
Abstract
Objective. Congenital hypothyroidism (CH) is a treatable condition with a good outcome if diagnosed promptly. However, neonatal screening programs are not routinely available in developing countries in Pakistan. Method. To highlight the practices of newborn screening in Pakistan, an online survey was conducted. Google forms were circulated to national pediatric societies and hospitals. Results. Out of 341 respondents most were consultant pediatrician (n = 212, 62.17%) followed by residents (n = 80, 23.41%). Majority, (n = 309, 90.6%) believed it was essential to screen all newborns for CH. However, in practice only (n = 141, 41.3%) were offering screening. The most common reasons cited for not screening was the cost of test (n = 110, 32.2%), non-availability of testing services (n = 29, 8.5%) and lack of any implemented screening policies in the hospitals or national guidelines (n = 20, 5.8%). Differences in practice were also observed at provincial levels (P < .05). Conclusion. This survey highlights marked variation in CH newborn screening practices.
Introduction
Congenital hypothyroidism (CH) is a treatable with a good outcome if diagnosed early and treatment started within the first 2 weeks after birth. Newborns with CH usually do not have any clinical signs and symptoms at the time of birth. It takes a few weeks to a month before clinical features of hypothyroidism start presenting, prompting a physician to initiate the relevant clinical investigation. The delay in diagnosis leading to delayed treatment is an important factor which results in long-term cognitive and physical impairment. 1 The most effective way to prevent this delay in diagnosis and to promote a favorable outcome is by introducing effective neonatal screening programs. Neonatal screening programs are essential pillars of public health and well established in many developed countries but are yet to be a norm in developing countries. 2
On a global scale, approximately 29% (37 million out of 130 million) newborns are screened annually, leading to the identification of 12 000 newborns with CH. We can estimate that approximately 30 000 newborns with CH in a year remain undiagnosed due to the absence of neonatal screening programs in their respective countries. Interestingly, incidence of CH has doubled over the last four decades from 1 in 4000 live birth (1970) to 1 in 2000 live birth (2010). It is believed that this doubling over the last decade is a result of the reduction of TSH cut offs which enabled the identification and treatment of milder cases. Moreover, another reason is the increase in high risk population like preterm and small for gestational age newborns. 3 The incidence of CH in developed countries – where neonatal screening programs are well established ranges between 1:2000 and 1:4000 newborns with a significant variation among different ethnic groups. 4 The incidence of CH significantly increases within twin/multiple births and consanguinity. 5 The highest known incidence of 1:581 has been reported in Iran. 6 The incidence reported in preterm and very low birth weight newborns (<1500 g) is up to 1:400 cases which is considerably higher than term, normal weight newborns. A female to male ratio of 2:1 is seen in many studies published till date. 7
In Pakistan, there is no national screening program for CH. 8 The incidence of CH is reported to be 1:257 in healthy newborns with the limited data available from an individual center. 9 Incidence in low birth weight/pre-terms is largely unknown due to lack of population-based studies, however a frequency of 12% is reported from local hospitals.10,11 Data reported from tertiary healthcare hospitals worldwide puts the frequency at 2.6% which is nearly half of data (4.5%) reported in the South Asian region. 12 A study from a tertiary healthcare hospital of Pakistan with an ISO certified laboratory analyzed 5000 neonates and reported the incidence to be 1:1000. 13
All developed countries and some developing countries have implemented neonatal screening programs successfully. The heel prick method (24-72 hours) is preferred, and samples are transferred to national testing laboratories. 14 In pre-termers with very low birth weight, critically ill neonates (at the time of sample), neonates with down syndrome, twin/multiple births or in those that received a transfusion before sampling, a second sample is advisable for screening at 2 to 4 weeks of birth. 15
