
Abstract
Objectives. Newborn screening for critical congenital heart disease (CCHD) was added to the Recommended Uniform Screening Panel in 2011, and states have been gradually adding pulse oximetry as point-of-care screening to panels. Few data are available on the effectiveness of pulse oximetry as a mandated screening. This study describes outcomes of the first year of screening in Maryland. Methods. A web-based data collection tool for screening results and outcomes, eScreener Plus, was utilized. Data collected from the start of screening from September 1, 2012, to December 31, 2013, were analyzed. Well-baby nursery data were evaluated separately from neonatal intensive care unit (NICU) data to determine whether setting influenced effectiveness. Results. In the first 15 months of newborn screening for CCHD in Maryland, 4 asymptomatic infants were diagnosed with a critical cardiac condition by newborn screening. Eleven infants passed but were later identified with a primary or secondary target condition. Seventy-one percent of infants with CCHD were identified prenatally or by clinical signs and symptoms. Pulse oximetry screening for CCHD had a specificity of more than 99% in both the well-baby nursery and the NICU. Sensitivity in the well-baby nursery was 10% and 60% in the NICU. Conclusion. Further investigation and interpretation of specific protocols that were used and outcomes of screening is needed for continued refinement of the well-baby algorithm and NICU protocol development. Pulse oximetry screening in newborns provides valuable clinical information, but many infants with CCHD are still not identified with current protocols.
Introduction
Congenital heart defects occur in slightly less than 1% of infants born in the United States, and one quarter of those infants will have a critical congenital heart defect (CCHD), which may cause significant morbidity or mortality if not detected early. 1 Pulse oximetry is a noninvasive test that can identify asymptomatic hypoxemia in neonates.
On September 1, 2012, Maryland became the third state in the nation to begin mandated newborn screening for CCHD. Reporting of public health surveillance data for CCHD screening is critical to the evaluation and improvement of this new procedure’s efficacy. While large studies have provided preliminary data on the sensitivity, specificity, and positive predictive value of CCHD screening2-4 and feasibility has been demonstrated in a research setting, 5 results from implementation in a public health setting provide valuable information regarding the performance of current protocols in population-based screening. Maryland also has a prenatal detection rate for CCHD of approximately 70%, which affects the utility of pulse oximetry screening. Finally, infants in the neonatal intensive care unit (NICU) were excluded from previous studies, and several states, including Maryland, screen all babies, resulting in the need to examine performance in various clinical settings.6,7
Methods
Setting
Maryland has approximately 72 000 births a year in 32 birth hospitals, 2 birthing centers, and home births. CCHD screening documentation was added to the web-based reporting system for infant hearing screening and birth defects surveillance. Documentation includes whether a child was screened, screening outcome, the date and time of the screen, and optional pulse oximetry readings. Recording of actual saturations remains optional given the potential for errors and the additional data entry burden. In addition to pass/fail, options for screening outcomes include parent refusal and physician override. The latter category was created to identify infants who did not clinically require screening due to prenatal diagnosis, onset of symptoms with cardiac evaluation before screening, or an adequate echo before screening. All data management and analysis were conducted using SAS 9.3.
Sample
From September 1, 2012, to December 31, 2013, there were 92 728 births documented in the eScreener Plus (eSP) system: 83 381 were well babies, and 9247 were admitted to the NICU. Seventy-four infants in the well-baby nursery and 267 in the NICU died before discharge from the hospital and were excluded from this analysis. A contact person at each of the 3 centers that provide the majority of cardiac surgery care to infants in Maryland was established for identification of false negative screen results. If an infant presented to one of these centers with a CCHD diagnosis not identified at birth, the contact person provided this information to the screening program.
Data Collection
Maryland’s Expert Panel approved the CCHD screening algorithm endorsed by the American Academy of Pediatrics (AAP) and American Heart Association (AHA), and web-based training as well as a website were provided with resources for families and providers. Protocols used in all birth hospitals have not been obtained, but the majority utilize the AAP/AHA protocol.
Additionally, a system of surveillance and quality assurance needed to be developed. The eSP system has been used in Maryland for several years to provide surveillance and follow-up of newborn hearing screening. All hospital births in Maryland are captured on that system, along with demographic information. A module was added to collect data on CCHD screening with fields to include the results of the CCHD screen (pass/fail/refused), as well as information on the clinical evaluation of children who had a positive screen and their eventual diagnosis. Another option, “physician override,” was provided for infants who had a prenatal diagnosis of CCHD or had a diagnostic echocardiogram before screening.
