
Abstract
A 7-month-old girl had been suffering from progressively deteriorating pneumonia despite getting multiple courses of broad-spectrum antibiotics as well as anti-fungal drugs for adequate duration. To find out the cause behind this deterioration, the patient underwent thorough clinical and relevant laboratory evaluation including chest radiology & imaging, screening for primary immune deficiency disorders (PID), cystic fibrosis, tuberculosis, invasive fungal pneumonia, congenital heart disease, covid pneumonia, TORCH etc. but failed to solve the mystery. Upon further detailed re-evaluation, it was discovered that the child had a history of being forcefully fed lentil-based khichuri (a rice-lentil mixed dish) during her weaning process and diagnosis was finally confirmed as hypersensitive pneumonia due to lentil aspiration by a high level of IgG, specific to lentil antigen. Treatment was commenced with prednisolone resulting in significant improvement in her clinical and radiological condition within 72 hours.
Keywords
Introduction
Hypersensitivity pneumonia, also called extrinsic allergic alveolitis, is a rare immune-mediated interstitial lung disease in children, resulting from repeated exposure to organic or inorganic antigens, and less commonly fungi and drugs like methotrexate with varying clinical manifestations. 1 Hypersensitive pneumonitis (HP) is a less commonly prevalent but fatal pediatric pulmonary condition affecting an estimated 4 in 1 million children. 1 From the first clinical descriptions in 1932 noting symptoms in workers exposed to fungus on Maple bark and moldy hay or lentils, numerous exposures causing HP have been reported globally.2,3
HP primarily affects the distal airways of the lungs and is often triggered by repeated exposure to antigens, animal proteins, chemicals, or microbes in the environment. 4 The susceptibility of a child to these environmental antigens is an immune-mediated phenomenon with T-cells, B-cells, and granulocytes playing significant roles. However, genetic factors contribute to an individual’s susceptibility to hypersensitivity toward these environmental factors. 4
In HP, initial exposure to the offending antigen triggers the immune complex-mediated (type III) hypersensitivity reaction. This subsequent continued exposure gives rise to a delayed (type IV) hypersensitivity reaction, an essential step in progression to fibrosis. 2 An early clinical diagnosis can greatly help to early initiation of treatment that may further help to reduce prolonged illness and complications. However, it’s not unusual for the diagnosis to be delayed. In this article, we present the details of a young infant suffering from hypersensitivity pneumonitis from lentil aspiration, who showed substantial improvement following glucocorticoid therapy and published here to serve as a useful reference and raise awareness among the pediatricians.
Case Summary
A 7-month-old girl was admitted to BIRDEM hospital, Dhaka, Bangladesh due to repeated instances of difficulty in breathing, low-grade fever, and a cough that had been occurring since she turned 6 months old. Notably, there was no suggestive history of tuberculosis, immunodeficiency or cystic fibrosis like recurrent loose stools, weight loss, skin abscess, sinopulmonary infections or infection at multiple sites. There was no risk factor for aspiration like Gastroesophageal reflux, structural defect like cleft palate/tracheoesophageal fistula, airway anomaly, impaired swallowing, developmental delay etc.
Upon admission, the patient was tachypneic, accompanied by intercostal, subcostal, and suprasternal retractions and arterial oxygen saturation level, was 88% measure by pulse oximeter (NT1D Vital Signs Monitor, Solaris Medical, USA) while breathing at room air. The general physical examination was unremarkable, upon further examination of the respiratory system; bilateral crepitation as well as wheeze was detected. No abnormalities were found during other systemic examinations.
Initial assessments of her condition, both clinically and through radiological assessments, revealed that she had bronchopneumonia. Chest X-ray (Figure 1) showed bilateral patchy consolidation with infiltrate with sparing of the lung bases suggesting bilateral interstitial pneumonia. The high-resolution CT scan (HRCT) of the thorax (Figure 2) revealed confluent areas of patchy opacities involving bilateral lung fields predominantly in hilar and para-hilar region, presence of air bronchogram, consistent with atypical pneumonia.