Three major techniques are used for screening: simultaneous T4 and TSH levels, initial T4 with subsequent TSH (if T4 is low) and initial TSH with subsequent T4 (if TSH is high). No technique is preferable to any other. All techniques detect CH with a sensitivity of 97.5% and specificity of 99%, however, each technique has its own pros and cons. 16 Initial TSH with subsequent T4 can detect subclinical hypothyroidism but can miss central hypothyroidism, while initial T4 with subsequent TSH can detect central hypothyroidism but miss patients with subclinical hypothyroidism. 17
Different TSH cut off for positive screening were used depending on methods of screening. For serum TSH of >40 mIU/L and whole blood TSH of >20 mIU/L are considered elevated. Whole blood cut off are one-half of serum units and hematocrit values can also alter the TSH levels. 18
In developing countries, like Pakistan, lack of national screening program, delayed diagnosis of CH, different cut off used by physicians to start treatment and lack of national guidelines to manage it, lead to poor prognosis of this easily manageable condition. By improving our national services and implementation of the right guidelines we can make these children a productive member of our society and can reduce the financial burden on our national healthcare system. This survey was undertaken with the aim to determine the gaps in our knowledge, attitude, and practice regarding newborn screening for CH. It is expected that identifying these gaps will aid us in implementing national guidelines and recommendations which will contribute in addressing CH care in Pakistan.
Method
An online cross-sectional survey using Google form regarding newborn congenital hypothyroidism screening was conducted from September 2023 to November 2023. These Google forms were circulated through social media pages, WhatsApp groups of national pediatric societies and to focal persons of different major public and private sector pediatric hospitals of Pakistan. The inclusion criterion included pediatric residents, consultants, fellows, general practitioners involved in newborn care and pediatric and adult endocrinologist and fellows practicing in Pakistan. Incomplete responses were excluded.
Our questionnaire comprised of 4 parts. The first part of the survey included basic responder information such as name, age, gender, designation, place of work, province, city, and number of CH patients with delayed presentation visits per month in their set up and their most common presentation.
The second part was about their knowledge of newborn screening for CH. It included 7 questions related to the importance of screening, when to screen, how to screen, which level of TSH to be used as a cut off to diagnose CH, which level they considered as equivocal, what are the symptoms of CH and at what time of the day did they advise to take thyroxine.
The third part of survey was about responders and their hospital practices regarding newborn screening of CH. It included ten questions including: was CH screening offered to all newborns, who paid for the screening, which method was practiced for CH screening, were critical results systematically reported, what relevant procedures were followed diagnosing a newborn with CH, which tests were advised in the setup for screening, which preparation of thyroxine was used and how did they follow up these newborns. The last part of the survey related to recommendations to improve newborn screening system for CH in Pakistan. The survey questionnaire was pilot tested among a group of colleagues before circulating to the wider participants.
Statistical Analysis
All information was collected from a Google form derived excel sheet. Data was transferred to SPSS v 27 for statistical analysis. Qualitative data was analyzed as a mean and standard deviation, quantitative data as frequency and percentages, and finally, Chi-square and binary logistic regression were also applied. A P-value of <.05 was taken as significant.
Ethics approval and informed consent
Institutional Review Board and ethical approval was taken Shifa International hospital (IRB no: 0425-23). The survey was conducted anonymously and participation by physicians was voluntary.
Results
Characteristics of Respondents
A total of 341 physicians participated in the study from all over Pakistan. Males were 179 (52.5%), females were 150 (43.9%) and 13 (3.5%) physicians did not reveal their gender identity. The mean age of participants was 37.7 + 9.3 years (25-73 years). Most of the participants were consultant pediatrician (n = 212, 62.17%) as shown in Table 1. Maximum participation was seen from Punjab, the largest province in Pakistan followed by Khyber Pakhtunkhwa and Sindh as shown in Tables 2 and 3.
Designation of Study Participants.

Provincial Distribution of Study Particpants.

Practice Differences Among Provinces.

