
Abstract
Objectives. Extremes of maternal age at childbirth may influence child nutritional outcomes, but this is under-researched in Roma populations. Methods. The study was a secondary data analysis of Multiple Indicator Cluster Surveys for Serbian Roma settlements and included 2564 children aged 0 to 59 months. Results. About 19% of children were stunted, 9% underweight, 16% were unwanted and born with a low birth weight. Logistic and linear regressions show that maternal age at childbirth had no association with either nutritional or growth outcomes of Roma children (P > .05). Instead, child characteristics: being born as a boy, low birth weight, unwanted, younger age, and maternal characteristics: short birth spacing, higher parity and low socioeconomic status were associated with children’s malnutrition. Conclusion. Maternal age at childbirth per se does not increase the chances of poor child health outcomes, as the risks seem to be related more to individual child and maternal characteristics and maternal behavioral patterns.
Introduction
Childhood growth deficiencies (low height-for-age or weight-for-height) such as stunting, an indicator of chronic malnutrition, and low weight-for-age, or being underweight, represent risk factor for overall morbidity and mortality, influencing health, growth and development from early age well into adulthood. 1 Growth faltering is regarded to be a result of complex interaction between environmental, socioeconomic, and maternal and child characteristics. 2 In regard to maternal factors, the determinants of childhood nutrition and growth include maternal anthropometry, literacy and education, and access to improved sanitation, while risk factors at the level of the child include age (birth order), sex, birth spacing and breastfeeding. 3
Additionally, there is increasing interest in the effects of maternal age at childbirth on offspring health outcomes. 4 Early (≤19 years), but also late (≥35 years), maternal age may be associated with adverse birth and child outcomes owing to biological risk predicted for extremes of reproductive age. The costs associated with low age at marriage may also have bearing upon aspects of the health and well-being of both mother and child. 5
In most developed countries, maternal age at childbirth has continued to rise with the result that the majority of children are now born to mothers aged 30 years and over. 6 In low-and -middle-income countries, by contrast, childbirths by adolescent mothers remain high, with early marriage (first marriage before 18 years) being the predominant factor influencing fertility. 7
Studies examining the growth and nutritional outcomes in the offspring associated with maternal age at childbirth are limited, while those on the association between maternal age at birth and offspring health outcomes have shown mixed results. 6 In regard to early marriage and subsequent childbirth, previous studies rarely separated the effects of age at marriage versus age at childbirth on offspring outcomes, which may undermine the effects of differential determinants on child nutritional outcomes. 8 Furthermore, in cultures where early age at marriage is customary, low age at marriage and childbirth may not necessarily be associated with deprivation and poor child outcomes.8 -10 Other studies, however, have presented negative associations between early marriage and birth outcomes: children born to younger mothers had more odds to be preterm, born with low birth weight and greater chances of stunting compared to children born to older mothers.4,10,11 Still others found either no relationship at all,9,12,13 or that the risks associated with child outcomes may be mitigated by adjusting for maternal nutritional status or behavioral and socioeconomic differences. 14
Childbearing in later years may be associated with adverse outcomes resulting from reproductive aging: the higher likelihood of poor perinatal outcomes and elevated risk of mortality and cancer in adulthood. 15 At the same time, for children born to older mothers, there may be certain advantages over children born to younger mothers: Studies have found that increasing maternal age is associated with a more favorable offspring phenotype (height), better survival outcome for multiple pregnancies, and improved child health and development.6,16 -18 Differences in the pre-and-post-natal child-rearing setting and maternal age-related behaviors may also play a role in these associations. 6
In low-and -middle-income countries, evidence for the influence of maternal age on child growth and nutritional outcomes, 4 particularly with respect to late maternal age and the child’s health is limited. 10 There is also the lack of this research being conducted for European minority populations, including the Roma. The aim of this study was to assess whether maternal age at childbirth is associated with the growth and nutritional status observed among Roma children.
