
Abstract
Thoracic blunt injuries are not uncommon, and they can cause severe cardiac and major vascular damage, leading to high mortality. Blunt cardiac rupture and traumatic aortic dissection are the primary fatal outcomes of these injuries. Many patients do not survive long enough to reach the hospital, and even those who present to emergency departments face challenges in timely diagnosis and management. This narrative review was conducted in accordance with the core principles of the Scale for the Assessment of Narrative Review Articles. A literature search was performed to summarize current evidence on blunt cardiac rupture and traumatic aortic dissection in thoracic blunt trauma settings. Early recognition of life-threatening complications from thoracic blunt trauma is essential for prompt and accurate diagnosis as well as appropriate clinical interventions. Cardiac rupture and traumatic aortic dissection from thoracic blunt trauma have traditionally been considered distinct entities, exhibiting different injury mechanisms and clinical outcomes. This review provides a comprehensive overview of the etiology, injury mechanisms, diagnosis, and management of fatal cardiac rupture and aortic dissection resulting from thoracic blunt trauma. The review is limited by the scarcity of high-quality studies and the predominance of case reports, but it highlights critical patterns in diagnosis and management that may inform clinical practice and guide future research. Overall, the findings underscore that improved understanding and awareness of these conditions can facilitate earlier diagnosis and treatment, ultimately reducing mortality and improving patient care in real-world clinical settings.
Keywords
Introduction
Fatal cardiac and major vascular injuries from thoracic blunt trauma primarily include blunt cardiac rupture (BCR) and traumatic aortic dissection (TAD). Blunt chest trauma can result in a spectrum of cardiovascular injuries, ranging from mild myocardial contusion to life-threatening conditions, such as cardiac rupture or TAD, which arise from direct damage to the heart muscle or disruption of the aortic wall. 1 These catastrophic outcomes occur in approximately 0.007%–0.45% of admitted patients.2,3 Their rarity and nonspecific clinical signs lead to considerable diagnostic difficulties and are associated with high mortality. Clinical signs in thoracic trauma patients vary widely, ranging from vague symptoms, such as chest and back pain, to severe presentations, including coma, which significantly complicate early recognition and timely management. 4 Moreover, fatal cardiac and major vascular injuries may arise from both high-energy and seemingly minor thoracic trauma, making clinical suspicion crucial for prompt diagnosis.
Although previous studies have reported individual cases, comprehensive analyses distinguishing the clinical characteristics, risk factors, and outcomes of BCR and TAD remain limited. To the best of our knowledge, existing literature on these conditions is limited, mainly consisting of case reports and case series, with only a few studies offering guidance for early identification and intervention strategies. In this review, we have categorized thoracic blunt trauma, which leads to fatal cardiac and major vascular injuries, into two entities: BCR and TAD. We have also provided illustrative figures to facilitate the understanding of these life-threatening conditions. Emergency medical personnel should recognize that cardiac rupture or aortic dissection may occur following seemingly minor blunt chest trauma, enabling prompt intervention to improve patient outcomes. By summarizing current evidence and highlighting clinical patterns, this review aimed to increase awareness among clinicians and guide future research directions. This narrative review was conducted in accordance with the core principles of the Scale for the Assessment of Narrative Review Articles (SANRA), including a clear statement of scope, literature search transparency, and discussion of clinical relevance and limitations. 5
Literature search
Using the keywords “Lenz-Majewski syndrome” OR “PTDSS1,” we conducted a literature search in PubMed, Scopus, and Web of Science. Of the 218 retrieved records, 150 remained after duplicates were removed. Screening of titles and abstracts excluded 100 articles, leaving 50 full-text articles for eligibility evaluation. A total of 9 studies were excluded (irrelevant: 5; incomplete data/type mismatch: 4), resulting in 41 included studies. The selection process is summarized in Figure 1, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework. The literature search and selection process followed SANRA principles, ensuring transparency, reproducibility, and comprehensive coverage of relevant studies.