The eSP database allows for the creation of reports based on user-selected criteria. These reports, as well as typed notes in the system regarding infants with diagnoses of CCHD, were used to develop counts of total births, numbers screened, screening outcomes, and CCHD diagnoses. Diagnoses other than CCHD identified after a positive screen were requested but this information was rarely provided. Sensitivity and specificity were manually calculated based on these data.
Data collection beyond screening results is not mandated by regulation and was difficult to collect. The newborn screening nurse contacted birth hospitals to obtain information on infants who did not have screening or outcome results documented, but response rates were poor. Infants presenting with undetected CCHD after their newborn hospitalization were identified by 1 of the 3 pediatric cardiology centers serving the state and these programs notified the newborn screening program. Finally, the Birth Defects Reporting System for Maryland is housed in the same office as Newborn Screening Follow-Up and CCHD identified at birth or on a death certificate would be communicated to the newborn screening follow-up nurse.
Ethical Approval and Consent
Ethics approval and informed consent was not sought: this article reports on aggregate outcomes of a mandatory newborn screening program. Analysis was done on anonymous data collected as part of routine clinical care.
Results
Results are reported separately for the well-baby nursery and the NICU. The 12 target conditions for newborn CCHD screening are listed in Table 1.
Target Conditions for CCHD Screening (per CDC a ).

Abbreviations: CCHD, critical congenital heart disease; CDC, Center for Disease Control and Prevention.
Source: CDC, National Center for Birth Defects and Developmental Disabilities, https://www.cdc.gov/ncbddd/heartdefects/cchd-facts.html.
Well-Baby Nursery Screening Outcomes
From September 1, 2012, to December 31, 2013, there were 83 380 births documented in the eSP database, with 74 infants deceased. This left 83 306 infants eligible for screening. Of these, 78 542 had a pulse oximetry screen reported, 63 were reported as “physician override,” 52 were documented as “not screened,” including 8 who had parents who refused the screen.
