
Abstract
Background. Pneumonia and bronchiolitis are common childhood illnesses caused by the respiratory syncytial virus. A systematic analysis of published epidemiological data in sub-Saharan African children under the age of 5 was conducted. Methods. To retrieve literature, electronic databases, indexing services, and directories such as PubMed/MEDLINE, Scopus, EMBASE (Elsevier), Google Scholar, and Worldcat were utilized. Data from the included studies were extracted after screening and eligibility evaluation. Results. The pooled prevalence rate of respiratory syncytial virus was 21% (95% CI: 17, 25). Subgroup analysis based on participants’ ages showed that, prevalence was highest in children <6 months (32%). High prevalence was also found in children who were hospitalized (27%), children co-infected with HIV (28%), and children co-infected with bacteria respiratory pathogens (22%). Conclusion. The prevalence of respiratory syncytial virus infection was high in children in sub-Saharan African countries. Therefore, it should be prioritized as a major health problem.
Introduction
In the poorest countries, such as sub-Saharan Africa, severe acute respiratory illness (SARI) is one of the most common causes of pediatric hospitalizations and deaths. 1 In spite of the public health and clinical importance of SARI, most sub-Saharan African countries do not have adequate surveillance for overall and cause-specific SARI hospitalizations and deaths. 2
It was estimated that approximately 5.8 million deaths were caused by acute lower respiratory tract infections (ALRTIs) in 2010. Sub-Saharan Africa accounted for about half of these deaths. 3 Globally, ALRTIs are responsible for about 4 million of the 15 million under-5 mortality cases every year. About 1 in 5 of the deaths of children in low- and middle-income countries in 2011 were caused by ALRTIs. 4
There are a number of organisms that may cause ALRTIs among children under the age of five, including Staphylococcus aureus, Streptococcus pyogenes, Pneumococci, Haemophilus influenzae, and Klebsiella pneumoniae. Respiratory syncytial virus (RSV), adenoviruses, influenza viruses, and enteroviruses are also common etiological agents. 5
In the family Paramyxoviridae, RSV belongs to the pneumovirus genus. It is an enveloped virus with a single-stranded negative-sense ribonucleic acid (RNA) genome. 6 From mild upper respiratory tract illnesses (URTIs) to severe and potentially life-threatening lower respiratory tract infections (LRTIs), RSV infection can present with a variety of clinical manifestations. 7 In children, RSV is a leading cause of pneumonia and bronchiolitis, particularly in the lower respiratory tract. The number of RSV-associated ALRTIs cases worldwide in 2015 was estimated at 33.1 million, with 3.2 million hospitalizations and 27 300 deaths among infants under 6 months of age. 8
The Pneumonia Etiology Research for Child Health (PERCH) project conducted a multi-site, international case-control study in 7 countries (Bangladesh, Gambia, Kenya, Mali, South Africa, Thailand, and Zambia). The study enrolled 4232 children aged 1 to 59 months who were hospitalized for severe pneumonia (cases) and 5119 community controls. The results showed that RSV had the highest etiological fraction (31.1%, 95% CrI 28.4-34.2) of all pathogens. 9
Systematically aggregating and analyzing published epidemiological data on RSV in young children in sub-Saharan Africa, which is a highly populated region with diverse ethnic populations, is crucial in order to ascertain the burden of the disease for evidence-based public health priorities, summarize the currently available data and identify the gaps and scope for further epidemiological study of RSV in this region. Furthermore, numerous RSV immunization products are in the pipeline. This regional estimates of RSV in children aged younger than 5 years, together with the available global estimates, provide important baseline information to support decision-making about the introduction of these products.10 -12 Thus, the aim of this review and meta-analysis, was to systematically aggregate and analyze published epidemiological data on RSV infection in young children in Sub-Saharan countries.
Methods
Outcome Measurements
The primary outcome measure was the prevalence of RSV infection. The purpose of this study is to estimate the prevalence of RSV in children under the age of 5 in Sub-Saharan Africa.
Study Protocol
In addition to identifying records, screening titles and abstracts, and evaluating the eligibility of full texts, the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) was used. 13 There is an online version of the methodology available, and it is registered on PROSPERO under the reference number CRD42021278964: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021278964.
Identification of Records and Search Strategy
In order to conduct the literature search, we used databases and indexing services such as PubMed/MEDLINE, EMBASE (Elsevier interface), Scopus, as well as other supplementary resources such as Google Scholar and Worldcat. Using advanced search strategies, we retrieved relevant findings by restricting the search to studies published in English on human subjects. Google Scholar and Worldcat were used to access gray literature from organizations and online university repositories. Articles were retrieved using key words and indexing terms. The key words used for searching were “Respiratory Syncytial Virus,” “RSV,” and “Africa South of the Sahara” [MeSH]. Boolean operators (AND, OR) were also used in the identification of records. Searches were conducted between August 16 and September 16, 2021.