The Roma are the largest European minority, diverse in constituent makeup, and characterized by high levels of exclusion, widespread poverty, and poorer health across many outcomes compared with non-Roma, which is usually explained by socio-economic and health care inequalities. 9 Another common distinctive feature of the otherwise heterogenous European Roma population is their pronatalist, endogamous tradition evidenced by the encouragement of early and endogamous marriages for all females, and high fertility rates. Thus, many Roma females exhibit early marriage, early onset of reproduction, and continuous reproductive activity throughout their most fertile years. 19
In Serbia, there are more than 14 < 0.0010 Roma, who suffer from mass unemployment, inadequate housing, low levels of education, and growing dependence on state benefits and services. 9 The females often enter marriage and become mothers in their teen years. 20 Many of their children exhibit poor nutrition, negatively impacting life outcomes and resulting in intergenerational cycle of poverty and poor development. 21 However, owing to scant data on the effects of maternal age at childbirth on the growth and nutrition of Roma children, their health status has not been fully understood. Previous studies have suggested that the children bear no negative consequences for maternal early marriage and rather that it is bias in maternal investment likely being the main contributor to health disparities observed in the children. 9 That is, some children may be more invested in than others: it is expected that parents should respond to their offspring fitness cues. 22 To address this knowledge deficit, data from Multiple Indicator Cluster Survey rounds 5 and 6 (MICS 5 and 6) for Serbian Roma settlements were used to study the effect of maternal age at childbirth on the nutritional and growth outcomes of children under 5 years from teenage and adult mothers, as well as that of sociodemographic determinants as possible confounders.
Method
A secondary data analysis of the MICS 5 and 6 surveys (2014 and 2019) for Serbian Roma settlements was conducted, where rounds 5 and 6/these were aggregated to assess the association between maternal age at childbirth and child nutritional outcomes, expressed as height-for-age z-score (HAZ), stunting (HAZ −2SD), weight-for-age z-score (WAZ), and underweight (WAZ −2SD). The surveys contained estimates on child health indicators at the national level, and separately for the Roma communities (http://mics.unicef.org/surveys). Serbia is one of the few countries globally to have implemented all MICS rounds (a total of six). Details about the surveys’ methodology can be found elsewhere.20,21 Children aged 0 to 59 months (under 5 years of age) are a key population for many of the MICS indicators. Mothers or caretakers of children aged <5 at the date of the survey, were also asked to provide information on several categories of child health, development and parental engagement. Roma mothers reported on their children’s age, sex, birth order, care and feeding practices, and parental stimulatory and caregiving practices. The section on child health also included anthropometric recordings of height and weight for each child. Weight at birth was obtained from health cards and mothers’ recall. Roma mothers self-reported all data except anthropometric measurements, which were conducted in situ.
The sample consisted of 2564 Roma children aged 0 to 59 months living with their mother (married or in a union), and whose age, anthropometric records and maternal age at childbirth were available. Calculations beforehand included G-power 3.1 for the sample size (database is UNICEF). For regression, minimal n is 178, for power 0.95 and effect size 0.15 (default), for effect size of 0.35—n = 83. For ANOVA, minimum n = 280, power of 0.95 and effect size 0.25 (default program parameters); if effect size = 0.3, minimal sample = 196, while 0.35 = 148. For Chi square min n = 191, power = 0.95, effect size 0.3 (default program parameters), for effect size 0.35 n = 141.
Ethical Approval and Informed Consent
This study was performed as a secondary data analysis of the UNICEF MICS 5 and 6, public use data sets, with no identifying information while all procedures involving research study participants were approved by the UNICEF. The data that support the findings of this study are available from Multiple Indicator Cluster Surveys http://mics.unicef.org/surveys.
Measures
Maternal age at childbirth, a key exposure variable, was self-reported by Roma mothers (n = 2496).
