
Abstract
Blunt trauma is a major cause of death in children, with renal arterial injuries occurring in less than 1% of cases. Traumatic renal artery occlusion (RAO) in children is rare and results in the loss of ipsilateral renal perfusion. Clinical signs are often nonspecific, and there is a lack of information on the exact incidence and management outcomes of these rare cases in children. We report a case of unilateral RAO in a 13-year-old boy with polytrauma. He was diagnosed with right RAO and hepatic laceration after a fall. A conservative approach yielded favorable outcomes despite the loss of function in the right kidney. In stable polytrauma patients, prompt diagnosis of RAO is crucial for treatment optimization and potential kidney salvage.
Introduction
Renal artery occlusion (RAO) is a rare complication of blunt abdominal trauma.1,2 occurring in less than 1% of blunt renal trauma injuries and often associated with other life-threatening injuries.1-3 Children are more prone than adults to these injuries, even with less severe traumas due to their anatomical vulnerability, This can be attributed to factors such as decreased perirenal fat, weaker abdominal muscles, and a less well-ossified thoracic cage, which offers less protection to the kidneys. 4
Management guidelines for renal arterial injuries have included both pediatric and adult cases. Optimal treatment remains controversial, with options including observation, nephrectomy, surgical repair, and endovascular stenting.5,6
We present a case study illustrating a traumatic dissection and thrombosis in the right renal artery of a polytrauma patient, necessitating vigilant monitoring in the intensive care unit. Given the high risk associated with revascularization and the limited expected benefits due to the time since the occlusion, a conservative approach was chosen. Furthermore, we conducted a thorough literature review to explore the management of such rare injuries, particularly in pediatric populations.
Case Report
A 13-year-old boy presented to our emergency department in a polytrauma case with an alleged history of an accidental fall from a 3-meter-high rock. The accident occurred 5 hours before his admission. The patient, while trying to dive from a rock, landed on the sand with a craniofacial impact (acceleration/deceleration mechanism). The violence of the initial shock was not precisely known.
