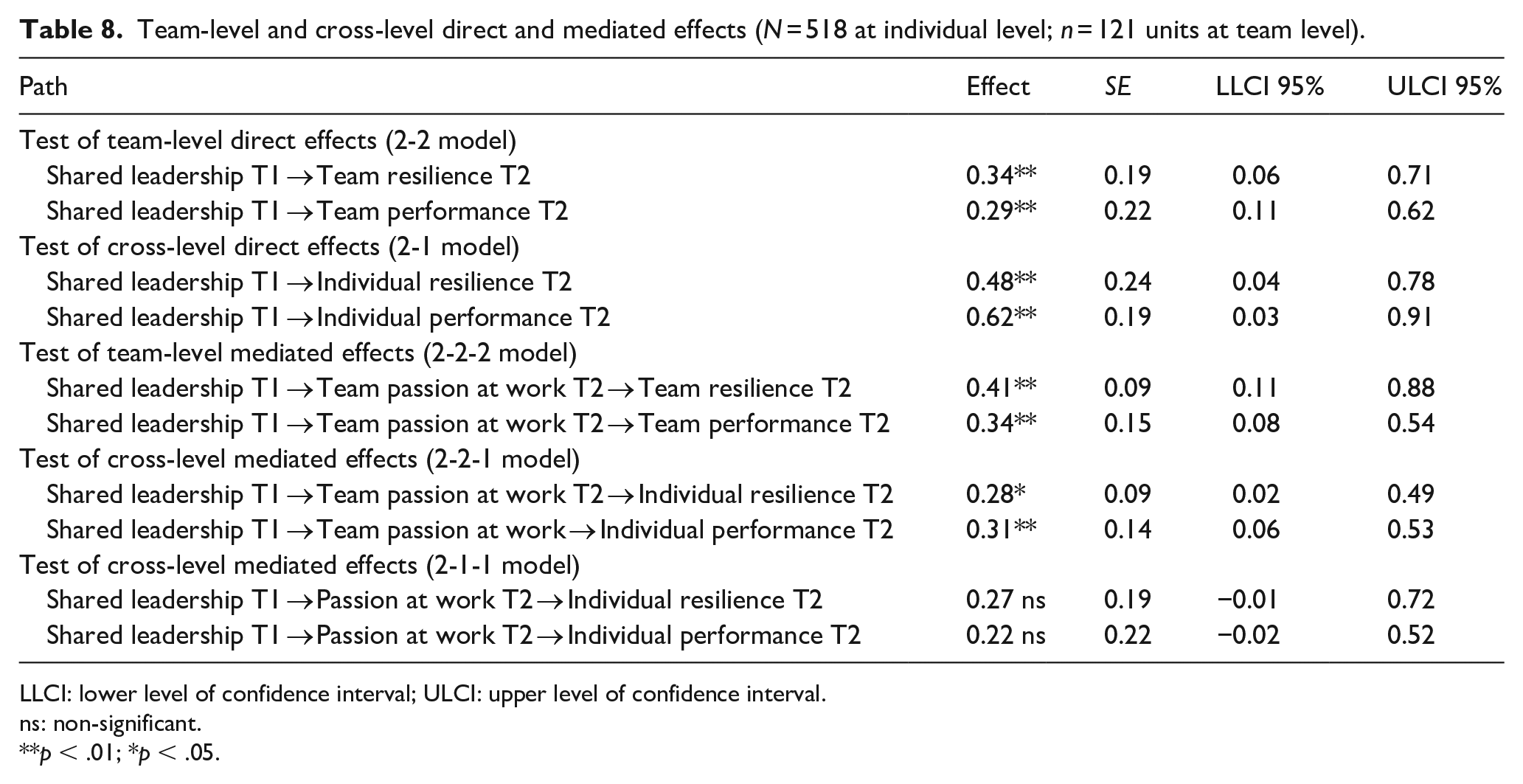
LLCI: lower level of confidence interval; ULCI: upper level of confidence interval.
ns: non-significant.
p < .01; *p < .05.