Child Outcomes: Nutritional Status and Growth
HAZ scores, stunting (HAZ −2SD), WAZ scores, and underweight (WAZ −2SD) (from the median values of WHO’s reference population), were used as measures of child growth and nutritional status. Too short for age, that is, stunting, reflects the health of the child: it is very likely that a stunted child has experienced malnutrition for a relatively long period. Underweight-for-age is also a measure of health and nutritional risk as it reflects both past (chronic) and/or present (acute) undernutrition. 20
Covariates
To adjust for theoretical confounders, the following covariates were included in the study. Maternal literacy skills (can read the whole sentence/basic literacy or can read only part of the sentence/functionally illiterate), prenatal care utilization (number of prenatal care visits), and household access to improved toilet facilities were used as proxies for socioeconomic status (SES). Healthcare utilization may be influenced by level of education while poor sanitation, in particular open defecation, is closely connected with low SES, affecting childhood health, as environmental contamination with fecal pathogens may provoke disease, limit nutrient absorption, and lead to inadequacy in height and weight. 23
Other maternal variables included reproductive behaviors, such as parity and birth spacing, while child mortality was estimated by whether a mother ever had a child who later died. In many studies among both contemporary and historic populations, maternal parity was used as approximation for investment and was associated with reduced odds of normal growth. 24 Short birth spacing, reflecting the pace of a reproductive strategy, may bring about higher risks for stunting. 25
Child variables were age (in months) and sex, and for children aged 0 to 24 months—weight at birth and child wantedness (whether the child was wanted at the time of conception).
Statistical Analyses
Descriptive statistics was used to define demographics and child anthropometric variables. Kolmogorov-Smirnov and Shapiro-Wilk test was used to test normal distribution.
Since very young age at childbirth (ie, <15 years) but also at older age (≥35) were more likely to be a risk for poor maternal and child outcomes,4,6 the mothers were divided into four groups based on age at childbirth: age at childbirth in teen years—equal to and below 19—and adult—20 to 24, 25 to 34, and ≥35 years. The chosen cut-off points were based on the sample characteristics and previous studies. 4 Chi-square, ANOVA and Tukey HSD tests were used to evaluate variations in demographics and child outcomes between Roma mothers in the different childbirth age groups.
Roma children were divided into younger children 0 to 24 months, and older children 25 to 59 months, as birth weight and child wantedness data were only collected for the younger group.
To estimate the relationship between maternal age at childbirth and Roma children individual-level HAZ and WAZ scores (for children aged 0-24, and 25-59 months), several multiple regressions were performed. In addition, to explore the association between age at childbirth and children’s stunting and underweight, separate logistics regressions were conducted for the 2 age groups. Only full models are shown.
In the multiple regressions, the dependent variables, that is, individual-level HAZ and WAZ scores, were continuous, while in logistic regressions HAZ and WAZ scores were dichotomous, that is, stunting versus not stunting and underweight versus normal weight. Maternal age at childbirth, number of prenatal care visits, birth spacing (in months) and child’s age (in months) were continuous variables, while weight at birth (low birth weight vs normal birth weight), child wantedness (unwanted vs wanted), sex (boys vs girls), child mortality (yes vs no), maternal literacy (illiterate vs literate), and type of toilet facility (unimproved vs improved) were dichotomous.
Statistical analyses were conducted using SPSS 2.2. Statistical significance was set as P ≤ .05.
Ethical Approval and Informed Consent
This study was performed as a secondary data analysis of UNICEF MICS 5 and 6 public use data sets, with no identifying information. Therefore, ethical approval was not required. All Multiple Indicator Cluster Survey datasets are publicly available from http://mics.unicef.org/surveys.
Results
Roma mothers were relatively young (26, SD = 5,79), with a parity of 3 (range 1-10) (data not shown). At the time the surveys were conducted, all mothers were living in a marriage/union. Maternal age at childbirth for the children in the sample was 24 (SD = 5.63, range 15-48), while age at first marriage and first childbirth were at 17.09 (SD = 3.34) and 18.43 (SD = 3.34), respectively. About 4% of mothers had a live born child who later died. Around one-third of mothers were illiterate (32%), and 17% lived in households without access to improved toilet facility. Antenatal care was used 6 times on average (6,25, SD = 3,43). Birth spacing was, on average, 2 years (24,38, SD = 9,15, range in months 10-54).
The sample comprised 1027 children aged 0 to 24 months and 1537 children aged 25 to 59 months (n = 2564). Average children’s age was 30 months, with a greater number of boys (52%). Children were on average third born, with mean HAZ and WAZ scores below zero (−0.95, SD = 1,.4, and −0.52, SD = 1.16, respectively), while mean WHZ score was at 0.16 (SD = 1.48). 19% were stunted and 9% underweight. For children aged 0 to 24 months, average weight at birth was 3 kg, 16% were unwanted and with low birth weight ≤2.5 kg.