Place of Work
Most of the participants were working in public sector hospitals (n = 202, 59.2%), followed by private sector hospitals (n = 79, 23.1%), both private and public sector hospitals (n = 54, 15.8%), and private clinics only (n = 6, 1.7%). Only 57 (16.7%) participants affirmed that their hospitals/ workplace has newborn CH screening policy. The practices of newborn screening were better in these hospitals (P < .05).
Knowledge and Practice
Among the study participants, (n = 309, 90.6%) answered that it is essential to screen all newborns for CH. However, in practice only (n = 141, 41.3%) participants were offering CH newborn screening. The designation of physicians and workplace were found to be important determinants of practice for newborn CH screening (P < .05). The majority (n = 200, 58.7%) were not screening newborns for CH. Most of the participants (n = 332, 97.4%) were aware of the symptoms of CH. We applied binary logistic regression model to predict if physicians would actively engage in CH newborn screening. The model predicted that the odds of a physician saying no are 1.35 times higher than those saying yes to do you think it’s essential to screen, with a 95% CI (1.126-13.267). The Hosmer and Lemeshow test value is 0.968 so the model adequately fits the data. Hence, there is no difference between the observed and predicted model. Only 26% change in the observed variable can be accounted to the predictor variables in the model.
Binary Logistic Regression
Hosmer and Lemeshow test.

Model Summary.


Variable (s)entered on step1: Designation, Place of work, province, do you think it’s essential to screen.
The most common reasons cited for not getting screening for CH was the cost of screening test (n = 110, 32.2%), followed by non-availability of testing services specially in remote areas (n = 29, 8.5%) and lack of any implemented screening policies in the hospitals or national guidelines (n = 20, 5.8%). Some physicians 19 (5.5%) suggested that it is not important to screen all newborns. In their estimation, testing should only be done if family/maternal history of hypothyroidism or baby is symptomatic. Seven (2%) physicians stated that CH was not a common condition in thier practice. The reasons were statistically significant when compared between the designation, place of work and based on the physician’s knowledge if testing was essential (P < .05).
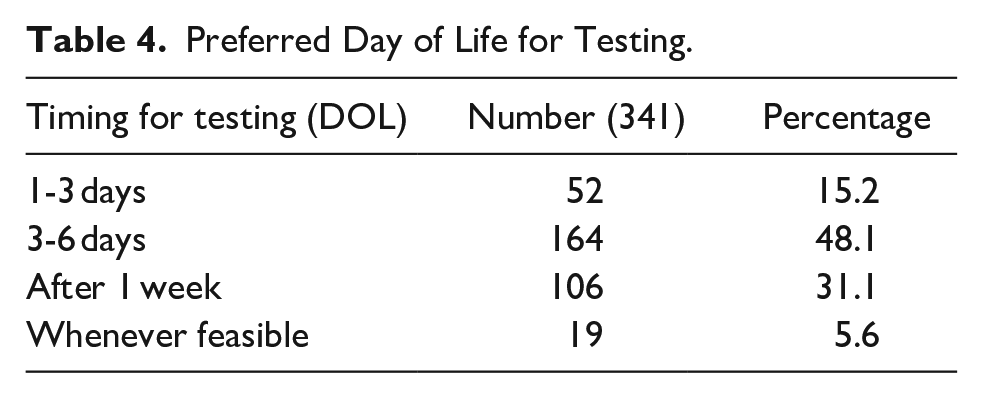
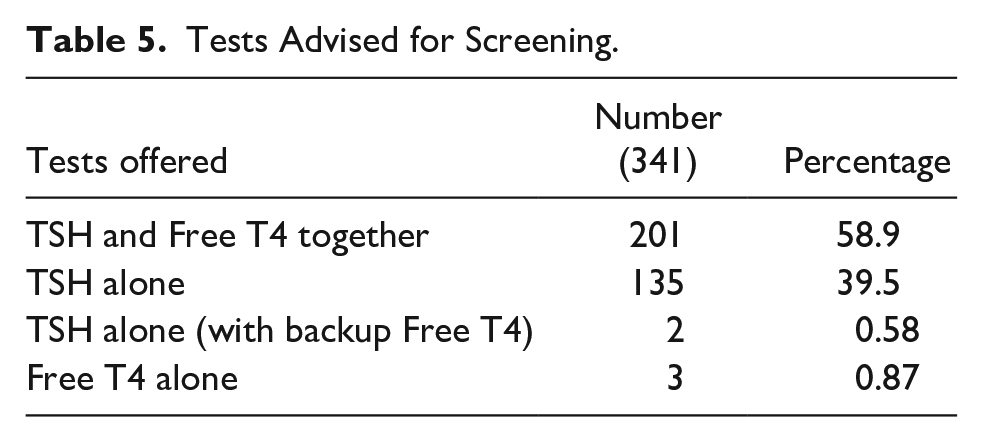
The preferred time suggested for testing for CH screening by majority of physicians (n = 164, 48%) was 3 to 6 days as shown in Table 4. TSH along with free T4 was opted by most participants (n = 201, 58.9%) for newborn screening of CH, followed by TSH alone in 135 (39.5%) participants (Table 5).
Preferred Day of Life for Testing.
Tests Advised for Screening.