PRISMA flow diagram showing the process of study identification, screening, eligibility assessment, and final inclusion for the systematic review. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Clinical overview of major thoracic trauma: mechanisms, epidemiology, and management
Etiology and injury mechanism of BCR
BCR refers to a complete laceration of the heart muscle resulting from blunt chest trauma. 6 Motor vehicle collisions are the leading cause of BCR, especially in high-speed accidents.3,7 BCR may also result from indirect impacts during sports, such as sudden deceleration injuries, heart compression between the sternum and vertebral column, or increased venous pressure from the abdomen or legs.7–9 Additionally, blunt trauma can cause rib or sternum fractures, which may directly injure the heart. 10
BCR is believed to occur due to abrupt elevations in intracardiac pressure during rapid thoracic compression or a surge in venous return triggered by abdominal compression of the inferior vena cava. Such injuries are often instantly fatal, as the heart may protrude from the pericardium, causing torsion of the major blood vessels. 3 The reported incidence of BCR among trauma-related hospital admissions ranges from approximately 0.16% to 2%. 11 However, the actual incidence may be higher, as many victims do not survive long enough to reach a hospital. Among patients who survive to reach the hospital, 44% die shortly after admission or in the emergency department, and 45% of initially surviving patients eventually die during hospitalization. 3 Another study revealed that 91% of BCR patients died within 30 minutes of injury. 12
The location of cardiac rupture often depends on the cardiac cycle at the time of injury.7–9 Among reported cases, the right atrium is the most commonly affected (40.6%), followed by the right ventricle (31%), left atrium (25%), and left ventricle (12%).7,11–13 Anatomical studies suggest that the right atrial appendage, thinner than the atrial wall, may be particularly vulnerable to rupture. 9 Clinically, BCR often presents with cardiac tamponade, hemopericardium, or pneumopericardium.10,11,14 In some cases, an associated pericardial tear can lead to significant hemothorax. 10 Notably, patients who undergo surgical repair may still die days later due to necrosis and delayed rupture of the injured ventricular tissue. 15
Diagnosis of BCR
BCR is associated with a high mortality rate of 50% to 100%, necessitating rapid and accurate diagnosis.7,16 Unlike penetrating cardiac injuries, which often present with obvious entry wounds, BCR frequently remains occult, particularly in patients involved in high-velocity traffic collisions, the leading cause of this injury. Common clinical signs of BCR include the triad of hypotension, muffled heart sounds, and jugular venous distension, indicative of cardiac tamponade. However, these signs may be subtle or absent due to hypovolemia at presentation or coexisting severe hemorrhagic injuries that mask tamponade signs.3,7,14
Electrocardiograms and cardiac biomarkers are generally considered more reliable for excluding cardiac injury than for confirming it in acute trauma cases.7,17–19 When BCR is suspected, prompt imaging is essential. Recommended modalities include chest computed tomography (CT), focused assessment with sonography for trauma (FAST), and transthoracic echocardiography (TTE), which are central to both diagnosing BCR and guiding emergent management.7,10,17,20
CT scans can demonstrate sternal or rib fractures indicative of significant thoracic trauma, along with hemopericardium and pneumopericardium, which strongly suggest cardiac rupture (Figure 2(a) and (b)). The severity of cardiac tamponade depends on the pericardial tear size and hemorrhage rate. 10 Active contrast extravasation may further indicate pericardial breach, and CT can also reveal associated mediastinal and cervical injuries (Figure 2(c) and (d)).

CT imaging of thoracic blunt trauma leading to BCR and TAD. (a–d) Features of BCR. (a) Rib fractures indicative of severe chest impact. (b) Hemopericardium and pneumopericardium suggestive of cardiac rupture. (c) Mediastinal free air indicating mediastinal injury. (d) Subclavian free air suggestive of injury to the pulmonary apex or cervical region. (e, f) Associated multiple organ injuries in BCR. (e) Liver contusion. (f) Kidney contusion. (g–l) Features of TAD. (g) Axial reconstruction in bone window showing rib and sternal fractures. (h, i) Thoracic aortic dissections with mediastinal hematoma. (j) Mediastinal widening with blurred aortic borders and hemothorax. (k, l) Axial reconstruction in soft tissue window showing sickle-shaped contrast encircling the aorta. BCR: blunt cardiac rupture; CT: computed tomography; TAD: traumatic aortic dissection.