Overall, a total of 94.4% of eligible well babies were evaluated for CCHD. A flow chart of the outcomes of screening in the well-baby nurseries is presented in Figure 1. Twenty-eight infants had a positive CCHD screen. Of those, one infant was identified with a target condition (tricuspid atresia). One infant had a significant noncardiac findings, and required intervention for pneumonia. Six infants had non-CCHD, 7 had delayed transition, and 13 did not provide information regarding outcomes even on phone follow-up. We do know from contact with the pediatric cardiac centers serving Maryland that these infants did not present for care at these institutions.
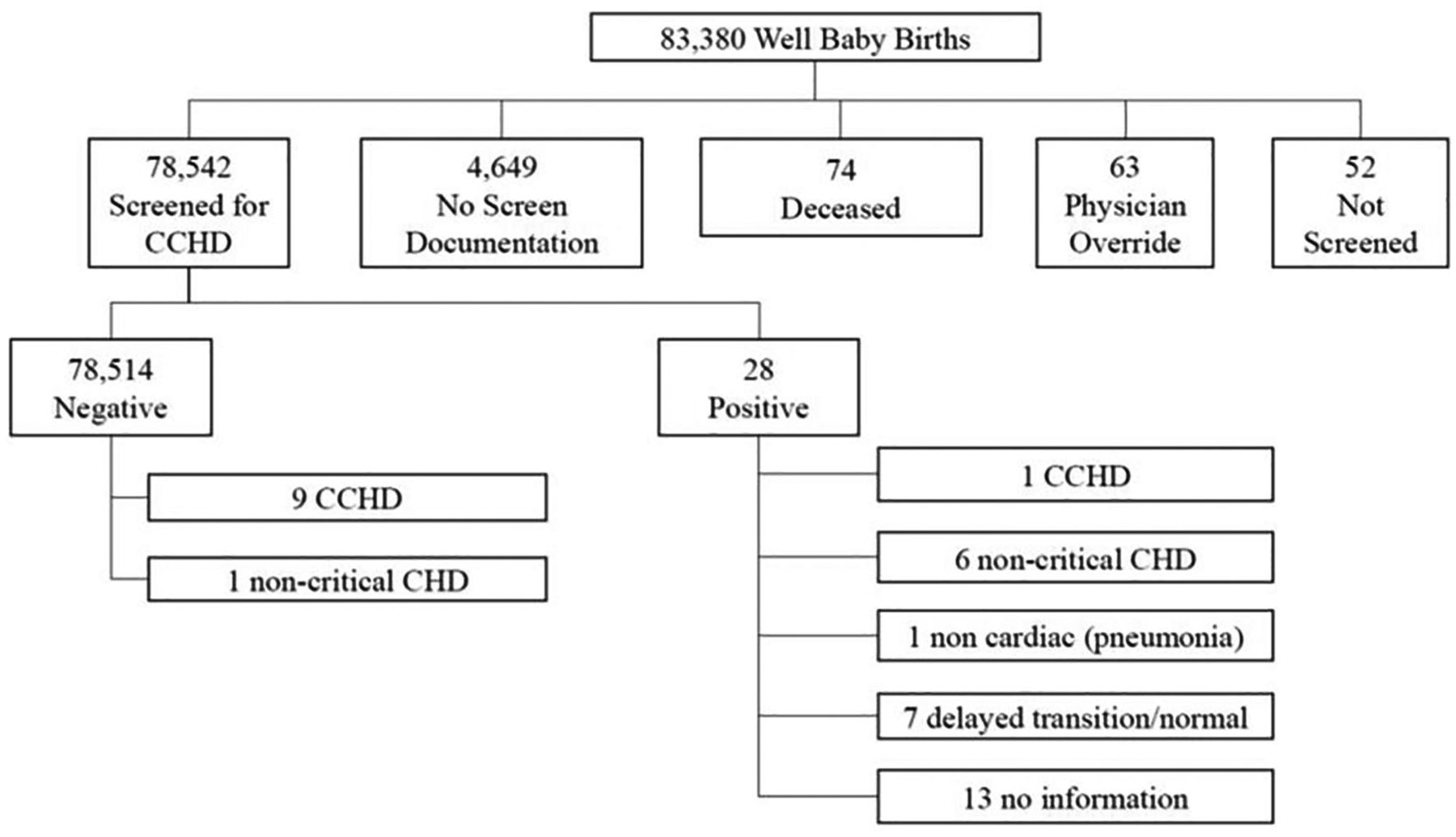
Well-baby nursery CCHD screening outcomes.
There were also 9 infants who passed their CCHD screen and were later identified with a CCHD diagnosis. Three of these infants had tetralogy of Fallot (TOF), 1 was diagnosed with total anomalous pulmonary venous return (TAPVR), and 5 had a coarctation of the aorta (COA). There was also 1 infant with a ventricular septal defect (VSD) requiring surgery. Finally, 1 infant who did not receive a screen was later diagnosed with TOF. This infant is not included in test evaluation analysis.
NICU Screening Outcomes
From September 1, 2012, to December 31, 2013, there were 9245 infants admitted to the NICU after birth, and 249 were deceased prior to screening. This left 8996 infants eligible for screening. Of these eligible infants, 6088 (67.2%) received a pulse oximetry screen. There were 569 physician overrides. Overall, 74.6% of infants were documented as having been evaluated for CCHD screening. Twenty-one infants had a positive CCHD screen. Of those infants, 3 were diagnosed with a CCHD: 1 had TAPVR and 2 had interrupted aortic arch. Three infants had non-CCHD, 14 had delayed transitions, and there was no information available on one infant.
There were also 3 infants who passed CCHD screening and later presented with a critical cardiac abnormality. One infant had TOF and 2 were diagnosed with COA. Four infants who were discharged from the NICU without a screen documented later presented with CCHD (2 with TOF and 2 with COA). These infants are excluded from test evaluation analysis. A flow chart of the outcomes of screening in the NICU is presented in Figure 2.