An important aspect checked was the physician’s practice about the level of TSH they consider appropriate for CH diagnosis and initiation of treatment. Interestingly, marked variation of responses was seen in this regard with majority (n = 106, 36.4%) responding that TSH level > 10 is the cut off to starting treatment as shown in Table 6. The cutoffs used were not found to be significantly associated with designation of the physician (P = 0.19).
Cut off TSH Levels.

Venipuncture for blood sampling was the most preferred technique for sampling by majority participants (n = 230, 67%) and heel prick on filter paper/ Guthrie was practiced by 103 (30%) participants. Most of the participants’ responded that their hospitals did not contain any reporting system for critical laboratory values (n = 228, 67%). Only 108 (31.6%) physicians were working in hospitals with reporting facilities.
Most CH screenings are paid out of pocket by parents (n = 288, 84.4%). Only 40 (11.7%) participants reported their hospital supported CH screening and 13 participants reported that (13.81%) it was done through non-governmental organizations (NGOs).
Management
When inquired as to how do physicians manage patients with CH, majority reported that they start treatment as well as manage patients themselves (n = 195, 57.2%). Some physicians (n = 129, 37.8%) refer the patient to pediatric endocrinologist, while (n = 10, 2.9%) physicians responded that they would start treatment and then refer the patient to pediatric endocrinologist for further management. Four (1.17%) physicians were not sure what to do and preferred to discuss with their senior physician.
Majority of the respondents (n = 271, 79.4%) were aware that thyroxine is the treatment for CH, however, some participants (n = 15, 4.39%) were not aware of the treatment while (n = 55, 16.1%) participants did not respond to this question.
The majority (n = 320, 94.1%) responded that tablet thyroxine should be taken early morning before breakfast, 10 (2.9%) responded anytime during the day, 7 (2%) responded that they are not aware and 3 (0.9%) advised at night. When physicians were inquired about how frequently they follow up patient with CH, (n = 94, 27.5%) responded after 2 weeks, (n = 157,46%) after 1 month, 17 (4.9%) said after 2 months and 51(14.9%) responded after 3 months.
Regarding further workup, 135 (39.5%) responded that they will advise both ultrasound neck and thyroid scan, 32 (9.3%) advised thyroid scan only and 50 (14.6%) advised ultrasound neck only. No response was received from 70 (20.5%) physicians.
Delayed diagnosis
Delayed diagnosis of CH was reported by most participants. The majority reported 1 to 5 patients per year (n = 210, 61.5%), 50 respondents reported 6 to 10 patient/year (14.6%) and 49 (14.3%) reported more than 10 patients. Most common delayed presentation of CH observed were developmental delay, constipation, prolonged jaundice, coarse facial features, hoarse cry, protruding tongue, lethargy, hypotonia, dry skin, and umbilical hernia.
