
Abstract
Aim. To analyze the relationship between auditory risk factors at birth and subsequent language development in toddlerhood. Methods. Participants are 136 children from a longitudinal birth cohort follow-up at age 2 years. They were divided into 2 groups: One comprising 105 children without hearing risk factors at birth and another comprising 31 children with auditory risk factors at birth but normal hearing. Results. In children with and without risk factors, the combination of socio-emotional, socio-economic, and auditory risk factors at birth significantly predicted language development at age 2 years. Family socio-economic status had a significant impact on overall child development, even after controlling for socio-emotional development and the presence of risk factors. Conclusions. The study was conducted in an upper-middle income country with a socialized health care system. It underscores the importance of a holistic approach to early childhood language development, taking into account biological, socioeconomic, and emotional factors.
The first 1000 days of life are critical for child development in all measurable domains and play an important role in lifelong academic progress. 1 In addition, early interventions have significant potential to improve developmental and educational outcomes in the first 3 years of life.1-3 This period of development remains critical to support language development as represents a key indicator of later health and academic outcomes. 4
Speech and language development during this early period can have a long-term impact early and subsequent childhood years. Early literacy and math skills, emotional intelligence, and school readiness are closely linked to language and have an impact on later academic achievement in school and adolescence.5-11 It is therefore important to identify auditory risk factors at birth and to intervene early.
An expert panel of the Joint Committee on Infant Hearing (JCIH) has identified several auditory risk factors that can negatively impact language development. 12 These include family history of hearing loss, gestational infections, cranio-facial anomalies, low birth weight, severe hyperbilirubinemia, ototoxic medications, bacterial meningitis, low APGAR score, prolonged mechanical ventilation, and syndromic causes. Such factors affect not only the child’s hearing and speech, but also physical, cognitive, and socioemotional development.13,14
Several studies have shown that the risk factors for hearing disorders identified by the JCIH can have a detrimental effect on children’s cognitive development.15-17 This research underscores the lasting influence of risk factors at birth on early educational outcomes. However, family influence during the first 6 years of a child’s life can help mitigate such effects. A recent comprehensive review by Patronick et al 18 recognized the critical role of the family in the care of preterm infants. They concluded that behavioral problems in preterm or low-birth-weight infants could be modified between 2 and 4 years of age by interventions targeting parental behavior.
The active involvement of families is crucial for promoting language development. Parental income and local economic conditions are closely linked to birth risk factors.19-21 In many cases, birth risk factors are associated with lack of prenatal care, malnutrition, maternal stress and tobacco use during pregnancy. Therefore, family income and socioeconomic conditions play a key role in the healthy growth and development of children in the first 2 years of life, which in turn affects the human capital of future generations. 13
Over the past 2 decades, longitudinal studies of language development in early childhood have been limited.8-10,22-34 Most research has focused on the language progress of children between the ages of 3 and 10, mostly in English-speaking environments. During the first 2 years, no significant differences in semantic language development are observed between children who speak English and those who speak Spanish. 35 However, cultural and risk factors related to birth may affect the rate of acquisition of semantic and phonological aspects. Therefore, it is crucial to conduct studies that combine developmental factors and observe their relevance in explaining development language.
Ecological theories of child development underscore the combination of individual and microsystemic factors to fully understand child development. 36 However, many studies on this topic have overlooked the analysis of language development in conjunction with other developmental variables, such as socio-emotional and economic factors. It is worth noting that much of the research published in prestigious journals comes from high-income countries, which hinders our understanding of child development in low- and middle-income countries. In countries such as Cuba, Brazil, and Peru, there is a high prevalence of children with neurodevelopmental disorders. Therefore, there is an urgent need for research during infancy in more disadvantaged regions of the global south.
Cuba and Auditory Risk Factors at Birth
Cuba, an upper-middle income country, there has been a great deal of research on language development, but there is a paucity of longitudinal studies focusing on infancy. Most of the research on language development during that period has focused on Cuba’s national hearing screening program. This program has identified auditory risk factors in the infant population, such as maternal use of ototoxic medications during pregnancy, low birth weight (<1500 g), prematurity (<28 weeks), and pre-eclampsia.37-42 However, there are a lack of longitudinal studies linking language development to such risk factors and their combination with other variables. Moreover, Cuba has experienced an adverse economic situation for Cuban families over the past decade, 43 which underscores the importance of studying the economic impact on language development.
Current Study
The purpose of this investigation is to examine how different auditory risk factors at birth may predict children’s subsequent language development in the Cuban context. We focused on language development and its association with birth risk factors, as well as their combination with other socio-emotional or socio-economic factors. Our goal was to determine whether these children experience difficulties in language development at 2 years of age when they are affected by additional factors that may complicate their overall development. Our specific research questions are threefold:
How do auditory risk factors at birth affect the development of expressive and receptive language in children with normal hearing at 2 years of age?
What are the differences in language development at 2 years of age between children with and without auditory risk factors at birth?
