
Abstract
Objective:
Preconception care is aimed to promote optimal health in women before conception to reduce or prevent poor pregnancy outcomes. Although there are several published primary studies from sub-Saharan African countries on preconception care, they need to quantify the extent of preconception care utilization, the knowledge level about preconception care, and the association among women in the reproductive age group in this region. This systematic review and meta-analysis aimed to estimate the pooled utilization of preconception care, pooled knowledge level about preconception care, and their association among women in the reproductive age group in sub-Saharan Africa.
Methods:
Databases including PubMed, Science Direct, Hinari, Google Scholar, and Cochrane library were systematically searched for relevant literature. Additionally, the references of included articles were checked for additional possible sources. The Cochrane Q test statistics and I2 tests were used to assess the heterogeneity of the included studies. A random-effect meta-analysis model was used to estimate the pooled prevalence of preconception care, knowledge level of preconception care, and their correlation among reproductive-aged women in sub-Saharan African countries.
Results:
Of the identified 1593 articles, 20 studies were included in the final analysis. The pooled utilization of preconception care and good knowledge level about preconception care among women of reproductive age were found to be 24.05% (95% confidence interval: 16.61, 31.49) and 33.27% (95% confidence interval: 24.78, 41.77), respectively. Women in the reproductive age group with good knowledge levels were greater than two times more likely to utilize the preconception care than the women with poor knowledge levels in sub-Saharan African countries (odds ratio: 2.35, 95% confidence interval: 1.16, 4.76).
Conclusion:
In sub-Saharan African countries, the utilization of preconception care and knowledge toward preconception care were low. Additionally, the current meta-analysis found good knowledge level to be significantly associated with the utilization of preconception care among women of reproductive age. These findings indicate that it is imperative to launch programs to improve the knowledge level about preconception care utilization among women in the reproductive age group in sub-Saharan African countries.
Keywords
Introduction
Preconception care (PCC) provides biomedical, behavioral, and social health interventions to women and couples before conception and between pregnancies. This care provision aims to prevent poor maternal and child health outcomes by improving women’s and couples’ health status. 1
The World Health Organization (WHO) has recommended a package of interventions for PCC: maternal nutrition such as micronutrient supplementation (iron, folic acids, and others), vaccination, cessation of tobacco and excessive alcohol use, prevention of interpersonal violence, sexuality education, and protection from environmental hazards, genetic counseling, and support for mental health. Adolescence is the prime—though not the only—window of opportunity to deliver these interventions. 2
Despite the growing body of evidence that PCC improves the health and well-being of women and couples, and subsequently improves the pregnancies and child health outcomes, evidence exists that a gap exists in the continuum of PCC for women in the reproductive age group.1,3
Adequate and equitable access to improved reproductive health care lowers fertility rates, prevents sexually transmitted infections, and improves pregnancy outcomes, with broader individual, family, and societal benefits. Such benefits may include a healthier and more productive workforce and access to greater financial and other resources for children, especially those in smaller families. Furthermore, access to adequate and quality reproductive health services is linked to achieving the sustainable development goal number 3 targets, advocating for healthy lives and well-being for all ages. 4
It has been acknowledged that 41% of all women report their pregnancies as unplanned, highlighting a pragmatic necessity for the general preconception of good health to be promoted to all women of reproductive age. 5
Many maternal and neonatal adverse outcomes could be averted through the effective utilization of PCC. For example, evidence informs us that maternal undernutrition and iron deficiency anemia increase the risk of maternal death by at least 20% worldwide. Also, up to 35% of pregnancies among women with untreated gonococcal infections can result in low birthweight infants and premature deliveries, and up to 10% of pregnancies result in perinatal death. 6
Sub-Saharan Africa (SSA) is a region with one of the highest maternal mortality ratios in the world. For example, in 2015, this region recorded nearly 550 maternal deaths per 100,000 live births compared to a global rate of 216 deaths per 100,000 live births. Spatial inequalities in access to life-saving maternal and newborn health services persist within SSA. 6 PCC is also reported to be poorly provided within maternal health services in the region. 4
A number of individual studies conducted in SSA region have shown inconsistency in the utilization of PCC among women in the reproductive age group with prevalence rates ranging from 13.4% to 34.1%. In some studies, knowledge about PCC care has also been examined and suggested to be negatively associated with PCC utilization, which is an unintuitive result. Furthermore, the level of knowledge varies substantially in SSA countries, with the range of 8.3–65.3 %.2,7–14 These inconsistencies may need to be revised for health policymakers and planners to use for decision-making and program planning. Moreover, early prevention and management of poor outcomes using PCC have been essential to save the life of mothers and reduce morbidity. Still, there need to be clear study findings on PCC utilization and level of knowledge in SSA. This systematic review and meta-analysis will present pooled estimates on PCC utilization and level of knowledge among women in the reproductive age group and the correlation between these two parameters to effectively inform policy and practices and improve maternal and child health outcomes.