FAST and TTE are essential for early detection and management of tamponade, particularly in trauma resuscitation settings. Pericardial catheterization under ultrasonographic guidance may aid diagnosis, as the color and volume of aspirated blood can indicate the rupture site. 16 Chest radiographs may occasionally reveal a widened mediastinum or enlarged cardiac silhouette, but are often nondiagnostic in BCR. Comprehensive assessment should also include evaluation for concomitant injuries to organs, such as the lungs, liver, spleen, and kidneys (Figure 2(e) and (f)), which are frequently involved in high-impact trauma.
Treatment of BCR
On the arrival of a BCR patient in the emergency room, initial management should include assessment of vital signs, peripheral perfusion, open wounds, signs of cardiac tamponade, pericardial tear, and severe bleeding injuries. Patients with unstable vitals require immediate interventions, such as intubation, fluid resuscitation, transfusion, and intravenous analgesics. When cardiac tamponade is suspected, ultrasound-guided pericardiocentesis may serve as both a diagnostic and temporary therapeutic measure. Immediate operative management is recommended for patients with cardiac tamponade, as the time needed for surgical preparation is comparable to catheter insertion. 11
Emergency thoracotomy remains the definitive treatment, enabling rapid decompression of pericardial pressure and restoration of hemodynamic stability.10,15 The choice of surgical incision depends on the patient’s condition and exposure requirements. The preferred approach is a subxiphoid pericardial window, followed by median sternotomy, offering optimal visualization of all cardiac chambers and major vessels, enabling cardiopulmonary bypass, and permitting extension to a laparotomy if clinically necessary.7,15,16 Conversely, a left anterolateral thoracotomy offers rapid access but limited visibility of cardiac structures, except for the left ventricular apex. 10 A low alternative incision at the site of sternal fracture is another option, offering direct exposure of the injured right ventricular outflow tract, although overall cardiac visibility remains limited. 10
Thoracotomy carries substantial risks, as massive bleeding or extensive manipulation may cause sudden circulatory collapse. Knowledge of the anatomical course of the internal thoracic vessels facilitates rapid hemostasis. 14 Emergency thoracotomy aims to achieve multiple objectives, including relieving cardiac tamponade, controlling bleeding, facilitating internal cardiac massage, isolating upper torso circulation via descending aorta clamping during damage-control surgery, and allowing rapid large-volume intracardiac fluid resuscitation. 2 Despite prompt interventions, patients with BCR exhibit high mortality both during hospitalization and after discharge. Studies indicate that elevated creatinine and CK-MB levels, thrombocytopenia, and multiorgan traumatic injuries are associated with poor prognosis.11,15 These findings underscore the critical importance of early recognition, rapid resuscitation, and timely surgical management to improve outcomes in patients with BCR.
Urban thoracic trauma
Urban thoracic trauma is increasingly prevalent owing to high population density, heavy vehicular traffic, and intensive industrial activity. Compared with rural trauma, urban cases are more frequently associated with high-energy mechanisms, such as high-speed motor vehicle collisions, falls from height, assaults, and industrial accidents, frequently presenting as polytrauma with both blunt and penetrating injuries. 21
Epidemiologically, most cases occur in young adult males, with pedestrians and motorcyclists representing particularly vulnerable subgroups.22,23 The injury mechanism largely determines clinical presentation: blunt trauma typically causes rib fractures, pulmonary contusions, and hemothorax, whereas penetrating trauma more often results in pneumothorax, hemothorax, or direct cardiac injury. 21 Early recognition, rapid triage, and timely intervention are critical, as many thoracic injuries in urban settings are acutely time-sensitive and potentially life-threatening. Initial evaluation should include chest X-ray, FAST, and CT scanning, enabling rapid identification of life-threatening conditions. Management often requires urgent surgical or endovascular intervention, supported by coordinated care in high-volume trauma centers. Prehospital measures, such as prompt on-scene stabilization and rapid transport, are decisive for survival, emphasizing the importance of robust urban emergency medical service systems. 24
For noncardiac thoracic injuries, which are particularly common in urban trauma, timely recognition of pneumothorax, hemothorax, pulmonary contusions, and rib fractures is essential. Immediate interventions may involve tube thoracostomy, surgical drainage, or supportive respiratory care. Standardized assessment algorithms that integrate rapid imaging, clinical examination, and structured triage can substantially improve patient outcomes and reduce complications. 21 Recognizing urban-specific injury patterns improves clinical decision-making, particularly in the context of high-risk conditions such as BCR and TAD. Awareness of high-risk populations, predominant injury mechanisms, and typical thoracic injury patterns enables clinicians to prioritize diagnostic evaluations, anticipate complications, and tailor interventions. 21 Integration of these insights with rapid imaging, early triage, and coordinated multidisciplinary management can facilitate timely detection and intervention for both cardiac and noncardiac thoracic injuries, ultimately improving patient outcomes in urban trauma settings.