Table 1 presents nutritional status of children and differences in maternal age at childbirth (≤19, 20-24, 25-34, and ≥35 years).
Demographics, Children’s Nutritional Status and Differences by Mother’s Age at Childbirth (≤19, 20-24, 25-34, and ≥35 Years of age) for Roma Mothers and Children.
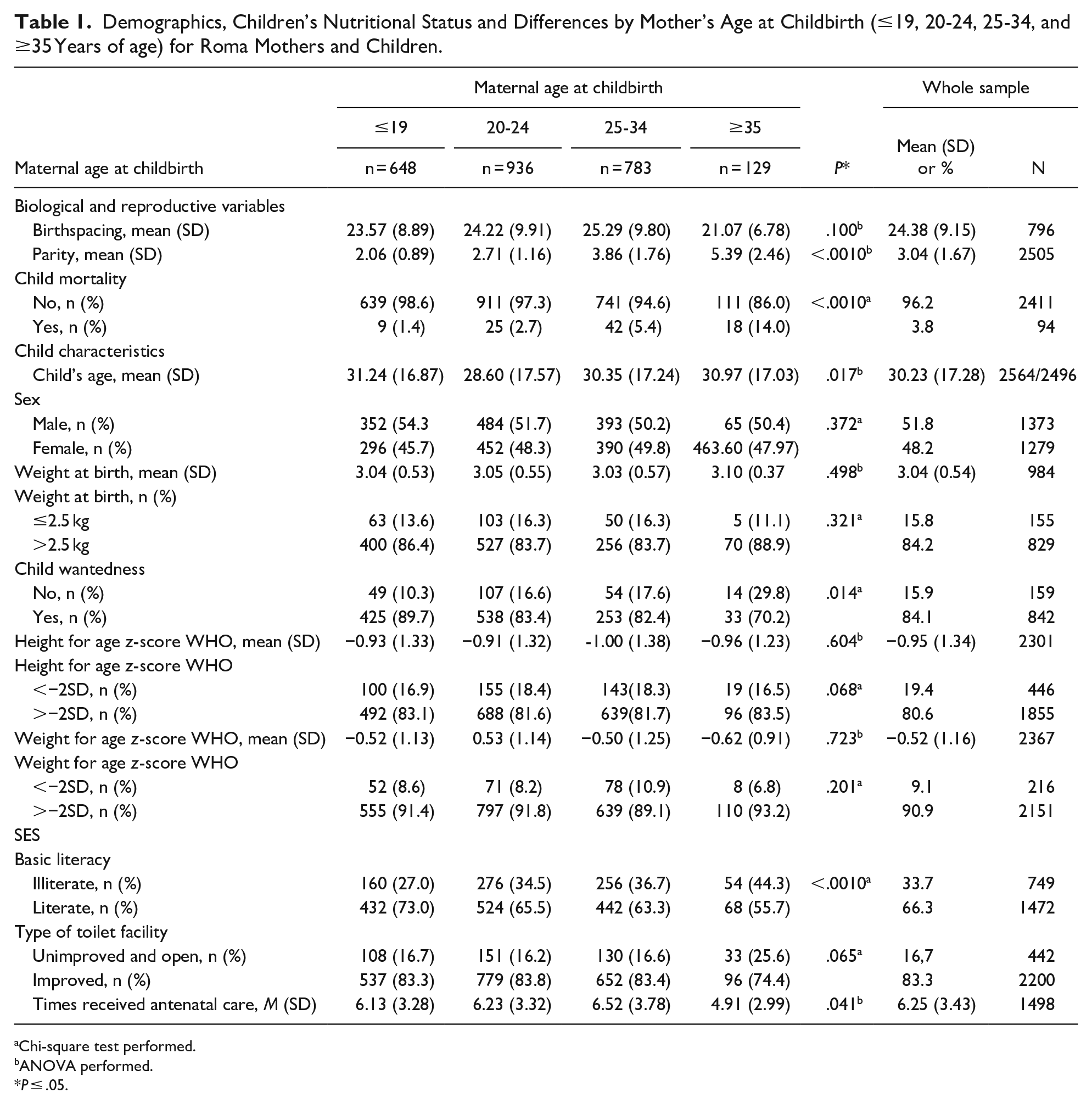
Chi-square test performed.