Methods
Eligibility criteria and review process
The review used published articles on the utilization of PCC and knowledge toward PCC among women in the reproductive age group in SSA. Studies published up to April 17, 2021 were systematically searched and identified in the following electronic databases: PubMed, Science Direct, Hinari, and Cochrane library. A compressive searching strategy was developed by consulting librarians and experts in searching articles for a systematic review and meta-analysis. Additionally, the references of appended articles were checked for further possible sources. All identified citations were collected and uploaded into EndNote version 8.0, and duplicates were removed. Studies were identified using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram (Supplemental Material). The Cochrane acronym PEO or PICOC, which stands for population, exposure, comparison, and outcomes (context), was used to decide on all key components before starting the review. Filters were applied to identify the relevant studies from the searches.
Inclusion criteria
Population: Studies conducted among women of reproductive age in SSA countries to determine the pool the utilization of PCC and a good knowledge level about PCC.
Study setting: Studies conducted at community level or institutional level.
Study design: All types of studies, including observational and interventional.
Publication type: Published articles written in English language. The most comprehensive and up-to-date versions were considered if studies were published in more than one report.
Study selection
The first step involved pre-screening of titles and abstracts by two independent reviewers to decide which studies would be retrieved fully. Following the screening processes, full-text articles were retrieved and included in the review if fulfilling the inclusion criteria. All relevant studies, including the thesis and relevant reports, were included. Two independent reviewers assessed the full text of selected citations in detail against the inclusion criteria.
Data extraction and quality assessment of the studies
Data were extracted by DW and DE and then assessed by a third author (ZH) to check for discrepancies. If any discrepancies were encountered, they were evaluated and resolved. Data were extracted using Microsoft Excel (Version 16.2) before the meta-analysis was conducted. Information was collected about the study author, year, country, and aims; participant characteristics (including population, sample size, setting, and inclusion/exclusion criteria); methods (study design, measures, analyses conducted); and main findings. All reviewers independently assessed the methodological quality of included studies using the Newcastle–Ottawa Scale (NOS).15,16 The studies which have at least six NOS criteria were considered to be high-quality studies.
Statistical analysis
Data extraction was performed using a Microsoft Excel spreadsheet, and the statistical analysis was performed using STATA version 14 statistical software. Standard error (SE) values were extracted from the studies for analysis since they are more commonly reported with a 95% confidence interval. When both SE and 95% confidence interval (CI) were not provided, SE was calculated using the formula (SE = √ (p × (1 − p)/n), where p is the proportion of the cases reported and n is the denominator of the prevalence estimate. 17
Statistical heterogeneity was assessed using the Cochran Q test (chi-squared statistic), the I2 test statistic, and by visual examination of the forest plot (overlap of confidence intervals). Cochran’s Q test was used to test the null hypothesis of no significant heterogeneity across the studies. 18 Cochran’s Q is calculated as the weighted sum of squared differences between individual study effects and the pooled effect across studies, using the pooling method’s weights. Cochran’s Q statistic follows a chi-squared distribution with k − 1 degree of freedom (df) where k is the number of studies. Cochran’s Q statistical heterogeneity test is considered statistically significant.
The I2 statistic was estimated because a percentage of variation (inconsistency) in the measures of association across studies is due to heterogeneity rather than chance. 19 The I2 statistic equals the quantity of Cochran’s Q minus its df divided by Cochran’s Q times 100%, I2 = 100% × (Q − df)/Q. The value of I2 ranges between 0 and 100%, where 0% indicates no observed heterogeneity and large values indicate increasing heterogeneity. 19 An I2 value of 25%, 50%, and 75% is considered as low, moderate, and high heterogeneity, respectively. 19 Egger’s weighted regression and Begg’s rank correlation tests were used to checking for publication bias (p < 0.05 is considered statistically significant).
Random-effects meta-analyses were used to combine the results of included studies and were measured as proportions of utilization and good knowledge level of PCC among the reproductive age group with 95% CIs.
In this review, test statistics showed significant heterogeneity among the included studies (I2 ⩾ 98%, p < 0.001). As a result, a random-effects model was used to estimate Der Simonian and Laird’s pooled effect. To identify the possible source of heterogeneity, meta-regression analysis was performed by taking the sample size and year of publication. However, none of them was found to be statistically significant (p > 0.05). The pooled effect was articulated in the form of an odds ratio (OR).
Result
Selection and identification of studies
A total of 1593 articles were obtained from electronic databases, and five studies were included from other sources. Among these, 55 were duplicates. Titles and abstracts of 1538 articles were checked, and 1397 were found to be irrelevant. In all, 121 articles were excluded after checking their full text. Finally, 20 articles were selected for inclusion in the meta-analysis, 14 articles for utilization, and 17 articles for knowledge, whereas seven studies were used to assess the association between the knowledge and utilization of PCC (Figure 1).

Flow diagram shows the study selection for a systematic review and meta-analysis on the knowledge level and utilization PCC in SSA study, 2020.