The Monte Carlo test yielded a significant cross-level mediating effect of T2 passion at work at team level on the relationship between T1 shared leadership at team level and T2 resilience at individual level (effect = 0.28, 95% confidence interval [CI] = [0.02, 0.49]). However, no significant mediating effect of T2 passion at work at individual level was found on the relationship between T1 shared leadership at team level and T2 resilience at individual level (effect = 0.27, 95% CI = [−0.01, 0.72]).
In addition, the results indicated a significant cross-level mediating effect of T2 passion at work at team level on the relationship between T1 shared leadership at team level and T2 performance at individual level (effect = 0.31, 95% CI = [0.06, 0.53]). By contrast, T2 passion at work at individual level did not mediate the relationship between T1 shared leadership at team level and T2 performance at individual level (effect = 0.22, 95% CI = [−0.02, 0.52]).
The results from the Monte Carlo test provided support to the OLS regression and HLM analysis, thus confirming the robustness of the results.
Discussion
Today, humanity is at threat from COVID-19, and physicians are suffering tremendous psychological damage due to work overload, lack of resources, exhausting working days, the constant risk of contagion, and experiencing the continuous death of COVID-19 patients. One of the negative consequences of the pandemic for this group is a lack of enthusiasm and attachment to their jobs. The main objective of this research is to offer a model to restore passion in the medical profession. The study reveals that the path to engage physicians with their job again involves shared leadership and passion at work. The public health care system is bearing the weight and cost of handling the pandemic, not only in economic but also in psychological terms. Public resource managers have not looked after physicians, and we should not let them throw in the towel. A re-enchanted workplace would renew physicians’ feelings of being positively connected to their job through passion at work.
This research contributes to the literature on leadership and healthy organizations by exploring the mechanism underlying the relationship between shared leadership and job outcomes (i.e., resilience and performance) namely, passion at work, among physicians in an unprecedented health emergency context. Shared leadership is considered to be a key job resource to cushion the negative effects caused by COVID-19, and the medical profession requires continuous interaction between physicians.
The novelty of this research resides in the fact that passion at work is introduced as a mediator to broaden our knowledge on how shared leadership impacts resilience and performance from a multilevel approach. This approach sheds light on the power of passion in a collective form for physicians on both team and individual job outcomes under highly demanding work conditions. In particular, we fill the gap pointed out by Moeller (2014), regarding the lack of models concerning the predictors and outcomes of passion. In addition, and in response to the call made by Pollack et al. (2020), this research provides evidence on how passion develops and is amplified for a specific work role, namely, the medical profession in the public sector, and how passion predicts work-specific outcomes, particularly, resilience and performance.
Theoretical contribution
The findings of this research are important for several reasons. First, the results support the explanatory power of the SDT to re-enchant highly demanding and challenging workplaces, which is the case of public health care in the midst of an unprecedented pandemic. Second, the results show that team resilience can be fostered through shared leadership, by means of team passion. Therefore, our study contributes to the emerging field of research on resilience at team level, which explores how groups or teams react positively to critical circumstances (Stoverink et al., 2020). At the time of writing this article, global COVID-19 cases are in excess of 25 million, and many countries are reporting record infections. Given this situation, there is an urgent need to improve our knowledge on how to build up team resilience in public health care or, in other words, how to adapt to and recover from high-risk situations. The effectiveness of both shared leadership and team passion might be explained because the effect of job resources on positive outcomes is more powerful under highly demanding circumstances, and this is the case of specialized medical units. This finding is in line with Bakker and Demerouti (2007), who argued that the interaction of job demands with job resources influenced team resilience. Medical work units treating COVID-19 patients include physicians from different specialties, who have a lack of knowledge and experience in this area in a risky and uncertain context. Physicians therefore require mutual support from their colleagues together with medical autonomy and professional capacity. Shared leadership creates the conditions to increase physicians’ autonomy, competence, and relatedness.
We also advance on previous research on team resilience by focusing on specialized medical units in public hospitals, as little research has focused on specific work contexts (Pollack et al., 2020). Furthermore, while prior studies highlighted the role of team coordination in explaining team resilience (Meneghel et al., 2016), we provide a more holistic approach through the concept of shared leadership.