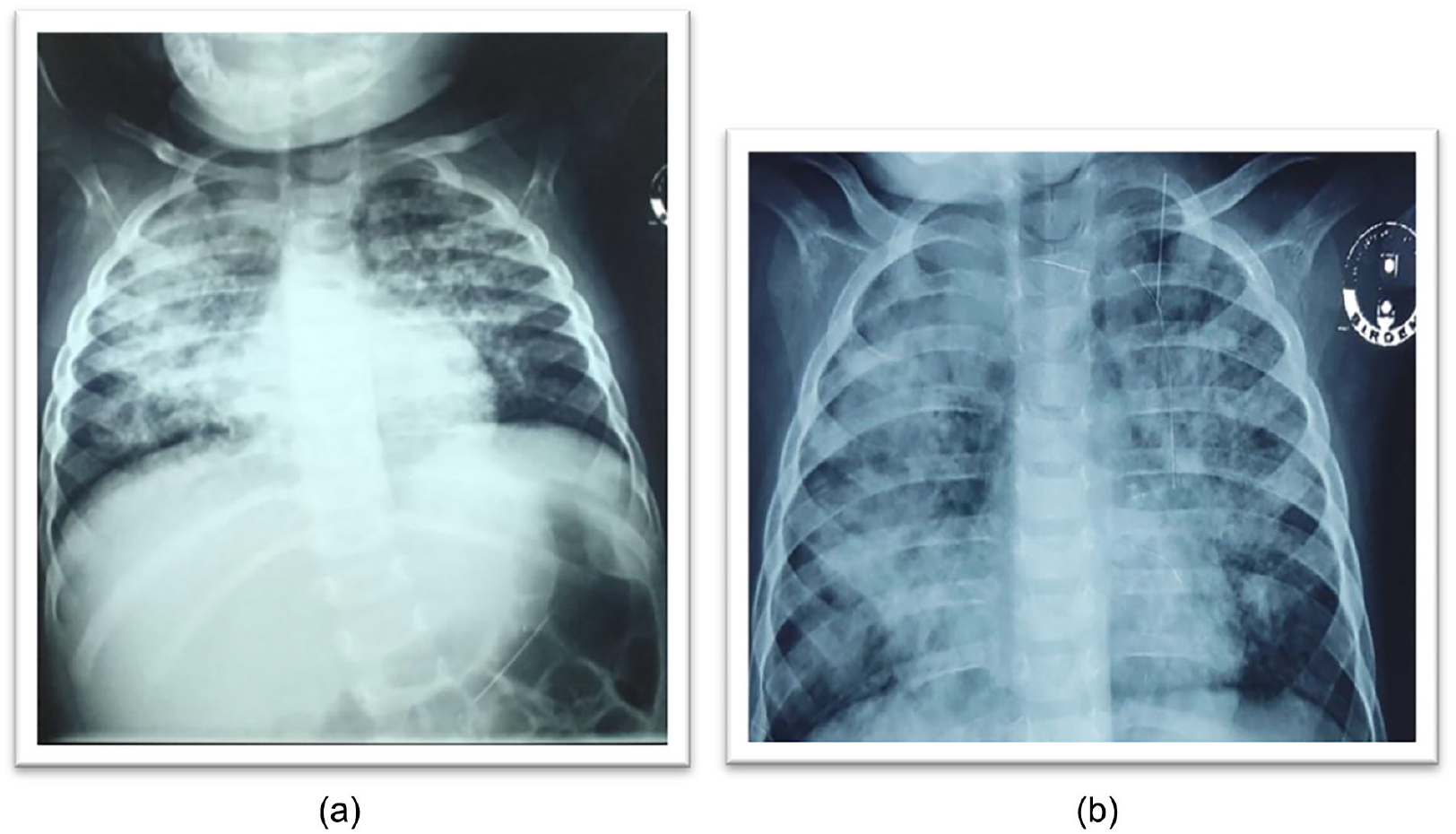
Both the chest x-rays a & b were done before starting prednisolone, 1 week apart and showed bilateral consolidation with infiltrates suggesting bilateral interstitial pneumonia. X-ray (b) is seen worser than x-ray (a), indicates progressive radiological deterioration.

High-resolution computerized tomography (HRCT) thorax showing confluent areas of patchy and nodular opacities and Ground glass opacity in periphery of the dense consolidation involving bilateral lung fields predominantly in hilar and parahilar region and air bronchogram.
The pediatric team conducted multiple investigations to determine the potential cause of the progressively deteriorating recurrent pneumonia, but none of them yielded useful results.
Complete blood count and PBF: Mild microcytic hypochromic anemia with hemoglobin of 10 g/dL, Total leukocyte count- 18.92 × 109/L, Neutrophil- 9.93 × 109/L (52.5%), Lymphocytes- 7.70 × 109/L (40.7%), Monocytes 1.09 × 109/L (5.8%), Eosinophils- 0.02 × 109/L (0.1%), Platelets- 391 × 109/L
Blood culture (bacterial and fungal): No Growth
Respiratory Viral PCR: None detected
The sweat chloride test was within normal limits at 20 mmol/L.
PID panel and Immunoglobulin profiles were within the normal limits.
Lymphocyte subset analysis (TBNK) was normal.
Gastric lavage for acid-fast bacilli and Mantoux test were negative.
Echocardiogram was normal
Rt PCR COVID 19 was Negative
Aspergillus Galactomannan test for fungal pneumonia was very weakly positive
TORCH Screening, was negative
She had history of recurrent hospitalizations with similar presentations in the past 1 month. During this admission, she was initiated on oxygen therapy, various broad-spectrum intravenous antibiotics, and anti-fungal medications. Unfortunately, despite receiving treatment with multiple courses of broad-spectrum antibiotics, there was continuous clinical and radiological deterioration (Figure 1).