Description of included studies
All included articles were designed as cross-sectional studies. In total, 11 studies were facility based, and nine were community based, with a total population of 9075 participants. The included studies’ largest and lowest sample sizes were from studies conducted in Nigeria.20,21 Studies reporting the highest PCC utilization and highest good knowledge level about PCC, 72.6% and 70.7%, were conducted in Kenya and Nigeria, respectively.10,13 In all, 13 studies were from Eastern Africa,7,8,12.22–30 seven were from Western Africa,10,20,21,31–34 and there were no studies from Southern Africa. Based on the NOS for cross-sectional studies quality assessment tool, the score ranged from medium 7 to highest. 9 Regarding the response rate, 19 studies had a response rate of greater than 90%, and only one had a response rate of 88.7% 21 (Table 1).
Summary of the 20 included studies in the meta-analysis to a level of knowledge and utilization of PCC in SSA countries, 2021.
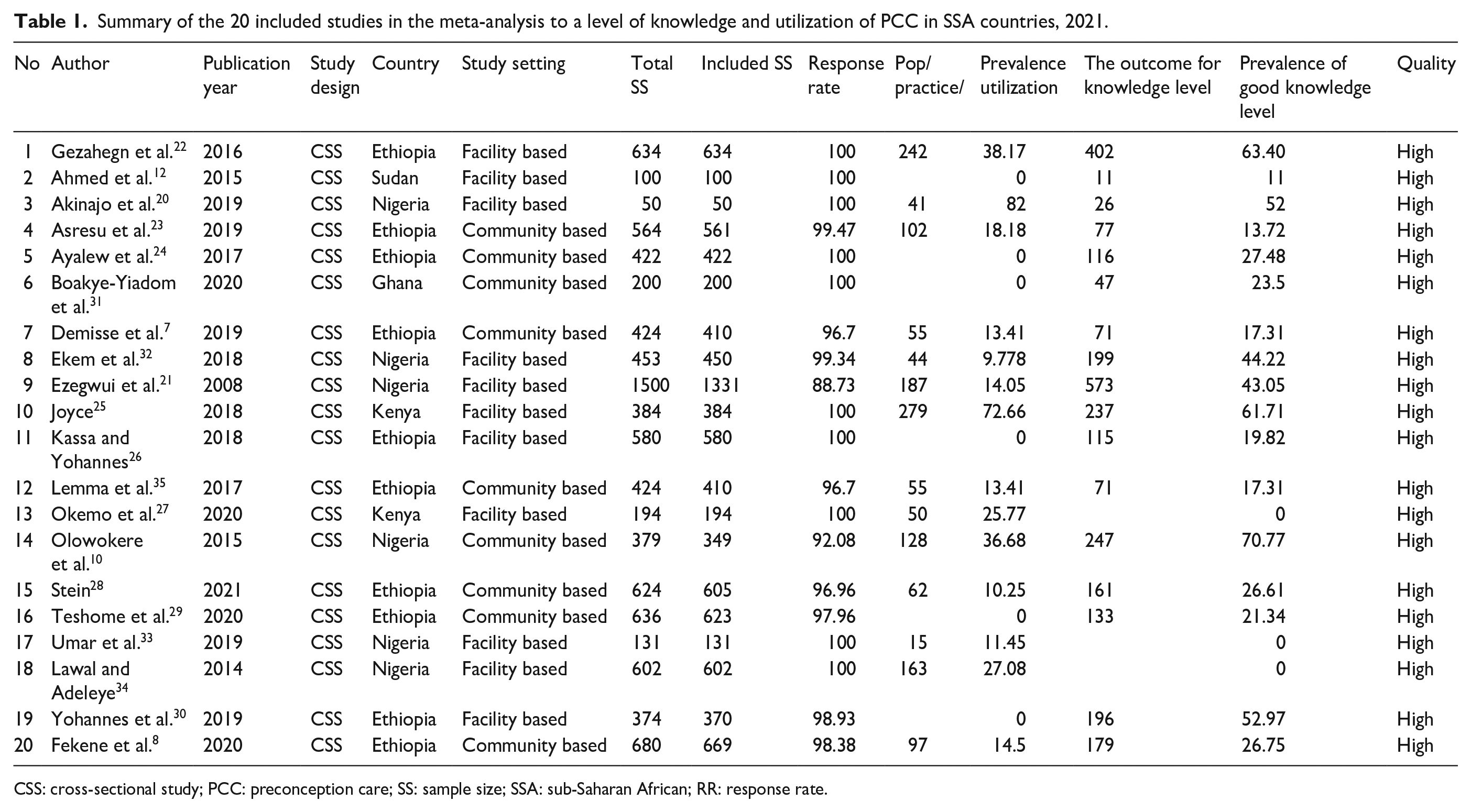
CSS: cross-sectional study; PCC: preconception care; SS: sample size; SSA: sub-Saharan African; RR: response rate.