ANOVA performed.
P ≤ .05.
In the youngest group, ≤19, women were on average 20 years of age at the time the surveys were conducted (19.74, SD = 1.91, range 15-23, n = 648), while women aged between 20 and 24 on average 24 years old (23.72, SD = 1.93, n = 936) women 25 to 34 on average 30 years old (30.30, SD = 3.10, n = 783), and women ≥35 on average 40 years old (39.89, SD = 2.94, range 35-48, n = 129) (data not shown).
There were no differences (P > .05) in children’s HAZ and WAZ, stunting or underweight or birth weight scores/values related to maternal age at birth. Instead, significant differences were observed/found in relation to maternal literacy (P ≤ .001), prenatal care (P = .04), parity (P ≤ .001), child mortality (P =< .001), wantedness (P = .01), and child’s age (P = .02).
Literacy was highest among women in the ≤19 age at childbirth group, antenatal care was most often used by women in the 25 to 34 group, child mortality was/greatest for women ≥35 age at birth, while children in the ≤19 age at childbirth group were older than children to mothers in the 20 to 24 group (M = 31.24, SD = 16.87, vs M = 28.60, SD = 17.57, P < .05), age at birth group. The Tukey HSD test (P < .05) showed that maternal parity was lowest among women in the ≤ 19 age at childbirth group (M = 2.06, SD = 0.89) compared to women in 20 to 24 age at birth group (M = 2.71, SD = 1.16) women in 25 to 34 age at birth group (M = 3.86. SD = 1.76) and women in ≥35 age group (M = 5.39, SD = 2.46). Furthermore, among women in 20 to 24 age at birth group, parity was lower than among women in both the 25 to 34 (M = 3.86. SD = 1.76) group and the ≥35 age at birth group (M = 5.39, SD = 2.46).
Table 2 summarizes the results of multiple regressions estimating the relationship between maternal age at childbirth and child individual-level HAZ and WAZ scores, shown separately for children aged 0 to 24 months and children aged 25 to 59 months.
Multiple Linear Regression Analyses: Associations of Maternal Age at Childbirth and Roma Children Individual-Level Height-for-Age z (HAZ) and Individual-Level-Weight-for Age z (WAZ) Scores.

P ≤ .05.
Maternal age at childbirth had no statistically significant bearing on child HAZ or WAZ scores (P > .05), whereas weight at birth was significant for predicting these scores in children aged 0 to 24 months. Children born above 2.5 kg were, on average, taller by .49 standard deviations (β = .49, 95% CI = <−0.001, 1.49, P ≤ .001) and heavier by 1.45 standard deviations (β = 1.45; 95% CI = 1.33, 2.16; P ≤ .001), compared with those born below 2.5 kg. Furthermore, widely spaced children were heavier ((β = .09, 95% CI = <0.001, 0.20, P ≤ .001), as well as those who were older (β = 1.59; 95% CI = 0.410, 2.778; P ≤ .001), wanted (β = .37, 95% CI = 0.11, 0.60, P ≤ .001), with literate mothers (β = .39, 95% CI = 0.11, 0.66, P ≤ .001), who used antenatal care more often (β = .32, 95% CI = 0.15, 0.64, P ≤ .001). Maternal parity negatively impacted WAZ scores (β = −.76; 95% CI = −1.22, −0.55; P ≤ .001), thus children with more siblings and boys (β = −.55; 95% CI = −0.91, −0.41; P ≤ .001) had lower WAZ scores than their counterparts.
For children aged 25 to 59 months, both HAZ and WAZ scores were negatively associated with maternal parity (β = −.16; 95% CI = −0.33, −0.07; P << .0011, and β = −.13; 95% CI = −0.03, −0.55; P = .03, respectively), and positively associated with child age (β = .13; 95% CI = 0.08, 0.44; P = .01, and β = .09; 95% CI = < 0.001, 0.35; P = .04, respectively). Also, literate mothers (β = .12; 95% CI = 0.04, 0.25; P = .01), who used antenatal care more often (β = .09; 95% CI = <0.0011, 0.22; P = .04), had taller children.