Clinical overview of TAD: mechanisms, diagnosis, and management
Etiology and injury mechanism of TAD
TAD is a potentially fatal condition most often associated with vehicle crashes and falls from heights.25–28 It represents the second leading cause of traumatic fatalities. 26 In trauma patients, aortic injuries occur at an annual incidence of approximately 22 cases per 100,000 individuals. 29 Although relatively uncommon, TAD accounts for approximately 1.79% of clinical cases involving blunt chest trauma. 30 A striking 85% of TAD patients die before reaching the hospital, and more than half of the survivors die within 24 h of admission. 31 Consequently, clinical experience in managing such cases is limited, posing challenges in developing standardized treatment protocols.
TAD usually arises from high-energy blunt impact conditions, where rapid deceleration or compression generates extreme shear stress on the aortic wall. 28 This mechanical stress may directly rupture the aorta or produce an internal tear, most often at the inner curvature of the distal aortic arch near the left subclavian artery. The injury results from a combination of external shear forces, torsional stress, and abrupt intravascular pressure surges caused by events such as high-speed vehicular collisions, vertical falls, industrial accidents, or severe thoracoabdominal compression. 25
The entry tear in TAD predominantly occurs at the aortic isthmus, reported in 45% to 67% of cases, as more than 54.0% to 91.4% of blunt traumatic aortic injuries (BTAI) involve this region.28,32,33 Anatomical fixation explains this tendency: the aortic isthmus, located between the flexible ascending aorta and the fixed descending thoracic aorta anchored by the ligamentum arteriosum, is highly vulnerable to differential motion in high-velocity deceleration events. The next most frequently affected segments are the ascending aorta, aortic arch, distal descending aorta, and abdominal aorta. 34 One study reported that nearly 93% of proximal intimal tears originated at the aortic isthmus, particularly along the inner curvature. Furthermore, proximal intimal tear sizes on the outer curvature are typically larger than those on the inner curvature. 4 In TAD, blood enters the aortic media through the injured intimal tear, separating the media and forming a hematoma. Progression of the dissection may result in pseudoaneurysm formation, complete rupture, or progressive aortic dilation. The rate of bleeding progression varies widely, depending on the extent of the initial injury, hemodynamic stability, and the presence of concomitant trauma.27,35
Diagnosis of TAD
TAD is an uncommon manifestation of BTAI, associated with a poor prognosis, diverse clinical manifestations, and a high likelihood of concomitant injuries. 4 A study involving 24,010 BTAI patients revealed that most presented with chest injuries, with rib fractures and pulmonary contusions being the most common. 36 Between 76% and 96% of TAD patients present with severe chest and back pains described as tearing or lacerating. 31 However, these symptoms may be misleading because they can also result from associated rib fractures, abdominal trauma, spinal injuries, or pulmonary contusions. 37
Chest trauma accompanied by hemothorax, particularly on the left side, should prompt suspicion for TAD, even in the absence of haemopneumothorax. 25 Failure to promptly recognize TAD can result in missed resuscitation opportunities and increased mortality. For example, in one of our cases, an extensive multivessel aortic dissection was initially overlooked, leading to delayed treatment. Indeed, TAD has a missed diagnosis rate of up to 60%. 31
Contrast-enhanced CT remains the preferred first-line imaging modality for suspected TAD (Figure 2(g) to (i)). Compared with standard angiography, CT can identify intraluminal thrombus, differentiate true and false lumens, and evaluate mass effect from local hematoma on adjacent structures. Plain CT scans may reveal indirect signs such as mediastinal widening with indistinct aortic borders (Figure 2(j)) or a large hemothorax, whereas subtle findings—such as intimal displacement or sickle-shaped calcification surrounding the aorta—should also raise suspicion (Figure 2(k) and (l)).