Meta-analysis
The pooled prevalence of PCC utilization among the reproductive age group
In ALL, 14 of the included studies revealed a pooled prevalence of PCC utilization among women in the reproductive age group in SSA was 24.05% (95% CI: 16.61, 31.49) (Figure 2). High heterogeneity was observed across the included studies (I2 = 98.5, p = 0.000). Therefore, a random-effect meta-analysis model was executed to estimate the pooled utilization of PCC in SSA. From this meta-analysis, the pooled prevalence of PCC utilization in Eastern Africa was 25.73% (95% CI: 13.58, 37.88), whereas in Western Africa was 21.44% (95% CI: 13.60, 29.28) (Table 2).
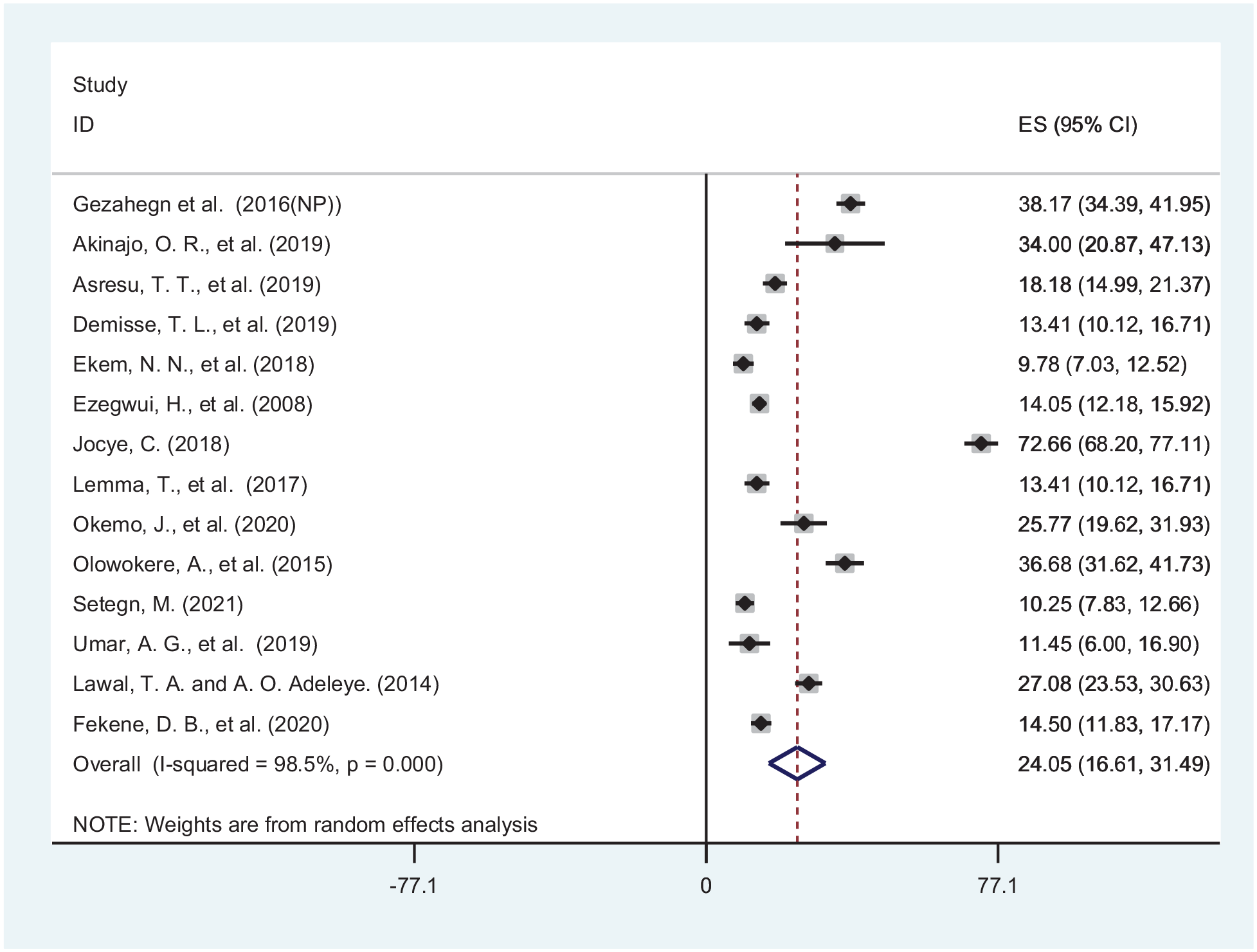
Forest plot of the pooled utilization of PCC in SSA, 2021.
Subgroup analysis for pooled utilization of PCC and knowledge level in SSA, 2021.

CI: confidence interval; PCC: preconception care; SSA: sub-Saharan African.