What is the effect of economic status on the development of children with and without hearing risk factors at 2 years of age?
Methods
Participants
The present IRB-approved investigation used data from the neonatal hearing screening program in the province of Cienfuegos, Cuba conducted between 2018 and 2022. During this period, the provincial hearing center screened a total of 9315 newborns during the first 15 days of life, representing 52% of all births in the province at that time. 44 The remaining children (48%) were screened after the first 15 days of life due to internal health center and family reasons.
This study focused on the first subsample (52% of the children) and selected 136 children who had false-positive neonatal hearing loss screening results. These children were selected in 2 steps: In the first stage, inclusion criteria were (1) children born in 2018, (2) children with false-positive otoacoustic emissions test results at 15 days of age but negative auditory neurophysiology test results. Exclusion criteria were (1) children born between 2019 and 2022, (2) children with both negative and positive results on both auditory screening tests (otoacoustic emissions and auditory neurophysiology).
In the second screening phase, most of the false-positive children were found to have no hearing risk factors, according to the Joint Committee on Infant Hearing (JCIH) guidelines.
Since the specialists performing the otoacoustic emissions tests were experienced in this area, it was decided to divide the sample of 136 children into 2 groups: Group A comprised 105 children with no auditory risk factors at birth and normal hearing, and Group B comprised 31 children with auditory risk factors at birth, but normal hearing. This decision was made because it is possible both groups of children may face difficulties in language development in infancy due to genetic, environmental, or economic factors.
To determine the appropriate sample size, a pilot study was conducted in 2018 and the false positive rate was estimated to be P = 25/1963 = 0.012. Considering precision of i = 0.0183 (1.83%) and a confidence level of 95% (Z = 1.96), the formula n = Z2p(1 − p)/i2 = 136 was applied. Therefore, 136 false positives were considered an adequate sample size, which was achieved by screening 9315 infants during the period 2018 to 2022 (Table 1).
Descriptive Statistics of the Study Variables.

Abbreviations: M, media; SD, standard deviation.
Ethical Approval and Informed Consent
The Scientific Council of the Faculty of Education of the University of Cienfuegos (SCFE-Ucf) approved the research project, reference number PS221LH001-007. The Director of the Hearing Center of Cienfuegos also approved the project activities and the use of data from the Provincial Hearing Screening Program according to the guidelines of the Declaration of Helsinki. The SCFE-Ufc recommended obtaining the approval of the Provincial Hearing Center and obtaining informed parental consent before performing the evaluation at 2 years of age.
Measures: Predictors
Auditory risk factors at birth
(Maternal interview, conducted minutes before the otoacoustic emissions test): The interview aimed to identify three indicators: (1) population (0 = rural, 1 = urban); (2) mother educational level (0 = medium, high school, 1 = high, university); and (3) presence of hearing risk factors according to the JCIH guidelines (ie, family history of hearing loss, mother with Zika disease, mechanical ventilation for more than 5 days, mother with dengue disease, low birth weight (≤1500 g), use of ototoxic drugs, prematurity ≤28 weeks, low Apgar score, mother with varicella disease, mother with HIV, children with malformations).
Social-emotional development
Parents completed the Child Behavior Checklist (CBCL) 45 was administered when children were age 2. The adaptation of the CBCL for Cuban children by Ramirez 45 was used, although the norms used were those of Rescorlas. 46 The CBCL comprises 100 items, is used with children aged 1.5 to 5 years, and includes several scales that empirically assess behavioral and socioemotional. The internalizing and externalizing scales were used in this study. An internalizing profile was considered atypical if the questionnaire scores reached ≥98 percentile, which corresponds to approximately 2 standard deviations beyond the mean. In contrast, it was considered a typical profile if it scored ≤84th percentile. This cut-off point has also been used in other studies.47,48
Measures: Outcomes
Language Development Screening Test (PPDL) (administered at 2 years of age) represents a brief and easy to administer assessment that uses accessible materials (answer sheet, cup, crayon, ball, bucket, and bell). 49 It is used for children aged 0 to 36 months and consists of 42 items that assess 3 domains of language: auditory expressive (19 items), auditory receptive (13 items), and visual (10 items). Finally, the study used the auditory expressive and receptive domains. The child is asked to identify objects and form sentences to assess language development in semantic, phonological, and grammatical terms of the Spanish language. Cuban standards were applied. 49 Children were classified as typically and atypically developing. Typical language development refers to the natural and progressive process by which children acquire language skills in an appropriate and timely manner. This includes the ability to understand and produce sounds, words, sentences, and speech in increasingly complex ways according to their age and stage of development. Conversely, atypical language development refers to situations in which a child has significant difficulties in language acquisition, whether in terms of comprehension, expression, pronunciation, fluency, or appropriate use of grammatical rules.
Data Analytic Procedures
For the first research question addressing how auditory risk factors at birth affect the development of expressive and receptive language cases of normal hearing at age 2 years, the sample of children from Group B (31 with risk factors and normal hearing) was used to perform a contingency table test to analyze the relationship between auditory risk factors at birth and language development at age 2 years. In addition, socioemotional development, maternal educational level, and family socioeconomic status were added as confounding variables in the analyses.