Screening and Eligibility of Studies
Endnote reference software version 7 (Thomson Reuters, Stamford, CT, USA) was used to screen and qualify records identified from electronic databases, indexing services, and directories. Endnote was used to identify, record, and remove duplicate records. Due to the different reference formats used by the various sources, some duplicates were removed manually. After that, 2 authors independently reviewed the titles and abstracts using predetermined inclusion criteria (HM and ME). Additionally, 2 authors (HM and NA) separately gathered the full text and assessed it for final inclusion eligibility.
Inclusion and Exclusion Criteria
Titles and abstracts were screened for eligibility using predefined inclusion-exclusion criteria, and complete texts were evaluated for eligibility. Observational studies (cross-sectional, and case control) addressing the prevalence of RSV from a human source (patients) less than 5 years of age, regardless of the clinical characteristics. For additional eligibility assessment, only English-language literature and research carried out in sub-Saharan African nations between January 2010 and September 2021 (the final date of the literature searches) were taken into consideration. All original articles outside of sub-Saharan Africa, review papers, books, letters, brief reports, case reports, meeting reports, poster presentations and studies conducted before January 2010 were excluded during the screening of titles and abstracts. When screening full-text papers, those with irretrievable full-texts records, unrelated outcome measures, articles with missing or insufficient results, and studies done before January 2010 were discarded.
Data Extraction
Two authors (HM and TT) independently retrieved significant data relating to research characteristics from the included studies using an Excel sheet. The following information was taken from the study characteristics and outcome measures data: first author and publication year, region, country, age of the study participant, population (patient type), clinical features, diagnostic method for detection of RSV, co-infection, number of RSV infected-individuals, sample size, and prevalence of RSV.
Quality Assessment of Studies
The Joanna Briggs Institute (JBI) critical evaluation checklist for observational studies (check list for prevalence study and case control studies), University of Adelaide, Australia, was used to evaluate the internal and external validity of included research. 14 The evaluation instrument for the included questions on the study’s quality was based on the following replies to design-specific questions: no, unclear, yes, and not applicable. Prevalence studies were graded out of 9 points, and case control studies were graded out of 10 points. The systematic review and meta-analysis only included studies with more than half of the checklist items’ receiving affirmative responses (yes), or a score of 5 or above.
Data Processing and Statistical Analysis
For outcome measures and subgroup analyses, the pertinent data were retrieved from the included studies using a format created in Microsoft Excel and exported to STATA 16.0. For outcome measures and subgroup analyses, the pertinent data were retrieved from the included studies using a format created in Microsoft Excel and exported to STATA 16.0. I 2 statistics were used to determine the heterogeneity of the studies. The Egger’s tests was used to assess the presence of publication bias. A statistical test was deemed significant if the P-value was less than .05.
Ethics Approval and Informed Consent
Not applicable (ethical clearance is not required for this review of the literature; however, the study is registered on PROSPERO with the reference number CRD42021278964 in order to prevent duplicate reviews on related topics).
Result
Search Results
The search of electronic databases, including PubMed/Medline, Scopus, EMBASE (ELSIVER interface), Google Scholar, and Worldcat, turned up a total of 1391 studies. A total of 702 records were examined using their titles and abstracts after 689 duplicates were eliminated using the Endnote reference manager and human tracing, and 621 of them were rejected. Following the evaluation of the full texts of 81 records for eligibility, 46 articles were also disqualified because the desired outcome was unclear, the desired outcome was missing, the full text of the article could not be located, the study was conducted in another nation, and the study was completed before January 2010. Finally, 35 articles have passed the eligibility criteria (Figure 1).

PRISMA flow chart describing the selection process.
Of the 35 studies that met the eligibility requirements, 28 were cross-sectional studies, and the remaining 7 were case-control studies. The maximum and minimum scores of the quality assessment for the cross-sectional studies were 9 and 5, respectively. The maximum and minimum scores of the quality assessment of the case control studies were 9 and 5, respectively. Thirty-five studies were evaluated for quality, and all passed; as a result, they were all included in the study.