Knowledge level about PCC among the reproductive age group
The pooled prevalence of good knowledge level of PCC among women in the reproductive age group in SSA was 33.27% (95% CI: 24.78, 41.77) (Figure 3). Subgroup analysis for the knowledge level of PCC based on the regions of SSA showed that 29.93% (95% CI: 20.14, 39.45) in Eastern Africa and 41.52% (95% CI: 27.15, 55.89) in Western Africa (Table 2).
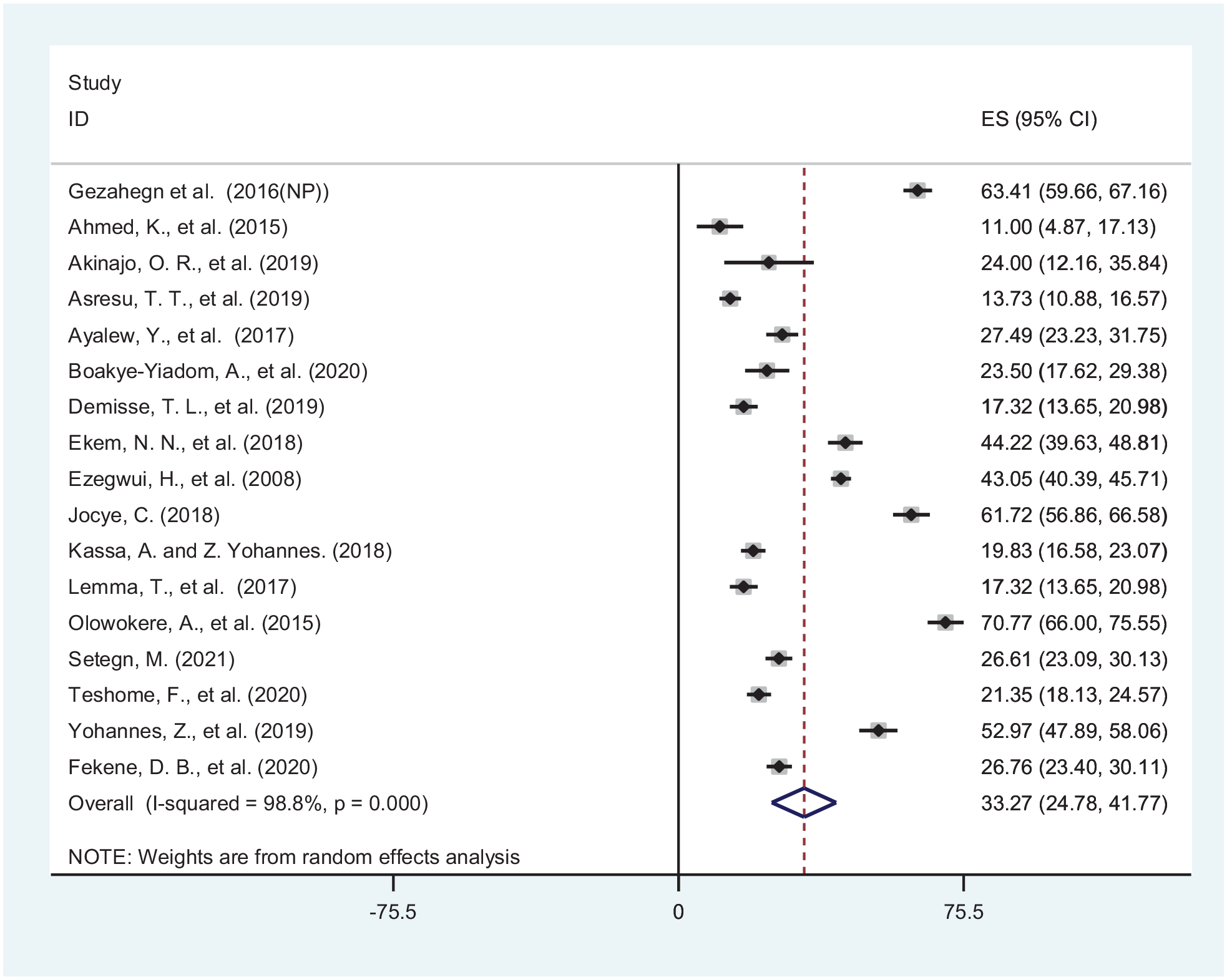
Forest plot of the pooled good knowledge level of PCC among reproductive age group women in SSA, 2021.
The association between PCC utilization and knowledge level
From included studies, seven showed the association between PCC utilization and good knowledge among women in the reproductive age group in SSA.7,8,20,22,23,28,32 From seven studies, five of the studies showed that there was a statistically positive association between PCC utilization and good knowledge level.7,22,23,28,32 In contrast, one study showed a negative association between PCC utilization and good knowledge 8 among women in the reproductive age group in SSA. The pooled finding of the analysis with 3379 participants showed that women in the reproductive age group with good knowledge levels were 2.35-fold more likely to utilize PCC than those with poor knowledge levels (OR: 2.35, 95% CI: 1.16, 4.76). The random-effect model was computed due to the highest heterogeneity (I2 = 92.3, p = 0.000) (Figure 4).