Nevertheless, CT has limitations. One study reported a 17% false-negative rate and a 39% false-positive rate in diagnosing aortic injury using CT, and other large series advise against its indiscriminate use as the sole diagnostic tool.38–40 Computed tomography angiography (CTA) demonstrates a sensitivity of 94% and a specificity of 100% for aortic dissection diagnosis, with typical findings such as an intimal flap separating the aorta into true and false lumens, double lumen formation, and involvement of branch vessels (e.g. brachiocephalic trunk, carotid, subclavian, mesenteric, renal, or iliac arteries).25,41,42
Transesophageal echocardiography (TEE) serves as a valuable adjunct to CTA, enabling bedside assessment of proximal ascending and descending aortic lesions, detection of aortic regurgitation, and evaluation of cardiac function. 43 Unlike aortography, TEE is noninvasive, requires no contrast, and can be performed in 15–20 minutes in the emergency room. However, its sensitivity is limited in the ascending aorta and aortic arch because of the air-filled structures and complex branching anatomy. A prospective study of 29 blunt chest trauma cases reported a TEE showing a sensitivity of 57% and a specificity of 91%. 44 Importantly, no single imaging modality offers a definitive diagnosis in all cases. Therefore, a multimodal approach that integrates clinical assessment, CTA, and, where appropriate, TEE remains essential. Additionally, elevated D-dimer, C-reactive protein, and neutrophil-to-lymphocyte ratio levels are frequently observed in TAD and may serve as supportive markers.4,45–47 Early detection is facilitated by a high degree of clinical suspicion, notably in cases involving high-risk injury mechanisms and suggestive radiologic or laboratory evidence.
Treatment of TAD
Immediate management of trauma patients with multiple injuries presents complex, time-critical challenges. In TAD, the coexistence of life-threatening aortic injury with concomitant trauma necessitates individualized treatment strategies and close coordination within multidisciplinary teams. Particularly in cases of severe polytrauma resulting from traffic accidents or high-energy falls, effective resuscitation is often difficult. At the outset, the nursing team should closely monitor vital signs, administer oxygen, provide blood transfusions, and establish intravenous access. Early and adequate analgesia, with sedation, if necessary, is essential not only to alleviate pain and anxiety but also to minimize sympathetic activation that may exacerbate aortic wall stress. In cases of hemorrhagic shock, judicious fluid resuscitation is required to restore circulating volume while avoiding over-resuscitation, which may worsen bleeding or dissection. Strict blood pressure and heart rate control is critical to prevent aortic rupture or progression of dissection, typically achieved with short-acting beta-blockers and vasodilators to maintain systolic blood pressure within a controlled range (e.g. 100–120 mmHg), thereby reducing shear stress on the aortic wall. Following damage-control strategies for severely injured patients, urgent measures such as external pelvic fixation, limb fracture traction, vessel embolization, or enterostomy may be indicated. In the context of TAD, the sequence of interventions must be carefully planned because excessive surgical stress or uncontrolled hemodynamic fluctuations during nonaortic procedures can precipitate dissection progression or rupture. It is essential to minimize iatrogenic stress from extracorporeal circulation and open thoracoabdominal procedures.
Open repair remains a treatment option for patients with TAD, but it carries a reported mortality rate of approximately 20%.48,49 Endovascular repair has become the preferred approach, showing favorable short- and intermediate-term outcomes in elective and emergency settings. 50 Compared with open surgery, endovascular aortic repair (EVAR) is associated with lower perioperative mortality and improved overall outcomes.4,26 In selected unstable patients, EVAR may be performed under regional or local anesthesia, reducing procedural risk. Comprehensive postoperative intensive care is imperative, with strict blood pressure management, early detection of complications (e.g. endoleaks or stent migration), and scheduled follow-up imaging to ensure long-term durability of repair.