Study Characteristics
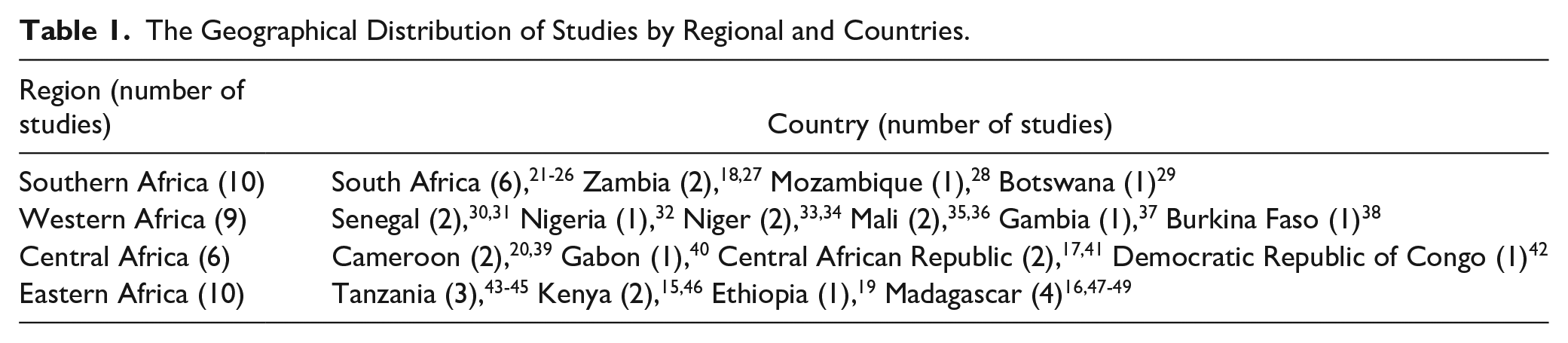
A total of 35 studies with 32 994 research participants from 18 Sub-Saharan African member countries were included. The oldest studies were published in 201215,16 and the most recent were published in 2021.17 -20 The geographical distribution of studies by region and country are depicted in Table 1.
The Geographical Distribution of Studies by Regional and Countries.
The cross-sectional study type was utilized in more than two-thirds (32) of the included studies, while the case control study design was used in the remaining 7 studies. The study period ranges from January 2010 to December 2019. Almost all 36 studies use PCR for the detection of RSV infection, except three, which use ELISA and immunochromatographic assays for diagnosis. The studies included participants ranging from 100 20 to 4293. 21 The largest study was carried out in South Africa 21 whereas the smallest study carried out in Cameroon 20 (Table 2).
Characteristics of Studies Describing the Prevalence of RSV Infection in Under 5 Children.

Abbreviations: CRA, Central African Republic; com, community; Imm, immunization; PN, pneumonia; AFI, acute febrile illness; WRF, without respiratory features; CAP, community acquired pneumonia; ICA, immunochromatographic assay; B, bacterial infection; M, malaria; yrs, years; mon, month; ELISA, enzyme-linked immunosorbent assay; RSV, respiratory syncytial virus; co-inf, co-infection; DR, democratic republic; SARI, severe acute respiratory infection; ILI, influenza-like illness; URTI, upper respiratory tract infection; ARI, acute respiratory infection; ALRI, acute lower-respiratory infection; RTI, respiratory tract infection; LRTI, lower respiratory tract infection; PCR, polymerase chain reaction.
Every study that was included was conducted in a hospital; 17 of the studies included hospitalized children, 8 studies included outpatients, and the remaining 10 studies included both inpatient and outpatient patients. Upon examining the clinical features of the subjects involved in these investigations, we found that every single one of them had a respiratory tract infection, with the exception of one who had an acute, uncomplicated fever. There were 3 studies done on infants under 6 months old, 7 studies on children under 2 years old, and the remaining twenty-five studies included children under 5 years old (Table 2).
Study Outcome Measures
The reported prevalence rate of RSV varied widely, with the highest rate of 48% reported from Madagascar 48 and the lowest rate of 1% reported from the Democratic Republic of Congo. 42 The pooled prevalence of RSV was 21% (95% CI: 17, 25). The I 2 statistics show that there was significant study-to-study heterogeneity when the random effects model was employed for this meta-analysis (I 2 = 98.99%, P < .001) (Figure 2).

Forest plot depicting the pooled estimate of the prevalence of RSV infection in under 5 children in sub-Saharan Africa.
Sensitivity Analyses
Outliers were taken out of the analysis to do sensitivity analysis. Even after outliers were removed from the analysis, the level of heterogeneity did not alter significantly. As a result, the meta-analysis included all of the papers that met the quality assessment criteria.
Subgroup Analyses
A subgroup analysis was conducted based on the region, age, study settings and co-infections. According to the results of the subgroup analysis based on region, Sub-Saharan Africa’s western region had the highest prevalence of RSV (24%; 95% CI: 16, 32) while the lowest was the central region (10%; 95% CI: 5, 15) (Figure 3).