Forest plot of the association between knowledge level and utilization of PCC SSA, 2021.
Heterogeneity and publication bias
Significant heterogeneity was observed among the studies in terms of the pool PCC utilization and good knowledge level of PCC (i.e., I2 = 98.5%, p = 0.000 & I2 = 98.8%, p = 0.000, respectively). The random-effects meta-analysis model was used to estimate the Der Simonian and Laird’s pooled effect to address this. Meta-regression was conducted to identify the possible sources of heterogeneity using sample size. However, the finding was not statistically significant (p > 0.05). In this meta-analysis, possible publication biases were visualized through funnel plots. Symmetrical large inverted funnels resembled the absence of publication biases (Figures 5 and 6). Additionally, the probability of publication biases was tested using Egger’s and Begg’s tests. Egger’s weighted regression (p = 0.439) and Begg’s rank correlation test (p = 0.187) methods also showed no significant publication bias (p > 0.05). To detect the influence of one study on the overall meta-analysis estimate, sensitivity analysis was conducted using a random-effects model. However, it did not show strong evidence for the influence of a single study on the overall result.
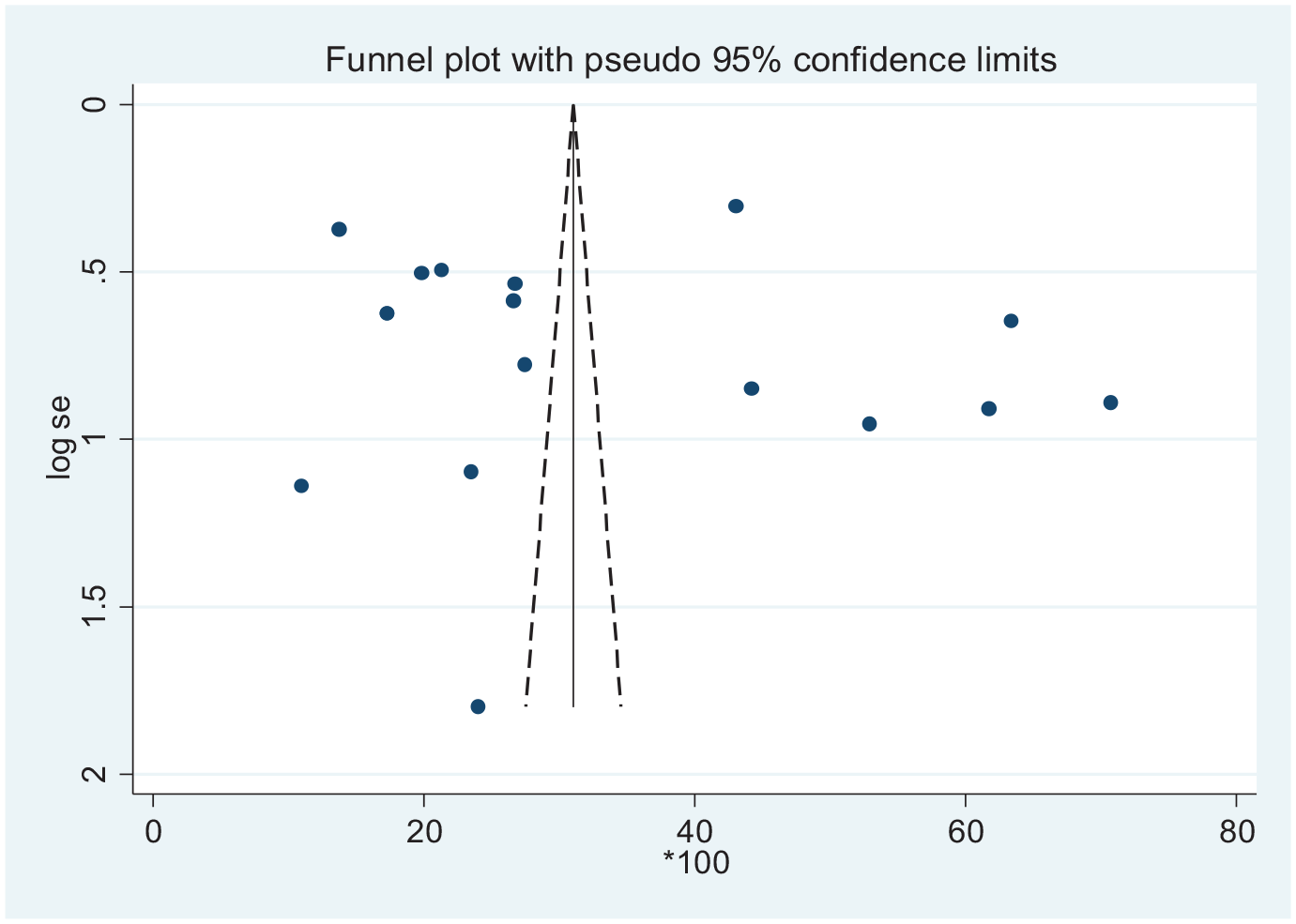
Funnel plot to test the publication bias of 17 studies.