Clinically, the child was conscious and hemodynamically stable with an initial blood pressure of 114/56 mmHg. On inspection of his abdomen, there was no bruising on the right flank. On palpation, it was soft with mild tenderness in the right hypochondrium and the right flank, with no guarding or rigidity.
After conditioning, abdominal ultrasonography was not performed. A contrast-enhanced computed tomography (CT) body scan carried out immediately (6 hours post-trauma) revealed non-enhancement of the right kidney with a total thrombosis of the ipsilateral renal artery, localized in juxta-aortic for a length of approximately 1 cm without extravasation of the contrast product; no contrast was seen delineating the right ureter, classified as grade V of the American Association for the Surgery of Trauma (AAST). 7 A grade III hepatic laceration according to AAST classification, medium abundance hemoperitoneum, left kidney, and other viscera were reported to be normal (Figure 1).
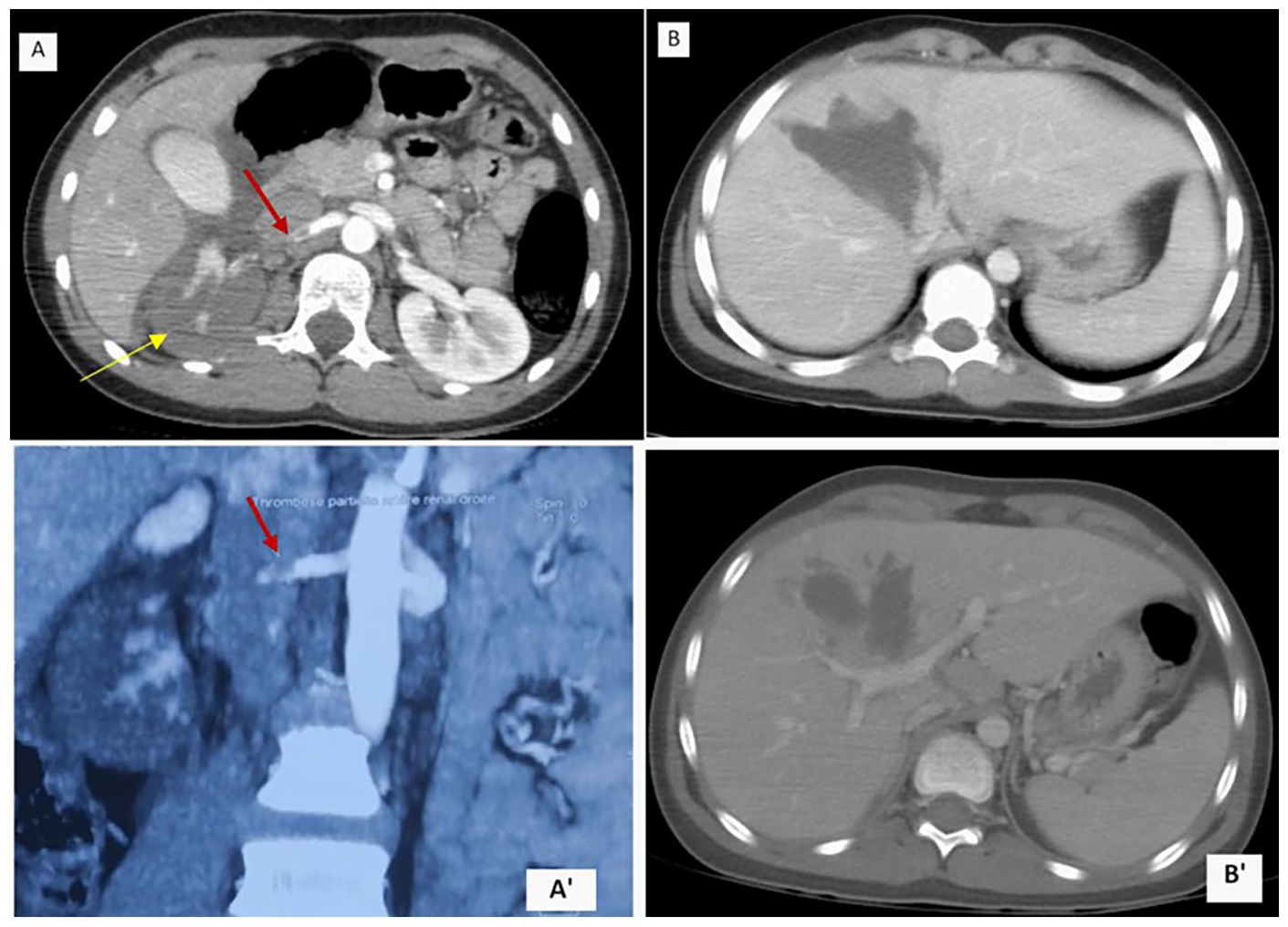
Contrast-enhanced CT scan showing (A and A′): non-enhancement of the right kidney (yellow arrow), with a total thrombosis of the ipsilateral renal artery (red arrow). (B and B′): hepatic laceration.
Initial laboratory assessments were normal, with a hemoglobin level of 12.3 g/dL, a urea level of 0.36 g/L, and a creatinine level of 0.76 mg/dL. The patient had microscopic hematuria (10 red blood cells/HBF).
Due to the delayed diagnosis, complete unilateral thrombosis, hepatic laceration with hemoperitoneum (which contraindicated anticoagulation or antiplatelet therapy after potential stent placement or endoluminal navigation), and the lack of a trained endovascular team, both endovascular and open vascular procedures were deemed ineffective and potentially harmful. Consequently, the child received conservative management with meticulous monitoring, including twice-daily blood counts to detect potential deglobalization.
After 72 hours, a follow-up CT scan showed stabilization of the lesions and reduced hemoperitoneum. Subsequently, the patient was transferred to the pediatric surgery department. During hospitalization, the patient progressed well on simple analgesics and good rehydration, leading to discharge on the 10th day with blood pressure monitoring instructions.
A repeat clinical and ultrasound Doppler examination at 2, 6, and 12 months revealed a well-differentiated, moderately hypoechoic, and hypotrophic right kidney, with the right renal artery appearing permeable on Doppler. Renal scintigraphy at 1 and 6 months indicated a non-functional right kidney with only 3% differential renal function (Figure 2).