Pooled prevalence of RSV based on region of sub-Saharan Africa.
The pooled prevalence of the respiratory syncytial virus was highest in the age group less than 6 months, according to the results of the subgroup analysis based on age (32%; CI: 28, 36), followed by the age group less than 2 years of age (26%; CI: 16, 36). The result of the subgroup analysis based on study setting also revealed that the pooled prevalence of RSV was highest in hospitalized patients (27%; CI: 22, 32), followed by both hospitalized and outpatients (18%; CI: 12, 24) (Figure 4).

Sub-group analysis based on age of studies and study setting.
The result of the subgroup analysis based on co-infection revealed that the prevalence of respiratory syncytial virus was highest in HIV co-infected (28%; CI: 24, 32), followed by co-infected with bacterial respiratory tract pathogens (22%; CI: 12, 32) (Supplemental Figure 1).
Publication Bias
Publication bias was considered but not analyzed statistically.
Discussion
Infection with the RSV is a significant public health issue in poor nations, and this is also true of countries in Sub-Saharan Africa. Based on the available data, the present study attempted to provide an up-to-date and comprehensive assessment of the prevalence of RSV among children <5 years of age in Sub-Saharan African countries. A total of 35 studies, encompassing 32 994 study participants from 18 member countries of Sub-Saharan Africa, were included in this study. The pooled prevalence rate of RSV was 21%. RSV prevalence was highest in children <6 months, children who were hospitalized, children co-infected with HIV, and children co-infected with bacterial respiratory pathogens.
According to this systematic review and meta-analysis of data from 35 studies with 32 994 individuals, in Sub-Saharan Africa, children under the age of 5 were found to have a pooled prevalence of RSV infection of 21%, with significant heterogeneity. Excluding outliers from the study allowed for the execution of sensitivity analysis, although the level of heterogeneity was not significantly altered. The drivers of the high prevalence of RSV infection included age, study settings and being co-infected.
Only 18 countries were included in the review, and most (72.2%) of the reported studies were done among 3 sub-Saharan African countries (South Africa, Madagascar, and Tanzania). The majority of the sub-Saharan African countries are not represented in this review. Most of the studies reported in this review were carried out in influenza virus surveillance programs, which have been established in collaboration with WHO for more than 10 years to improve the detection of influenza and non-influenza viruses. However, there are no platforms for systematic information sharing in the region. 50
The substantial heterogeneity (variability) observed in the pooled prevalence of RSV in this study. The sample size of each study varied considerably; we included studies with the minimum sample size of 100 and the maximum sample size of 4293. The sample size variation might contribute to the heterogeneity (variability) of the pooled estimate. Furthermore, there was variation in the age groups of participants included in each study: children under the age of five, children under the age of two, and children younger than 6 months old. Since data from different age groups were pooled together, it contributes to the substantial heterogeneity (variability) of the pooled estimate. Other methodological factors, such as variation in clinical features, study seating, and the presence of co-infection, also contribute to the heterogeneity (variability) of the pooled estimate.
The present study, the reported prevalence rate of RSV varied widely, with the highest rate of 48% and the lowest rate of 1%. Due to a number of factors, including the features of the study, the burden of respiratory viral infections is likely to vary from country to country; like study site, disease severity, duration of the study, season of the year, age range for study inclusion, patients selection criteria, health care and hospitalization setting or laboratory and specimen management like sampling method (nasopharyngeal aspiration/wash and nasal wash vs nasal swab, nasopharyngeal swab or throat swab technique), quality of specimen samples, transport and storage condition of the samples, time of collection in relation to onset of illness, methodology applied to establish the diagnosis (eg, reverse transcriptase polymerase Chain Reaction (RT-PCR), immunochromatographic assay, serology), quality of reagents, laboratory technician experience, inter and intra-laboratory standardization.10,51
In a similar review conducted among children less than 5 years of age in the WHO European Region, a pooled prevalence of 46% was reported, with the highest rate of 76% and the lowest rate of 6%. 52 This is higher than we found (a pooled prevalence of RSV infection of 21% with the highest rate of 47.7% and the lowest rate of 1.1%) in this systematic review and meta-analysis. The difference might be due to the difference in study subjects. They included research done on children who had acute respiratory tract infections (respiratory infection, pneumonia, or bronchiolitis). In our case, we include studies that include children with uncomplicated fever, influenza like-illnesses, acute respiratory tract infections and healthy.
The pooled prevalence of RSV was higher in western region of Africa. Whereas the lowest reported from central Africa region. This might be due to variations in patients’ selection criteria, health care settings, and the season of the year where the study was carried out.