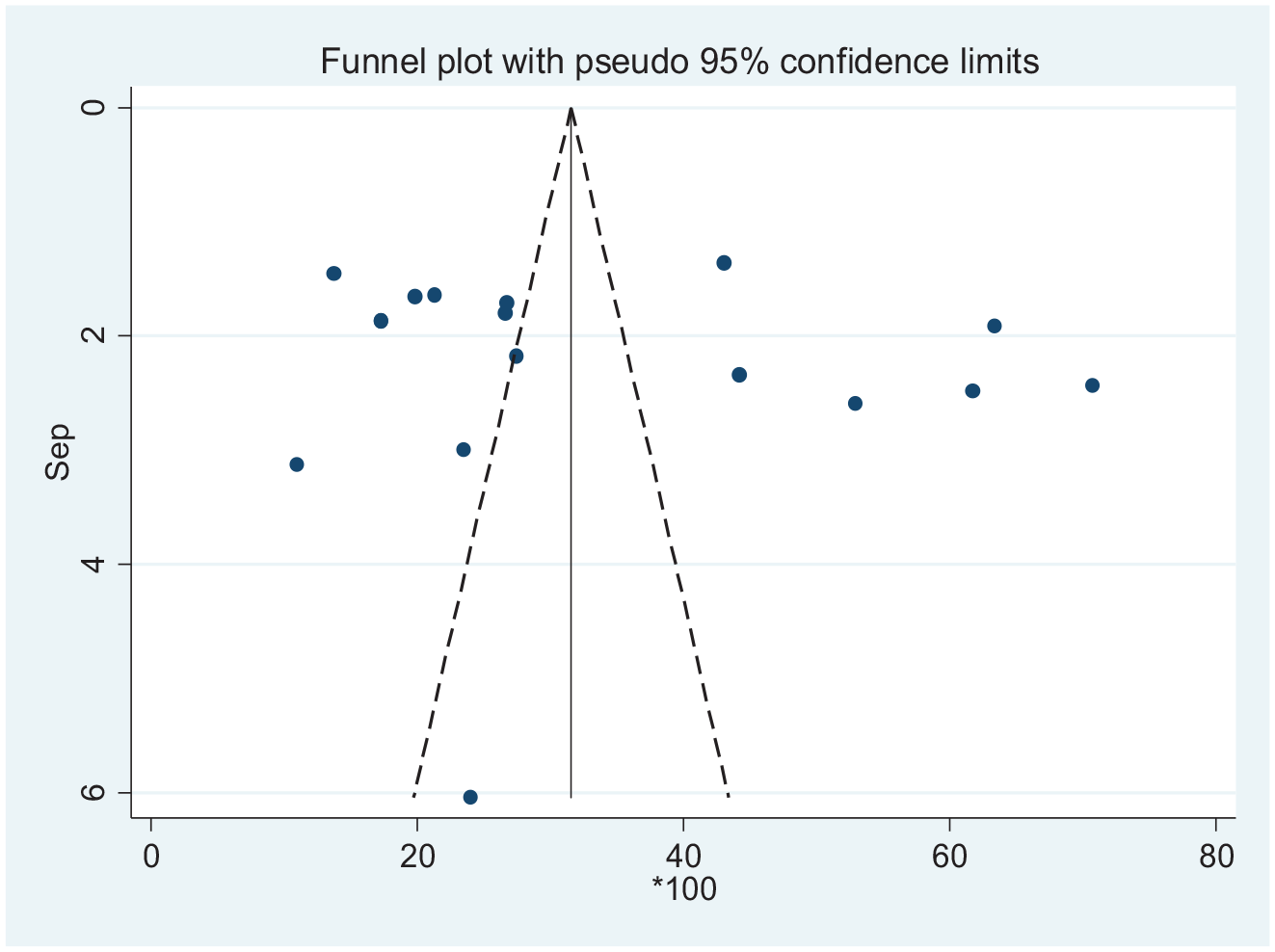
Funnel plot to test the publication bias of 16 studies.
Discussion
This review is the first to evaluate the literature and conduct a meta-analysis on PCC utilization and its association with the knowledge level of women in the reproductive age group in SSA. The findings provide insight into the recent PCC utilization and topographical distribution in SSA.
In all, 14 (24.05%) included studies revealed that only one-quarter of women in the reproductive age group in the SSA countries utilized PCC. This finding was consistent with a systematic review and meta-analysis conducted worldwide. 36 Although there have been reports about poor policies, guidelines, and low media coverage for PCC in SSA, the similarities in the findings between the utilization of PCC worldwide and SSA evidence might be explained by factors such as the differences in sociodemographic status, study setting, study participants, and healthcare system in these countries. However, it is noted that the utilization rate was higher in systematic reviews and meta-analyses conducted in countries such as Ethiopia, Nepal, Iran, Iraq, Sudan, and Brazil.12,37–41 We presume that this variability may be related to differences in each country’s study population’s education, culture, and study setting. For example, in the Ethiopian context, the evidence from the previous study was based on the study conducted a long time ago, and we hypothesize that as time increased, the health service demand might have increased as well.