Discussion
This narrative review was prepared with reference to the core principles of the SANRA, emphasizing transparent literature selection, evidence synthesis, and discussion of limitations. 5 This review synthesized global evidence on BCR and TAD, highlighting similarities, differences, clinical implications, and knowledge gaps across studies. Although distinct in pathophysiology and clinical presentation, both BCR and TAD share similar diagnostic and therapeutic challenges in the setting of severe thoracic blunt trauma. As highlighted in our comparative table (Table 1), this synthesis integrates findings from multiple studies to underscore patterns in early recognition, diagnostic pitfalls, and management strategies. Early recognition is often hindered by nonspecific clinical manifestations, overlap with other thoracic or systemic injuries, and complex polytrauma presentations. Imaging remains central to definitive diagnosis; however, the selection of modalities must be tailored to hemodynamic stability and coexisting injuries. In terms of management, BCR typically necessitates immediate surgical repair, whereas TAD can be managed with either open or endovascular approaches, depending on lesion location and the patient’s condition. Despite these differences, both conditions require rapid hemodynamic stabilization, coordinated multidisciplinary management, and vigilant postoperative surveillance. A comparison across the reviewed literature reveals consistent challenges, as well as gaps in early diagnostic protocols and consensus on treatment approaches, emphasizing the need for standardized guidelines.
Key clinical features and differences between BCR and TAD.
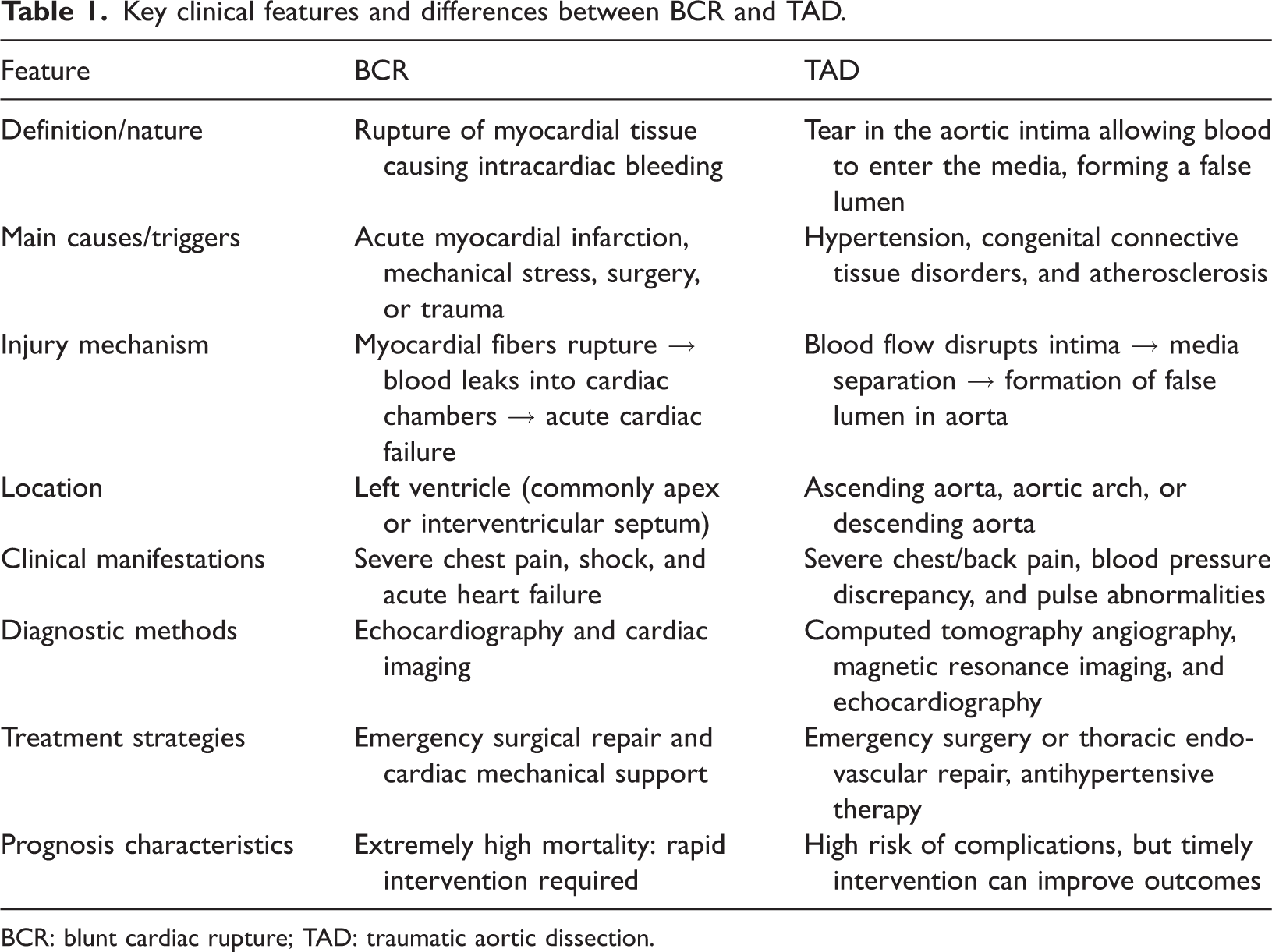
BCR: blunt cardiac rupture; TAD: traumatic aortic dissection.
Thoracic blunt trauma causing fatal cardiac and major vascular injuries is relatively uncommon but highly lethal. Among these, BCR and TAD represent the two most critical entities with exceptionally high mortality rates. Because initial presentations are often subtle, early suspicion, timely diagnosis, and prompt intervention are critical for survival. In patients with severe thoracic blunt trauma, such as those resulting from motor vehicle collisions, high-level falls, or chest compression, in which BCR and TAD cannot be excluded, definitive diagnosis should be guided by the mechanism of injury, clinical indicators, and timely imaging. This requires a high index of suspicion, early deployment of appropriate imaging modalities, and seamless collaboration