Only a small number of epidemiological studies revealed RSV incidence broken down by similar age groups. The highest prevalence (32%) was reported in children <6 months compared to the age group <2 years (26%), and the age group less than <5 years (18%). A similar finding was also reported by a review carried out in developing countries, China, and Latin America that reported the highest incidence rates in young infants aged <6 months.10,51,53 According to the Child Health and Mortality Prevention Surveillance (CHAMPS) study conducted in 7 countries in sub-Saharan Africa and south Asia, RSV is a significant cause of death in children under the age of 5, especially in infants between the ages of 28 days and 6 months; in this age range, RSV was responsible for 1 out of every 15 deaths. 54 This might be due to a naturally weak immune system in this age group compared to other age groups.
The highest prevalence (27%) was reported from studies that includes children who were hospitalized (inpatients) compared to studies which included children who were outpatients (16%). A similar review conducted in China reported that a higher prevalence of RSV was seen in inpatients (22%) compared to 13.8% in outpatients. 51 According to a review done in the European Region, RSV-related respiratory infections continue to be a serious health concern for young infants. 52 However, inadequate reporting, incorrect classification, and a lack of national guidelines for RSV diagnostic tests show that statistics are rarely adequate to determine the incidence or prevalence of RSV-associated disease, implying the need for additional research to obtain accurate data. 52
The prevalence rate of RSV in those studies included patients who were found to be co-infected with HIV, which was higher than those who were not found to be co-infected with HIV. A similar finding was also reported by a review carried out in developing countries and globally.10,55 The possible explanation is that HIV infection affects the cell-mediated immune pathways required for defense against RSV infection.
The prevalence rate of RSV in those studies which included patients co-infected with other respiratory bacteria pathogens, was also higher. A similar finding was reported by a review carried out in developing countries. 10 According to the CHAMPS study, which was conducted in 7 countries in sub-Saharan Africa and south Asia, the majority of RSV-related deaths in infants were really caused by other illnesses (most commonly co-infection with other respiratory bacteria pathogens). 54 This indicates that RSV deaths are more common in children who are particularly vulnerable, such as those who have a birth abnormality, are also infected with bacteria, or whose RSV results in subsequent infections with different pathogens. The multiplicity of pathogens that have been found and proven to be involved in the causative chain emphasizes the likelihood that more than one pathogen is frequently to blame for severe pneumonia episodes. 54
Limitation of the Review
Due to a lack of studies that assessed the risk factors of RSV, this review could not address the risk of RSV. Moreover, only 18 countries were included in the review, but the majority of other sub-Saharan African countries were not represented. So, the review may not be able to generalize to sub-Saharan African countries. Because of different case-finding methodologies, varying study years, and inconsistent age classification techniques, it is difficult to compare the findings from the reviewed literature.
Conclusions and Recommendations
This systematic review showed the highest prevalence of RSV reported among children of sub-Saharan African countries, particularly among infants. The highest prevalence was also reported from studies, which included children who were hospitalized. Therefore, it should be prioritized as a major health problem, and healthcare providers, researchers, ministers of health, and the World Health Organization must work hard to improve detection, manage conditions properly overall, and exert effective control.
In the present systematic review, the reported prevalence rate of RSV in the past decade has varied widely; the majority of the sub-Saharan African countries were not included in the present systematic review. Therefore, additional RSV monitoring studies must be established in order to increase incidence estimates.
Most of the studies reported in this review carried out in influenza surveillance programs, which is established in collaboration with WHO, to enhanced the detection of influenza viruses for over a decade. By incorporating RSV research into current influenza surveillance systems, more proof of the prevalence of RSV disease in Sub-Saharan African nations can be established.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241298803 – Supplemental material for Prevalence of Respiratory Syncytial Virus Among Children Under 5 Years of Age in Sub-Saharan Africa
Supplemental material, sj-docx-1-gph-10.1177_2333794X241298803 for Prevalence of Respiratory Syncytial Virus Among Children Under 5 Years of Age in Sub-Saharan Africa by Habtamu Mitiku, Tewodros Tesfa, Mekuria Edae and Nega Assefa in Global Pediatric Health
Footnotes
Acknowledgements
We would like to thank Mr. Mekonnen Sisay and Mr. Teshager Worku, who have technically supported us to realize this systematic review and meta-analysis.
Author Contributions
HM and NA conceived and designed the study. All authors collected scientific literatures, critically appraised individual articles for inclusion, analyzed and interpreted the findings. HM drafted the manuscript, critically reviewed it and prepared the final version for publication. All authors read and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.