In SSA, one-third (33.27%) of women in the reproductive age group had good knowledge about PCC. This finding was aligned with two studies conducted in Ethiopia and Utah37,42,43 but lower than a systematic review and meta-analysis conducted of studies from across the world, including Saudi Arabia, China, and Kenya.13,44–46 Women’s knowledge of PCC seemed to vary across countries, with some countries reported to have PCC guidelines and routinely practiced PCC. In contrast, others did not have such guidelines or routine practices on PCC. These findings highlight the essential issues, including that women’s knowledge of PCC is vital for alleviating adverse pregnancy outcomes and decreasing maternal and child death and illness.47,48 We hypothesize that the low level of knowledge reported in this study might be due to many factors related to social determinants of health (i.e., social environment factors in which people are born and live in, and shaped by the distribution of power, money, and other resources in society). 49 It is, therefore, reasonable to allude that, in the context of SSA and in women of reproductive age in the current study, the social determinants that would have affected their knowledge of PCC would be multifaceted including the low socioeconomic status, the discrepancy in the infrastructure of the health sectors, lack of promotion of PCC reported in the media, the insufficient attention given to PCC implementation by the healthcare system across the country, lack of preconception clinic at the health institution level, and low commitment of healthcare workers due to high case flow of the patient/clients.7,23,50
It was also noted that women in the reproductive age group with good knowledge were 2.35-fold more likely to utilize PCC than women with poor knowledge. This finding was consistent with three primary studies conducted in Ethiopia.2,7,8 It was not surprising given that social determinants of health, 49 including poverty, poor education, and poor infrastructure affect multiple health outcomes in populations across settings, with SSA no exception.
Women with some basic level of knowledge were more aware of the costs associated with not using PCC services. Moreover, comprehensive knowledge of PCC would provide better insight and awareness, positively impacting the overall health and life of women, newborns, and the more comprehensive, communitywide community.
Strengths and limitations
The main limitation of this review was the need for studies from the southern region of SSA countries, which might limit the generalizability of the study to the southern region of SSA. Moreover, the pooled utilization of preconception and knowledge level was not separately estimated for different components of PCC services due to a lack of separation in reporting these components from the included studies. Separate analysis for each specific component of PCC could be more informative for the scientific community and other beneficiaries; however, the primary interest of the review was the general utilization and knowledge level PCC among women in the reproductive age groups without differentiating the specific components. Measurement for knowledge level could be different in the included studies.
Conclusion
In SSA countries, the utilization of PCC and good knowledge level about PCC among women of reproductive age groups remain low compared to the 2019 WHO report. However, the study found a positive association between good knowledge and utilization of PCC among women in the reproductive age group. These findings provide insightful information and would be imperative to launch programs to uplift the knowledge level about PCC among women in the reproductive age group in SSA countries.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231153511 – Supplemental material for Preconception care in sub-Saharan Africa: A systematic review and meta-analysis on the prevalence and its correlation with knowledge level among women in the reproductive age group
Supplemental material, sj-docx-1-smo-10.1177_20503121231153511 for Preconception care in sub-Saharan Africa: A systematic review and meta-analysis on the prevalence and its correlation with knowledge level among women in the reproductive age group by Demelash Woldeyohannes, Yohannes Tekalegn, Biniyam Sahiledengle, Zeleke Hailemariam, Desta Erkalo, Abraham Zegeye, Habtamu Tamrat, Akililu Habte, Aiggan Tamene, Fitsum Endale, Biruk Ertiban, Tekle Ejajo, Lolamo Kelbiso, Lombamo Liranso, Fikreab Desta, Dejene Ermias, Lillian Mwanri and Joanne C. Enticott in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to acknowledge all Liberians for their cooperation.
Authors’ contributions
DW: Conception of the research protocol, study design, literature review, data extraction, data analysis, interpretation, and drafting of the manuscript. DW, BS, YT, ZH, and DE: data extraction, quality assessment, data analysis. AZ, AT, FE, AH, HT, LL, BE, TE, DE, LM, LK, FD, DE, and JE: reviewing of the manuscript. All authors have read and approved the manuscript.
We have submitted this manuscript to a journal before submitting it to this journal and its preprint was online; the manuscript is withdrawn from that journal.
Availability of data and material
This study was based on a literature review of published studies in sub-Saharan Africa. Anyone who needs to access the data can contact the author concerning the studies included in the analysis. The reference list can also be used to access the articles directly.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participation
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Consent for publication
Not applicable.
Informed consent
Not applicable.
Trial registration
Not applicable.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.