Future Recommendation
We received a variety of responses for implementing the newborn congenital hypothyroidism screening in Pakistan. Listed below in order of frequency:
Implementation of Newborn Screening for CH in Pakistan
Free mandatory screening as a national health policy by the government of Pakistan.
Making legislation and national guidelines to be followed by doctors for CH screening.
Active collaboration between government, private sector hospitals and NGOs for implementation at the national level.
Lowest screening cost possible to be decided by the government in collaboration with private laboratories in Pakistan (Incase free services not possible).
In private hospitals it was advised to include the cost of testing in maternal health care plans.
Mandatory requirement before issuing a birth certificate by national database and registration authority (NADRA).
Making it part of the first visit for expanded program of immunization (EPI) which is a free program run by the government of Pakistan. The first vaccine is given in the first week of life according to EPI schedule.
Awareness
Education of health care professionals including GPs, pediatricians, neonatologists, gynecologists, trained birth attendants about significance of newborn screening of CH through workshops and social media campaigns.
Education of parents regarding the significance of timely screening and the aftermath of delayed diagnosis.
Facilities
Doctors working in rural and suburban areas advocated the need of testing facilities/ kits at tehsil and district level.
Guthrie and heel prick testing should be made available.
Discussion
This survey highlights marked variation in CH newborn screening practices at the national level. We managed to survey physicians from all parts of Pakistan. There were significant differences of practice observed at provincial levels (P < .05). Physicians from Balochistan, Azad Jammu & Kashmir reported no practices of screening newborns. Balochistan is the largest province by area yet the most underdeveloped, lagging in terms of medical infrastructure. 19 The lack of universal health coverage in Pakistan contributes to the lack of essential healthcare services. 20
The survey mainly involved pediatricians and pediatric residents in training. Most of the doctors (n = 206, 60.4%) were working in public sector hospitals out of which only 21(6.1%) said that their hospital had a CH screening policy. More than 40% of the population faces poverty in Pakistan and their healthcare needs are dependent on public sector hospitals. 21 However, the government run healthcare is not properly equipped to cater to the need of the masses due to limited spending by the government on healthcare. 22 The deficiency in newborn screening in Pakistan can be attributed to the absence of policy at the national level as well as limited facilities in public run hospitals. 23 Only 57 (16.7%) participants affirmed that their hospitals/ workplace has newborn CH screening policy. The practices of newborn screening were better in these hospitals (P < .05).
It was ironical to note that although (n = 309, 90.6%) physicians believed it is essential to screen CH, only 141(41.3%) were doing it in practice. On the contrary, 32 (9.3%) answered that screening was not essential. The study highlights huge differences between knowledge and practice necessitating the need for national practice guidelines like other regional countries. 24 CH remains the most common preventable cause of neurodevelopmental delay worldwide. 25
Most physicians (n = 201, 58.9%) preferred TSH along with Free T4 for screening, followed by TSH alone by (n = 135, 39.5%) participants. The majority wanted to screen between 3 and 6 days of birth, followed by respondents who wanted to screen after 1 week of birth. The AAP recommends that screening should be done after 24 hours of birth preferably between 48 and 72 hours or before hospital discharge or within the first week of birth whichever is sooner. 26 However, 19 (5.6%) physicians responded that they would offer screening whenever feasible, which can lead to delayed diagnosis of CH. TSH level greater than 10 mIU/ml was used for diagnosing CH by the majority (n = 124, 36.4%). The recommended TSH of greater than 20 mIU/ml was used by 109 (31.3%) only. One third of the study respondents were using cutoff of >30, 40 or 50 mIU/ml. This highlights a lack of knowledge of physicians with respect to CH diagnosis. The AAP recommends starting treatment at TSH > 20mIU/l and following up with free T4 levels. This calls for the need to creating greater awareness and improving practices according to evidence based guidelines. 27
The respondents demonstrated knowledge of available treatment in the form of tablet thyroxine. Most of them would start treatment on their own while some of them would consult at a later stage with pediatric endocrinologist. It is also very important that all physicians have the knowledge to start treatment in appropriate doses to manage CH as there is a lack of pediatric endocrinologists in small cities and towns in Pakistan. 28 Early diagnosis and treatment within 2 weeks of birth are imperative. However, delayed diagnosis and presentation are a common case scenario in Pakistan. 29 This adds to the burden of developmental delay, morbidity, and DALY (disability adjusted life years) to an already improvised economy. 30 CH newborn screening is cost effective and easily treatable with good outcomes when identified at an early stage.