By the same token, a pending question on team resilience research is related to the role of passion at work at team level. In this regard, health care professionals work in teams to effectively provide the highest quality medical care (Rosen et al., 2019). As professions like law and academia, medicine is a closed collegial, expert occupation, involving a degree of autonomy, expertise, and self-regulation (McGivern et al., 2015), which is crucial to solve complex problems through a broad knowledge base. Teams with shared leadership can obtain empowerment and autonomy either from the chosen leader or from the self-managed team (Dumaine, 1994). However, given the intensity and extreme conditions in hospitals, where death and family suffering is a constant, a working group can only become stronger when autonomy, competence, and relatedness lead to shared passion at work among the work unit members.
In contrast, hierarchy can constrain the proactive communication required for recovery from error (Sutcliffe et al., 2004). All the signs are that shared leadership is an effective tool to enhance mutual feelings of passion among physicians working in the same unit, in turn strengthening a common capability to successfully address adversity, namely, team resilience.
Yet the findings not only show that team passion explains team resilience. It also explains team performance. Given its importance to organizational functioning, the antecedents of job performance have been widely examined. However, there are few studies addressing the effect of passion at work on performance (Chummar et al., 2019), and even fewer in the public health care context and at team level. As a second contribution, this study reveals that a high level of team passion is an effective channel to explain the effect of shared leadership on improved team performance. This finding is particularly relevant because it confirms that it is a team’s identification with a task which boosts the achievement of team goals (Ho et al., 2011). This may well provide support to argue that passion reinforces its effect at team level, when employees share their emotions, since the intensity and immersion experienced by physicians increase. When group members interact together, they build social resources which improve performance (Peñalver et al., 2019), but when these relationships take place in a climate of mutual passion at work, the team becomes stronger and better able to achieve its objectives. Physicians need an extra dose of positivity and energy. When they arrive home, they are physically and mentally exhausted and look for support at home or a chat with friends. This research enables us to conclude that the shared feeling of passion at work is fundamental for them to bounce back from adversity.
As a third contribution, the multilevel analysis reveals the power of the shared feelings of passion on team and individual job outcomes. The results show a positive relationship between shared leadership at team level and individual job outcomes as mediated by passion at work at team level. Thus, this study provides evidence that shared leadership and passion at work at team level are crucial in eliciting not only team but also desirable individual outcomes, namely, resilience and performance at individual level. In this vein, this study draws attention to the scarcely explored connections between passion at work, resilience, and performance at different levels of analysis.
Individual resilience, as a capacity that can be developed (Hartmann et al., 2020), can emerge as a consequence of the interaction between shared leadership and passion at work at team level. Job resources such as strong professional networks promote individual resilience among physicians (Jensen et al., 2008). By experiencing positive emotions, people broaden their momentary thought-action repertoire, in turn enhancing individual resilience (Cameron & Brownie, 2010). However, the effects of job resources and positive emotions on individual resilience have scarcely been explored. To fill this gap, we provide evidence on the positive effect of passion at work at team level on individual resilience.
In addition, positive appraisals of work environment characteristics, namely, shared feelings of passion at work, result in positive work intentions to use discretionary effort and improve performance (Thibault-Landry et al., 2018). Studies have found that these intentions derived from psychological processes are reliable predictors of both in-role and extra-role behaviors (Dubinsky & Skinner, 2002).
However, in contrast to our expectations, passion at work at individual level did not mediate the relationship between shared leadership and individual job outcomes. This finding is striking because we expected the JD-R model to predict improved performance (Gross et al., 2019) and increase levels of resilience as a result of additional job resources and positive attitudes (i.e., shared leadership and passion at work at individual level). The results show that team-level shared leadership fosters feelings of being competent, autonomous, and empowered, thus boosting passion at work at individual level. However, passion at work at individual level does not seem to be sufficient to improve individual resilience, at least in a turbulent and highly demanding context such as the medical profession in specialized units. Therefore, the social psychological theories of social norms, modeling, and emotional contagion are relevant in terms of the importance of passion at work at team level. Team members’ passion has emerged as the driving force for individuals’ to flourish in adverse circumstances. This is an interesting finding as it reveals that physicians need extra mutual support and a high sense of shared identification, as well as an extra dose of motivation and commitment, namely, passion at work at team level, to be more resilient and improve their performance. This makes sense in the critical situation they are currently experiencing at work, where the work unit becomes a fundamental element to overcome tensions and work demands. In this sense, by sharing attitudes and behaviors, individuals become more vigorous (Bakker & Xanthopoulou, 2009), and shared positive emotions increase social resources and performance (Peñalver et al., 2019). In contrast, an individual approach to passion does not affect individual resilience. This might be explained by the influence of other variables in the process whereby individual passion leads to individual resilience. Furthermore, additional reinforcement of job resources could be necessary in this regard.