Upon conducting a more detailed history taking and extending the field of re-evaluation with less common differentials of the case, it was revealed that the child had a history of being forcefully fed lentil-based khichuri (a rice and lentil dish) during the weaning process. This led us to suspect that her symptoms were likely due to hypersensitivity pneumonia caused by the aspiration of lentils. After numerous discussions with relevant pediatric consultants and extensive literature search, we eventually settled on a diagnosis of hypersensitivity pneumonia due to lentil aspiration and initiated a treatment plan involving oral Prednisolone only and stopped all other antimicrobials. The child demonstrated significant clinical and radiological improvement (Figure 3) after a few days of taking Prednisolone, weaned off oxygen, and was instructed to continue Prednisolone for 2 weeks. The diagnosis was finally confirmed by a high positive level of IgG specific to the lentil antigen of 4.70 mgA/L.

Chest x-rays (a) and (b) done after starting prednisolone showing progressive radiological improvement; (a) done 3 days after starting of prednisolone and (b) after 10 days of starting prednisolone.
The infant was discharged from the hospital with advice for follow up after completion of prednisolone, and to omit lentil in the diet.
Discussion
Diagnosing hypersensitivity pneumonitis (HP) due to lentil/other triggers can be challenging due to the variety of symptoms it presents, such as cough, fever, tachypnea, or respiratory distress. A retrospective study conducted in North India 3 found that the average age of onset of lentil/ food related hypersensitivity was 9 months, similar to our case, which corresponds to the time of weaning to a lentil based mashed rice. The study 3 also reported that chronic cough was the predominant symptom, along with shortness of breath, fever, vomiting, and wheezing. Physical examination revealed auscultatory fine crackles, while CT scans showed nodular opacities and consolidation in a majority of children. 3
In absence of confirmatory diagnostic test to diagnose hypersensitivity pneumonitis (HP) due to lentil, a history of exposure, respiratory symptoms, and high-resolution computed tomography (HRCT) findings become pivotal in the diagnosis. 5
HRCT findings can vary based on the stage of the disease for example (a) in acute stage the findings could indicate ground-glass opacification, patchy airspace opacities, and diffuse consolidations. (b) in chronic stage, these could include centrilobular nodules, lobular areas with a mosaic pattern, honeycombing, septal thickening, and traction bronchiectasis. 6
Other investigations that aid diagnosis of Lentil Hypersensitivity pneumonitis include Plain Chest Radiograph which may show patchy or diffuse airspace opacities, and rarely consolidations with sparing of the lung apices and bases. 6
Blood counts and metabolic panels are usually normal. Inflammatory markers such as erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are typically elevated. 2
Serum IgG antibodies against potential organic antigens can be assayed in patient’s serum. A positive IgG antibody only indicates exposure and does not confirm diagnosis, however they can be useful as supportive evidence for HP. 7 Pulmonary Function Testing (PFT)/spirometry often reveal a restrictive pattern. 2 Although a provocation test using the suspected antigen is considered the gold standard for diagnosis, it is currently only available for research purposes. Bronchoalveolar lavage and lung biopsy can provide additional diagnostic information but may not always be necessary when there is a clear history of exposure and typical radiological findings. 8
If not diagnosed early and treated promptly as detailed above, HP can progress to pulmonary fibrosis and progressive respiratory failure. 2
The primary mode of treatment is complete avoidance of the offending antigen, combined with glucocorticoids to hasten initial recovery if severity deems necessary. 4
In the case discussed, the patient’s clinical presentation such as cough, resting tachypnea or chest retraction, failure to thrive, history of forceful feed with lentil leading to aspiration, along with the presence of typical radiological findings and a remarkable response to glucocorticoid treatment, were crucial in establishing the diagnosis.
Conclusion
Hypersensitivity pneumonia (HP) caused by lentil aspiration is a relatively rare pulmonary condition in children but is an important cause of HP in infants of weaning age with force-feeding practices. However, it should be considered when clinical symptoms of pneumonia and radiological features of interstitial pneumonia persist despite standard treatment. Thorough history, clinical assessment and careful evaluation of x-ray chest and high-resolution chest imaging play a vital role in promptly and precisely diagnosing this condition. Prospective studies with larger sample size are needed to identify aspirated antigens which cause HP in aspiration prone children.
Footnotes
Acknowledgements
Prof ARM Luthful Kabir, Professor, Dr Sudipta Roy, Associate Professor, Department of Pediatrics, Ad-Din Womens Hospital, Moghbazar, Dhaka; Dr Nurun Naher, Consultant, Pediatric ICU, Evercare Hospital, Dhaka Bangladesh
Author Contributions
Type specific contribution of authors:
Project Conception and Investigators: MAHM, PP, TA
Data acquisition: MAHM, JN, PP, TA, SK, SJ
Data Management and Analysis: MAHM, JN, PP, NT, TA, SK, SJ
Data interpretation and manuscript writing: MAHM, PP, NT, TA, SK, SJ, MJC
Manuscript revising & further editing: MAHM, NT, MJC
Manuscript finalizing & submission: MAHM, NT, MJC
Accountability: MAHM, NT, MJC
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Ethical statement
The mother of the baby has provided an informed consent to use the medical information of her child for publication. As the case report was prepared to improve the quality of patient care in the respective hospital, the ethical clearance was not required.