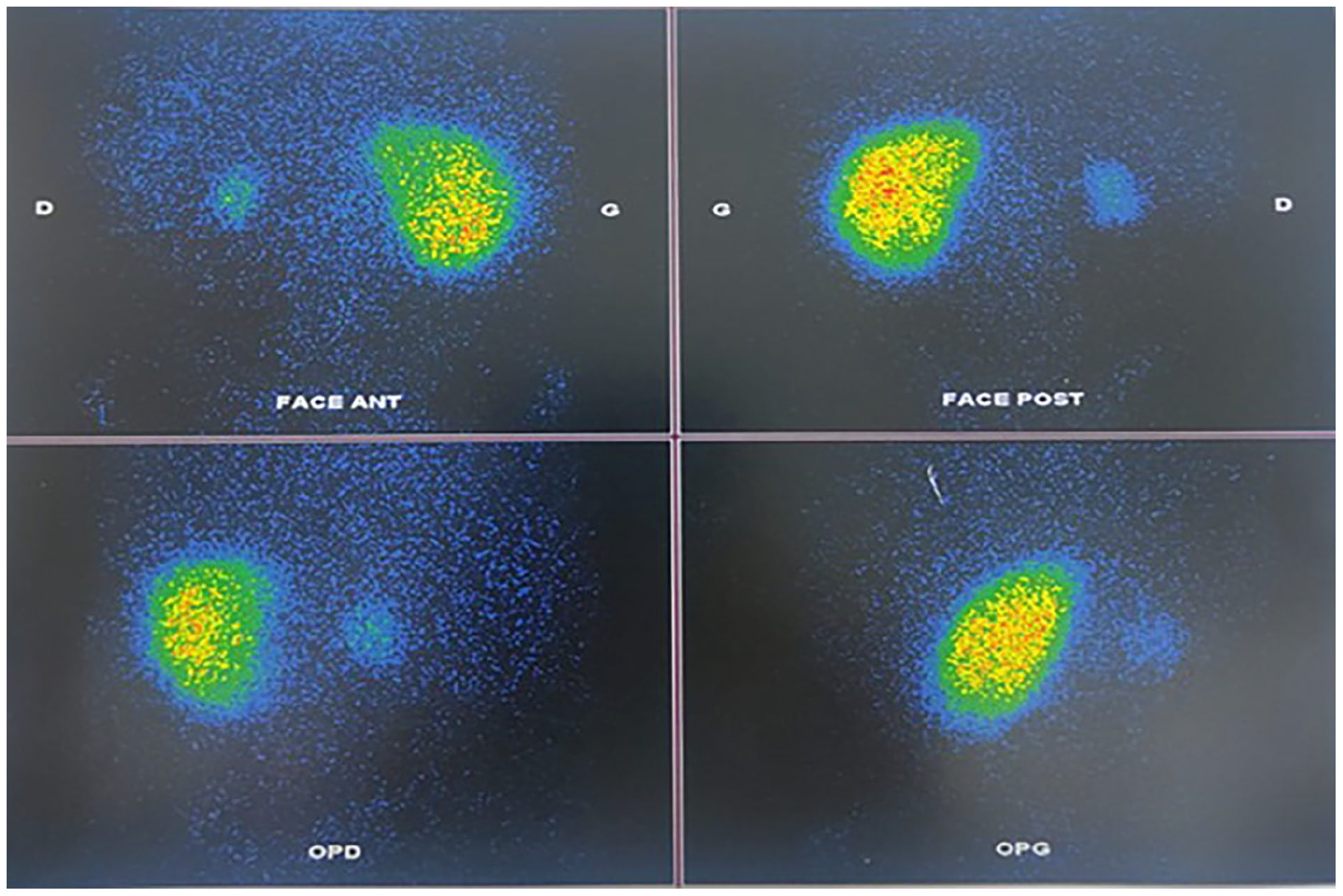
Renal scintigraphy shows only 3% of right kidney function has been preserved compared to the left kidney.
After a follow-up of 1 year, the child remains normotensive and did not develop a renal abscess despite not receiving prophylactic antibiotics. Regular follow-ups are ongoing to monitor the development of hypertension and renal abscesses.
Ethical Approval and Informed Consent
Consent Ethical approval was not required for the report of this case.
Written informed consent was obtained from the patient and their parents for the publication of this case.
Discussion
Traumatic injury of the renal arteries in children is rare and can lead to renal dysfunction and hypertension. Various studies report the incidence of renal artery injuries as 0.05, 0.08, 1%-4%.1,2,8 However, specific data on the incidence based on age are lacking. This is the first case of RAO documented in our institution.
RAO is more common in the left renal artery due to the left kidney’s greater mobility, 3 occurring more frequently in young males under 25 years of age. 1 Bilateral involvement is extremely rare.1,3,9 In our case, however, the right renal artery was dissected after a fall.
The injury mechanism often involves deceleration forces. 10 Deceleration force can lead to traction on the fixed renal vascular pedicle, causing intimal tearing, which can result in dissection, secondary thrombosis, and ischemia. Compression of the renal artery between abdominal contents and vertebral bodies, leading to intimal damage, has also been implicated.5,11,12 The more likely mechanism of intima tearing of the renal artery was a sudden deceleration in our case.
Renovascular injuries usually occur on the proximal portion of the renal arteries (the first 2 cm). 13 In our case the main renal artery was involved at the juxta-aortic for a length of approximately 1 cm.