Similarly, passion at work at individual level did not mediate the effect of shared leadership on individual performance. One could argue that ties in a context of collaboration are fundamental to achieve challenging objectives with limited resources, and a passionate team helps to tackle work intensification and increased pressure. In this way, the social psychological theories of social norms and modeling have a strong explanatory role: It is the team which infuses specific motivation and energy to achieve ambitious, complex objectives. The medical context involves continuous interaction between physicians because they need knowledge and support from other colleagues. The results show that physicians need a shared sense of passion at unit level, rather than passion at individual level.
In sum, shared leadership and team passion are disclosed as being essential to re-enchant public health care. Leaders are responsible for the performance and humanization of organizations (Kelemen et al., 2020), and those who share their role and promote autonomy, competence, and relatedness, are particularly effective in re-enchanting physicians’ workplace. The synergistic effect of shared leadership and team passion on team and individual job outcomes is due to the complementarity of resilience and performance, which points to a “mutual gains” approach, in accordance with Guest’s (2018) view.
To end with, we would like to recall the words of Vallina (2005), who paraphrasing Morin (2000), said that the human being, in the 21th century, must abandon the unilateral vision defined by rationality (Homo sapiens), technique (Homo faber), utilitarian activities (Homo economicus), and compulsory needs (Homo prosaicus). The human being is complex, and he carries itself in a bipolar way the antagonistic characters of sapiens et demens (rational and delirant), faber et ludens (worker and playful), empiricus et imaginarius (empirical and imaginary), economicus et consumans (economic and dilapidator), prosaicus et poeticus (prosaic and poetic).
Implications for practice
This study also provides a number of potential applications to encourage hospital managers to give particular consideration to teams’ passion at work. First, HR managers and heads of medical units need to delegate leadership assignments to team members, encouraging physicians to advise each other and be proactive. In addition, heads of medical units should create fluid team-based job descriptions, clearly defining employee roles and responsibilities. Shared leadership makes team members more confident and makes them value guidance from their peers (Ali et al., 2020), which fosters team passion.
In addition to this, our results indicate that team passion matters in encouraging individual job outcomes. In this vein, organizations should take into consideration that team members’ passion fires up individuals’ energy to tackle challenging circumstances and recover successfully from them, which boosts proactive behavior and individual performance. For this reason, organizations should promote the internalization of tasks in which individuals have the freedom to decide on the amount of time and effort devoted to their passion. Heads of medical units should seduce and attract employees in such a way that they pursue and love their jobs.
We urge hospitals to re-enchant their physicians and make public hospitals a better place to work. Physicians are not heroes, but people who deserve resources, care, and especially a re-enchanted workplace. Our lives are in their hands. Let this research serve as a tribute to all physicians dealing with COVID-19 patients.
Limitations and future research
As with all research, this article is not without limitations. First, both individual and situational moderators of passion should be considered, as suggested by Curran et al. (2015). Some moderating variables in the relationship between shared leadership and team passion could include self-efficacy, happiness at work, organizational culture, task characteristics, and team diversity, as they have the potential to influence interpersonal interactions and team effectiveness (Avolio et al., 2014). Another interesting avenue for future research relates to the “dark side” of passion. At present, little research has explored how and when passion has negative effects on employees or organizational outcomes. A more balanced approach including the potential dysfunctions of passion would provide additional opportunities for research. In addition, we also call for an examination of the capacity of other constructs over and above passion at work in predicting work-specific outcomes. Moreover, control variables could be examined in future studies, to check how sociodemographic aspects, such as gender and age, or organizational variables, such as tenure, influence (or not) resilience and performance. Likewise, given that passion at work at individual level was not significantly related to individual job outcomes, this suggests the presence of unidentified moderators that might boost or suppress the effects of passion at work at individual level or multiple mediating effects that neutralize each other. Finally, future research could carry out a controlled intervention, to find out how exactly team passion unfolds and how it can be enhanced.
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.