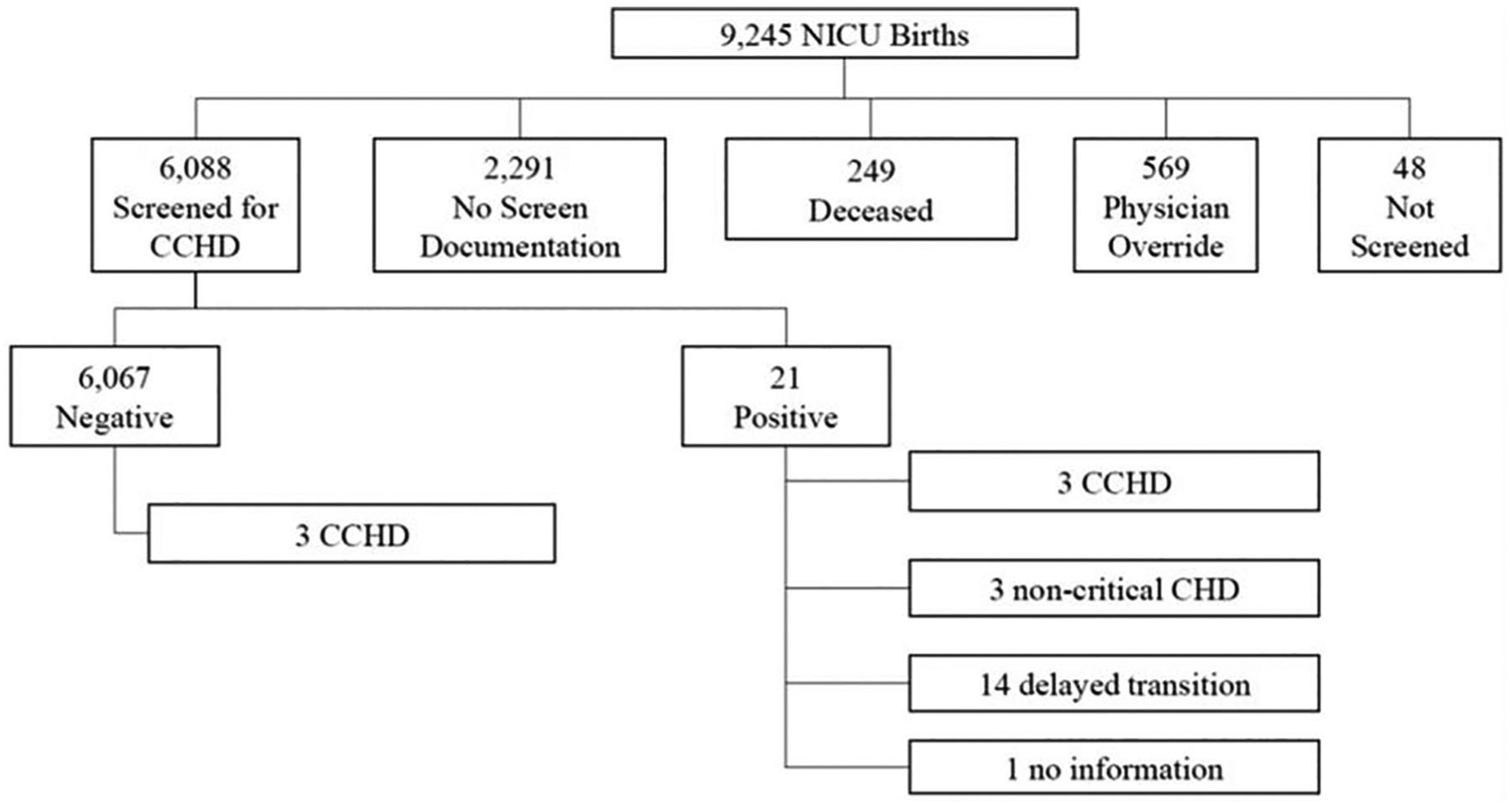
NICU CCHD screening outcomes.
Evaluation of Test
The sensitivity, specificity, and positive and negative predictive values of pulse oximetry screening for CCHD are presented in Table 2. These are presented separately for the Well-Baby Nursery and the NICU.
Well-Baby and NICU Screening for CCHD Performance Statistics.

Abbreviations: NICU, neonatal intensive care unit; CCHD, critical congenital heart disease; CI, confidence interval.