between emergency medicine, cardiothoracic surgery, vascular surgery, and critical care teams. By providing a global overview of available evidence, this review underscores the importance of a structured diagnostic and therapeutic algorithm that encompasses rapid assessment, hemodynamic stabilization, tailored surgical or endovascular repair, and meticulous postoperative care. Such a systematic and continuous approach is pivotal for the effective management of these high-risk patients and may serve as a valuable reference for future clinical decision-making in similar trauma scenarios. Nevertheless, the review is limited by the scarcity of high-quality studies, heterogeneity in case reporting, and the predominance of case reports and series, which restricts the generalizability of findings. This limitation highlights the need for cautious interpretation and further high-quality research.
Conclusion
In summary, BCR and TAD are critical complications of thoracic blunt trauma with extremely high mortality. Early recognition, timely intervention, and multidisciplinary coordination are essential for improving patient outcomes. This review synthesizes current evidence, emphasizing clinical patterns, diagnostic challenges, and management strategies, and underscores the importance of early recognition and coordinated care in severe thoracic blunt trauma.
Footnotes
Acknowledgments
The authors acknowledge the use of ChatGPT (OpenAI) for language polishing of the manuscript.
Author contributions
L.W. drafted the manuscript. H.Y. conceived and designed the study, oversaw data collection, and interpreted the figures. S.S. and L.L. provided the data and figures and contributed to figure legend interpretation. All authors reviewed and approved the final manuscript and take responsibility for all aspects of the work.
Consent to participate
Not applicable.
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no competing interests.
Ethics statement
Written informed consent was obtained from the patient for publication of the case details. Institutional approval was also secured to permit publication. The authors take full responsibility for all aspects of the work, ensuring that any questions regarding the accuracy or integrity of the study are thoroughly addressed and resolved.
Funding
This work was supported by the 1·3·5 Project of Center for High Altitude Medicine, West China Hospital, Sichuan University (grant number: GYYX24017, Haifang Yu, corresponding author). This funding was used for PRISMA diagram preparation and publication fees.