Table 3 summarizes the results of logistic regression analyses of associations of maternal age at childbirth and Roma children stunting and underweight.
Logistic Regression Analyses: Associations of Maternal Age at Childbirth and Roma Children Stunting (−2SD HAZ) and Underweight (−2SD WAZ).
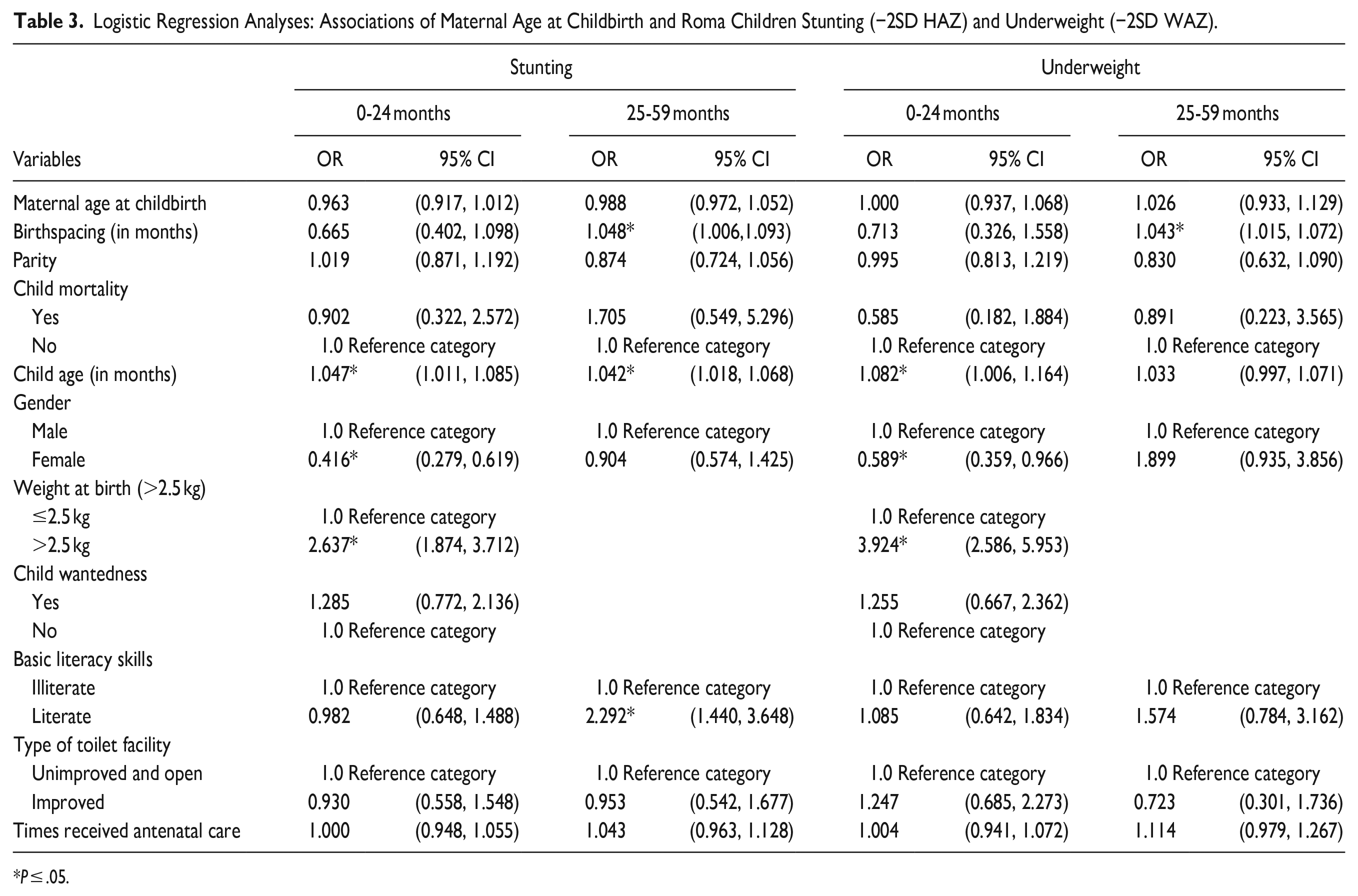
P ≤ .05.