In the NICU, there were also 148 infants with clinical signs and 36 infants prenatally diagnosed with a cardiac defect. Of the infants with clinical signs, 95 had no cardiac diagnosis, 18 had CCHD (1 with hypoplastic left heart syndrome, 3 with transposition of the great arteries, 4 with TOF, 2 with truncus arteriosus, 1 with TOF and pulmonary atresia, 1 with pulmonary atresia,1 with interrupted aortic arch, 4 with COA, and 1 with double-outlet right ventricle. One infant had an A-V canal. There were 19 other non-CCHD cardiac findings and 16 infants with no outcome documented. The 36 infants with a prenatal diagnosis included 33 with CCHD, 2 with other cardiac findings, and 1 without documentation of diagnosis.
Summary
Overall, the incidence of primary or secondary target cardiac condition in this population was 7.1 diagnoses per 10 000 live births (66 infants diagnosed out of 92 628 births). Two of these infants were identified by CCHD screening, including 1 in the NICU; 12 were identified due to clinical signs; and 35 were identified prenatally. Seventeen were not identified before discharge, because they either were not screened or passed their CCHD screen.
Discussion
The results of Maryland’s first year of screening for CCHD can be compared with results of statewide mandated CCHD screening in New Jersey and Minnesota. New Jersey was the first state to begin mandatory pulse oximetry screening in newborns, and it has reported on the results of the first 9 months of screening. 8 Of 75 324 live births in licensed New Jersey birthing facilities, 73 320 were eligible for screening, of which 99% were screened. Forty-nine infants with positive CCHD screens were reported to the New Jersey Birth Defects Registry, for a positive screen rate of 0.068%, comparable with Maryland’s positive screen rate of 0.058%. Three of the 30 infants who were referred on the basis of pulse oximetry screening alone had previously unsuspected CCHDs. It should be noted that the New Jersey protocol is modified from the AAP algorithm, requiring that both the upper and lower extremities have a pulse oximetry screening of more than 95%. A pilot study in Minnesota conducted by Kochilas et al 9 reported a positive screen rate of 0.079% (6 positive screens in 7549 newborns), slightly higher than the rate in our program. In the Minnesota study, one of these infants had a CCHD diagnosis, for a false positive rate of 0.066%. Bradshaw et al 5 piloted screening in a community hospital in Maryland with 6841 eligible newborns, of whom 6745 infants (98.6%) were screened. There were 9 infants with positive pulse oximetry screens, for a positive screen rate of 0.131%. One of the 9 infants was diagnosed with CCHD, for an overall false positive rate of 0.119%.
A meta-analysis done by Tharangatinam et al in 2012 10 that included these large series as well as earlier studies, found overall sensitivity of 76.5% and specificity of 99.9%. The false positive rate when the screen was completed after 24 hours of life was 0.05%.
In 2014, Singh et al 11 published results on a series of infants admitted to a NICU due to positive CCHD screening. Of 208 infants admitted with positive screens, 79% had a significant clinical condition, which required further intervention. These included 17 with a congenital heart defect (9 of which were critical), 55 with pneumonia, 30 with sepsis, and 12 with pulmonary hypertension. The current study only identified 1 infant with a condition other than congenital heart disease that required intervention (pneumonia). It may be that infants with other conditions presented prior to screening and were listed as “physician override.” Twenty-eight echocardiograms were performed in the well-baby nursery as a result of CCHD screening. Thirteen of these infants were diagnosed with delayed transition and 1 infant with pneumonia, so it could be argued that without the CCHD screening algorithm, these 13 echocardiograms would not have been necessary. However, this is a small clinical burden compared with the total number of births, and 1 infant was identified with a CCHD lesion. Concern regarding false negative screens has been corroborated elsewhere 15, and pediatricians need to remain vigilant despite a “passed” CCHD screen if signs or symptoms of potential cardiac disease arise.
The online reporting system allows for data collection and monitoring at the individual level. Birth facilities can periodically check their compliance and outcomes of screening. At the state level, birth facilities can be compared with identify variation in performance and technical assistance needs. These data are valuable, but as the fact that more than 6% of infants do not have a screen documented in the system illustrates, incomplete information is being collected. Pulse oximetry screening results are manually entered by hospital staff, unlike newborn hearing screening, which can be entered automatically from screening equipment. The development of an interface between pulse oximetry screening equipment and the eSP system would allow for more complete and accurate data collection.
The “physician override” category has been utilized inappropriately in several cases. Often, the reason for the override is not noted. Maryland worked with OZ Systems, Inc to modify the drop-down box for screening outcomes and replace this category with the specific reason, such as prenatal diagnosis, symptoms, or echocardiogram, before screening.