The major reason for not offering CH screening was the cost and lack of testing facilities in remote areas. We received different recommendations to implement the CH newborn screening at the national level. The state ownership and funding, national guidelines on testing, treating, and availability of testing facilities is most important. 31 Need for creating awareness for CH screening not only among physicians but parents can also prove beneficial in implementing practices. 32 The respondents gave some valuable suggestions for monitoring of screening program and to link it up with national immunization (EPI) program of Pakistan or make it a mandatory requirement for birth registration. The study highlights that physicians training, seminars, workshops are needed at all levels of healthcare provision to make it a national program. The success of newborn screening program will need a greater degree of advocacy, priority, funding, policies, as well as an active role of pediatricians. 33
Limitations of this study include unequal responses from each province, limited number of participants and crossectional nature of the study. However, the results can be used to improve the practices at the national level.
Conclusion
The study highlights variation in practices and knowledge of newborn screening for CH in Pakistan. Pediatricians continue to see delayed diagnosis of CH adding to disability and morbidity. The lack of national policies, testing facilities and lesser advocacy on significance of newborn screening is resulting in suboptimal practices.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241293526 – Supplemental material for A National Survey on Congenital Hypothyroidism Newborn Screening in Pakistan
Supplemental material, sj-docx-1-gph-10.1177_2333794X241293526 for A National Survey on Congenital Hypothyroidism Newborn Screening in Pakistan by Sabeen Abid Khan, Sommayya Aftab, Yasir Naqi Khan, Mehrunnisa Yasir, Kashan Arshad, Noor ul Ain Mehak, Syed Kaleem ur Rehman, Abida Faiztalpur, Shazia Bahar, Ayesha Abdul Razzaq, Sajjad Habibullah, Aamir Naseem, Syed Saddam Hussain, Hina Sattar, Mohammed Usman, Aqeela Ayub, Rehmana Waris and Taeed Ahmed Butt in Global Pediatric Health
Footnotes
Acknowledgements
Prof. Farhan Hanif Siddiqi for correction of English language.
Author Contributions
1. SAK: manuscript design, data collection, analysis, drafting.
2. SA: manuscript design, data collection, analysis, drafting.
3. YNK: data collection, analysis, manuscript writing.
4. MY: data collection, data analysis, writing, drafting.
5. KA: data collection, data analysis, study design.
6. NAM: data analysis, writing, drafting.
7. SKR: data collection, data analysis, writing.
8. AFT: data collection, data analysis, writing.
9. SB: data collection, data analysis, writing.
10. AAR: data collection, data analysis, writing.
11. SH: data collection, data analysis, writing.
12. AN: data collection, data analysis, writing.
13. SSH: data collection, data analysis, writing.
14. HS: data collection, data analysis, writing.
15. MU: data collection, data analysis, writing.
16. AA: data collection, data analysis, writing.
17. RW: data collection, data analysis, writing.
18. TAB: data analysis, review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Institutional Review Board and ethical committee approval was taken from Shifa International Hospital, Islamabad, Pakistan. IRB approval number: 0425-23.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.