Maternal age at childbirth did not have an effect on Roma child stunting or underweight (P > .05). Instead, for the younger group of children (0-24 months), children born above 2.5 kg had lower odds to be stunted and underweight (OR = 2.64; 95% CI = 1.87-3.71; P << .0011, and OR = 3.92; 95% CI = 2.59-35.95; P << .0011, respectively) than their counterparts. Boys had higher odds to be stunted and underweight than girls (OR = 0.42; 95% CI = 0.28-0.62; P << .0011, and OR = 3.92; 95% CI = 2.59-35.95; P << .0011, respectively), and older children had lower odds to be stunted (OR = 1.05; 95% CI = 1.01, 1.09; P = .04) and underweight (OR = 1.08; 95% CI = 1.00, 1.16; P = .01) than their counterparts.
For children aged 25 to 59 months, older children (OR = 1.04; 95% CI = 1.02, 1.07; P << .0011), born to literate mothers (OR = 2.29; 95% CI = 1.44, −3.65; P << .0011), and those more widely spaced had lower odds to be stunted (OR = 1.05; 95% CI = 1.01, 1.09, P = .01) and underweight (OR = 1.04; 95% CI = 1.02, 1.07, P = .01) than their counterparts.
Discussion
Maternal age at childbirth showed no association with either nutritional or growth outcomes of the Roma offspring. This pattern was detected also after comparing children among women in different childbirth age-groups, as there were no differences found in children’s HAZ and WAZ scores, stunting or underweight. These findings are consistent with other studies where it was found that maternal age at childbirth had no effect on children’s outcomes.12,13
For Roma mothers, the mean age at first reproduction was 18 years, which in traditional societies is an estimated optimal age for first reproduction. 26 Beyond this age, Roma women continue to have children in their most fertile years: the majority (38%) of children in this sample were born to mothers aged 20 to 24. One fourth (26%) of Roma women gave birth at ≤19 years of age, with the youngest being just 15, while more than 5% of women gave birth at age ≥ 35. Data on maternal health or height (used a as proxy for health) are lacking in the MICS samples but it is possible that difference among Roma women may be large enough that both early and/or late reproduction and good health are experienced by the same women: for example, healthier mothers tend to have healthier babies.27,28 This might explain the lack of nutritional and growth penalties for children born to teenage and/or older Roma mothers: that is, maternal age at childbirth alone may not increase the chances of poor child health outcomes as the risks could be more related to individual characteristics and behavioral patterns of the mother.22,29
This is in keeping with the results of other studies, where various maternal and child characteristics accounted for the variations in children’s growth and nutrition.14,22,29 Maternal reproductive behaviors, such as parity, birth spacing and SES were found to explain the growth and nutritional features observed in this sample. Maternal parity affects not only size at birth, postnatal growth and body composition but also morbidity. 30 It also represents a critical trade-off between number and size of offspring 24 : Roma maternal parity was negatively associated with WAZ scores for children aged 0 to 24 months, and with both HAZ and WAZ scores for those aged 25 to 59 months. Thus, Roma mothers with greater parity had children who were shorter and had lower WAZ scores than mothers with lower parity. Under poor conditions especially, numerous siblings may put children at higher risk of malnutrition, owing to the effect of greater family size on available resources. 31
Birth spacing, for Roma women was 2 years on average, but with considerable range variation. The results show that among Roma children aged 0 to 24 months, those more widely spaced tended to weigh more than their counterparts, and in children aged 25 to 59 months those who were more widely spaced had lower odds to be stunted and underweight than their shorter-spaced counterparts. Numerous studies have identified short birth-spacing as a risk factor for poor nutritional status in both mother and child, significantly increasing the risk of stunting. 32 In contrast, longer birth intervals (≥24 months) are found to be strongly associated with decreased risk of childhood undernutrition.