One third of Maryland birth hospitals were performing pulse oximetry screening for CCHD in newborns before the mandate. Hospitals have not reported significant barriers to the actual screening, but result reporting has been noted as a burden by some facilities, particularly larger ones with more births. A telemetry module is available for direct download of pulse oximetry values from the oximeter in the online system is available to address this issue.
There has been much discussion of the use of the term “false positive,” as some infants with positive screens who do not have CCHD do have a condition requiring treatment, such as pneumonia. The current study was limited in its ability to identify other conditions, as they were frequently not reported by hospitals. This type of data collection, which is beyond the mandate of newborn screening but is critical for public health, has proven to be a challenge for all conditions identified by screening at birth. Currently, much of this information relies on personal communication within newborn screening follow-up programs and between these programs and hospitals. The development of specific electronic medical record reports for public health purposes would minimize the human error inherent in such an informal system of communication. This effort would require the cooperation of major hospital associations and dedicated resources at a national level.
The current recommendations and algorithm for CCHD screening endorsed by the AAP and AHA are based on well infants in the full-term nursery. Maryland’s regulations stipulate screening for all infants but do allow for a physician override in cases where screening is not indicated such as prenatal diagnosis. There has been some literature to address screening in NICU babies,12-14 but there is not yet a consensus to recommend that hospitals use this algorithm consistently. The heterogeneity of NICU babies makes a uniform algorithm for this population unlikely, but as more data are collected and analyzed, more informed guidelines can be developed for screening this population.
Most hospitals in Maryland are following the AAP/AHA protocol, although slight variations may exist. There have not yet been enough data collected to determine whether these variations are clinically significant, but this will be an important issue to investigate in this state and across the nation going forward.
Limitations
This study reports on data available to the newborn screening follow-up program in Maryland and is limited by hospital reporting and regulations governing that program. While hospitals are mandated to report screening results, resources are limited for individual follow-up of infants with missed or abnormal screens. In order to improve information beyond screening data, state newborn screening regulations should consider inclusion of recommendations and resources to allow for adequate follow-up.
Conclusion
This study found that in a state with relatively high prenatal detection of CCHD, pulse oximetry screening in the well-baby nursery identified only 1 infant in 15 months in the well-baby nursery, and 3 infants in the NICU. In order to improve the effectiveness of screening, barriers to obtaining data from nurseries must be overcome. While electronic data submission allows for collection of individual infant data, additional information is needed, particularly for follow-up of abnormal screens.
Further investigation of specific protocols used, interpretation of protocols, and outcomes of screening is needed for continued refinement of the well-baby algorithm, and health care providers must evaluate potential cardiac symptoms in infants despite a passing result on pulse oximetry screening. Currently, if programs are able to collect this information it is being done by personal communication, rather than standardized electronic data collection. Pulse oximetry screening in newborns provides valuable clinical information, and more complete follow-up data on an individual level are needed to improve protocols.
Footnotes
Acknowledgements
The authors would like to acknowledge the Office of Epidemiology and Research in the Maternal and Child Health Bureau, Health Resources and Services Administration, and the Altarum Institute for assistance in preparation of this manuscript. The members of the Expert Panel for CCHD Screening provided critical support in implementing this new screening program, and they are as follows: Dianna Abney, MD; Carissa Baker-Smith, MD, MS, MPH; Miriam Blitzer, PhD; Elizabeth Bradshaw, MSN, RN, CPN; Anne Eder; Tanya Green, MS, CCC-A; Carol Greene, MD; Edward Lawson, MD; Gerard Martin, MD; Cynthia Mueller, RN; Geoffrey Rosenthal, MD, PhD; Philip Spevak, MD; and S. Lee Woods, MD, PhD.
The authors would like to thank Dr Miriam Blitzer, the chair of the Maryland State Advisory Council on Hereditary and Congenital Disorders, for convening the Expert Panel and overseeing its charge. Finally, the authors greatly appreciate the assistance of OZ Systems, Inc, in modifying the eSP™ system in Maryland to include CCHD screening results.
Author Contributions
DB and JW conceptualized the analysis, and JW collected and cleaned the data; SM and LR provided the quantitative analysis of the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.