Traumatic renal arterial thrombosis is uncommon as a standalone injury and usually suggests significant associated trauma. 2 In cases of polytrauma, close monitoring of vital signs may occasionally result in overlooking a diagnosis of renal artery dissection. 12 Symptoms like flank pain and hematuria should prompt consideration of renal artery dissection, emphasizing the importance of early diagnosis, especially in stable patients.1,2,12
In our case, the patient presented with vague abdominal pain and mild tenderness in the right hypochondrium and flank, with later identification of microscopic hematuria. More than the clinical signs themselves, understanding the context of initial trauma occurred (exact nature, kinetics) served as a warning sign, prompting intensive care monitoring and the realization of a CT scan.
Doppler ultrasonography of the renal arteries, contrast-enhanced CT, and renal scintigraphy are effective for the diagnosis and follow-up of renal artery dissection. 12 Contrast-enhanced CT scanning is the preferred method for diagnosing renal artery injury,2,10 with findings suggestive of renal arterial thrombosis including the absence of renal parenchymal enhancement and contrast excretion in the affected kidney. 11 CT scans can also assess associated injuries, supplanting the need for arteriography except when therapeutic endovascular procedures are considered.14,15
Optimal treatment for traumatic RAO remains controversial due to its rarity, delayed diagnoses, the presence of other life-threatening injuries, and the disappointing long-term results of revascularization procedures.1,2,16 Early restoration of blood flow is crucial for preserving renal function, as warm ischemia time is short and the injury can become irreversible. The suggested time window for successful revascularization is less than 4 hours of warm ischemia.2,11,15,17
Haas and Spirnak 5 analyzed 159 cases, Of the 20 patients with bilateral renal artery occlusion, surgical revascularization was attempted in 16 and successful in 9 (56%). Of the 139 patients with unilateral renal artery occlusion, surgical revascularization was attempted in 34 and successful in 9 (26%). Evidence of decreased renal function was noted in 67% of those who had successful revascularization for unilateral injury at a mean follow-up of 1.8 years. Jawas and Abu-Zidan 2 proposed an algorithm for treating RAO in adults (Figure 3). Suggesting revascularization in ideal patients with very short warm ischemia times (less than 2 hours) without major associated injuries or prolonged hypotension and aggressive revascularization for bilateral and solitary kidney RAO, as early as possible or even regardless of time delay. 2 This algorithm is also applicable to children. Additionally, Zhong et al 18 reported a cohort of 4 pediatric traumatic unilateral RAO cases managed conservatively without complications (Table 1).

Suggested algorithm for complete renal artery occlusion in multiple trauma patients. 2
Pediatric Traumatic Renal Artery Thrombosis Case Summaries.

Abbreviations: M, male; F, female; ATV, all-terrain vehicle.
Endovascular intervention, though an attractive option for treating RAO in adults, 11 lacks sufficient experience and evidence in pediatric patients. To our knowledge, 2 pediatric cases have been reported to undergo endovascular treatment for renal arterial injuries (Table 1). Vidal et al 19 reported the first case of a 15-year-old boy with post-traumatic RAO successfully with endovascular therapy, with long-term scintigraphic follow-up. Hsu et al 20 reported the case of a 2-year-old girl who developed post-traumatic occlusion from an intimal flap in a renal artery, which was treated with stent placement. Although the stent successfully restored renal artery flow, the patient developed stenosis within the stent and ultimately required a nephrectomy several months later. It has been suggested that endovascular revascularization be considered for ideal patients with very short warm ischemia. However, these studies lack large sample sizes and long-term results. 15 Our case ruled out an endovascular procedure due to delayed diagnosis, unilateral character, and associated injuries, leading us to opt for conservative management.
The follow-up of these patients is crucial, including scintigraphy scans to delineate the kidney function and development of hypertension. About 32% of conservatively managed patients develop hypertension within the first year, compared to 12% in those operated on. 5 These patients may need delayed nephrectomy. Our patients did not develop any infection or hypertension; only 3% of the right renal function was preserved.
The paucity of age-based literature makes it difficult to optimally answer this issue and highlights the need for studies in larger series. Close, regular follow-up is required to assess blood pressure and renal function. Long-term implications of living with a single kidney include risks of hypertension, reduced kidney function, and chronic kidney disease.
Conclusion
Traumatic RAO in children is rare and underreported, leading to the application of the same treatment algorithm as in adults due to a lack of age-based comparisons in larger series. The standard treatment for RAO associated with polytrauma in children has not been established. Surgical revascularization has limited indications, while endovascular revascularization is an alternative with encouraging short-term results. Optimal treatment should be determined after a comprehensive assessment of the prognosis.
Footnotes
Author Contributions
All authors contributed to the writing of this manuscript, all read and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The patient and their parents written approval was obtained for the publication of this article.