Furthermore, social factors may affect access to healthcare and children’ wellbeing. As with other studies, in this sample, both maternal literacy and antenatal care were positively associated with WAZ scores for younger group of children, while for the older group, with HAZ scores. 33 In the older group, children born to literate mothers were less stunted than their younger group counterparts. Mothers’ level of education may also increase their use of healthcare during pregnancy, as well as child nutrition and care practices, in turn affecting child health outcomes. 34 In this sample, over one-third of Roma mothers were illiterate, and studies have found that even a small increase in maternal education corresponds with a considerable decrease in child poor health outcomes. 35
In addition to maternal influences, child’s weight at birth, sex, wantedness, and age, were shown to contribute to the health outcomes of the Roma children. In line with other studies, weight at birth appeared as a significant predictor for growth and nutritional status of children aged 0 to 24 months: Those born above 2.5 kg were taller, heavier and less likely to be stunted and underweight than their lighter counterparts. 36 Evolutionary studies have often used birth weight as a simple proxy of maternal investment in utero, with the assumption that there is a positive association between birth weight and offspring fitness. 8 The effect of prenatal maternal effort on child birth weight significantly determines infant morbidity and mortality, cognitive and overall development, adult stature and marriage prospects. 13
Sex differences in nutritional status were detectable among children aged 0 to 24 months, with boys having lower WAZ scores and being more underweight and stunted than their female counterparts. These results suggest a greater susceptibility to nutritional inequalities of Roma boys than girls of the same age, a common finding in some settings, likely owing to a mixture of the biological and social traits underlying the differences. 37
Furthermore, among children aged 0 to 24 months, wanted children were heavier than their unwanted counterparts, indicating, as in other studies, that being unwanted is associated with adverse health outcomes. 8 This highlights unwanted childbearing as an important public health issue, as it is usually associated with disadvantageous maternal behavior during pregnancy and differential treatment of unwanted children.
Across all child ages in this study, child outcomes were affected by child’s age: in both child groups, age was positively associated with WAZ scores, while for children 25 to 59, with HAZ scores. Furthermore, older children were less likely to be stunted and underweight than their younger counterparts. In general, it is found that older children tend to be more nutritionally advantaged and have a considerably lower mortality risk compared with their younger siblings. 38 Children’s age is also associated with birth order and parents may unevenly invest in their children in view of this: the child’s reproductive value increases with age, thus older children may be much more valued than younger ones. 39 In addition, having numerous siblings in a family may also result in increased economic hardship, as the birth of each additional child limits the time, attention and other resources parents can allocate to any one child. 31
This study adds new evidence from the nationally representative Serbian Roma dataset on the association between maternal age at childbirth and child growth and nutritional measures. Some limitations that may have biased the results are noted: cross-sectional design of the MICS studies prevented causal inference. Most of the variables were self-reported by the Roma mothers. Other confounding variables, including maternal height and health, gestation period, previous preterm or low birth weight births, and birthweights for older children, were not collected. As the sample was mixed age, child’s age in itself may be a confounding factor in estimating nutritional and growth outcomes: the age range of 0 to 2 years included very different trajectories of infant growth. 3 Future studies should include more detailed data on individual risk factors such as of the role of nutrition (including breastfeeding practices and dietary intake) in infant growth, and maternal characteristics connected with early and/or late maternal age at childbirth, such as social costs for early childbearing, maternal reproductive stress levels, and unhealthy behaviors associated with early and/or older maternal age at birth. 23
Conclusion
No differences in Roma children growth and nutritional outcomes were found in relation to maternal age at childbirth. Instead, maternal (SES, reproductive behaviors: parity and birth spacing) and child (birthweight and wantedness for the younger group of children, and sex) characteristics were the strongest predictors of poor growth and nutrition.
Despite its limitations, the present study contributes to existing literature on the relationship between maternal age at childbirth and child growth and nutritional outcomes in the Serbian Roma population. The results could be useful for policymakers especially in regard to ethnic minority family planning and childhood nutrition.
Footnotes
Author Contribution
JČ is the sole author.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study was performed as a secondary data analysis of the UNICEF MICS 5 and 6, public use data sets, with no identifying information. Therefore, ethnical approval was not needed. All Multiple Indicator Cluster Surveys datasets are publicly available from ![]() . The author asserts that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
. The author asserts that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.