For the second research question addressing the differences in language development at age 2 years in cases with and without auditory risk factors at birth, both Group A and B were used. The non-parametric Mann-Whitney U test was used to determine whether there was a significant difference between the 2 groups with respect to the variables of language development, socio-emotional development, and family socio-economic status.
For the third question addressing the relationship between socio-economic differences in language development at 2 years of age between children with and without auditory risk factors at birth, Group A and B were used to construct a single sample. Since the sample did not meet the assumptions of normality, we proceeded to transform the data into z-scores to meet the requirements of linear regression.
Using the transformed data, several ordinary least squares regressions were conducted to examine the proposed linear relationship between socio-economic exposure, language development at 2 years of age, and other confounders, such as auditory risk factors at birth and socio-emotional development. Specifically, we regressed the language development scores (LANGUAGEi) of each individual i on the auditory risk factors at birth (RISKi). To ensure unbiased estimates, our fully controlled model accounted for possible omitted variable bias and confounding from the country’s economic conditions over the past 5 years (ECONOMYi), pre-existing and concurrent family factors (FAMILYi), and child socioemotional development characteristics (CHILDi) that could have a significant impact on our key variables. In developing the socioeconomic impact variable, several factors were carefully considered to provide a more accurate representation of the variable. Both the influence of specific variables (family socio-economic status) and general indicators of the Cuban economy (GDP per Capita2022 = 56.49, Unemployment Rate2022 = 1.4, GINI Index2022 = 0.40, Human Development Index2019 = 0.78, and Inflation Rate2023 = 45%) were taken into account. These indicators were used because they provide an accurate representation of the actual conditions of the economic environment.

Where (a1 and eit represent the intercept and the stochastic error, respectively):
LANGUAGEiage = receptive language + expressive language + age.
ß1 RISK = auditory risk factors at birth that affect language development (expressive language + receptive language).
ECONOMYi = 0.2 × family socio-economic status+ 0.3 × GDP per Capita2022 + 0.1 × unemployment rate2022 + 0.1 × GINI Index2022 + 0.2 × Human Development Index2019 + 0.1 × inflation rate2023.
FAMILi = socio-economic status of the family + mother’s level of education.
CHILDi = socio-emotional development + age.
Results
Descriptive Statistics
Group A
Table 1 reports descriptive data of the variables analyzed in the study. In group A, it was observed that out of a total of 105 children evaluated in 2022, 55 were boys and 50 were girls, with most of them (72 children) being between 18 and 21 months of age at the time of reevaluation.
None of the children had auditory risk factors at birth. However, at 2 years of age, 10 children showed atypical development in receptive language, while 95 showed typical development. In terms of expressive language, 4 children had atypical development and 101 had typical development. In terms of socio-emotional development, 44 children showed very high internalizing profile, while 61 had typical development for their age. In terms of externalizing profile, 29 children showed very high profile, while 76 showed typical development for their age.
In terms of family environment, 43 children came from families of middle socio-economic status, while 63 came from families of high socio-economic status. In addition, 42 mothers had a medium level of education and 63 had a high level of education, having completed university studies (see Table 1).
Group B
In group B, out of a total of 31 children evaluated in 2022, 15 were boys and 16 were girls, with the majority (22 children) between 18 and 21 months of age at the time of reevaluation. At birth, all were found to have hearing risk factors: family history of hearing loss (16 children present), mother with Zika disease (3 children present), mechanical ventilation for more than 5 days (2 children present), low birth weight (≤1500 g) (6 children present), preterm birth <28 weeks (2 children present), and ototoxic medications (2 children present).
At 2 years of age, 13 children showed atypical development in receptive language, whereas 18 children showed typical development. In terms of expressive language, 1 child had atypical development and 30 had typical development. In terms of socio-emotional development, 2 children had very high internalizing profile, while 29 had typical development for their age. In terms of externalizing profile, 10 children showed very high profile, while 21 had typical development for their age.
Regarding the family environment, 12 children came from families of medium socio-economic status, while 19 came from families of high socio-economic status. In addition, 12 mothers had a medium level of education and 19 had a high level of education, having completed university studies (see Table 1).
Research Question 1. How Do Auditory Risk Factors at Birth Influence Expressive and Receptive Language Development in Children With Normal Hearing at 2 Years of Age?
Table 2 provides results for contingency analysis between auditory risk factors and their combination with language, socio-emotional, and socioeconomic development. Family history of hearing loss in the child at birth significantly predicted children’s receptive language development at 2 years of age. This association was also significant when the control variables of internalizing profile, externalizing profile, family socio-economic status, and maternal education level were considered. The chi-squared values were χ2 = 5.74 with a significance level of P < .01 for each of these variables. As reported in Table 2, the combination of family history of hearing loss and internalizing profile was found to be a risk, as the odds ratio was greater than 1 (OR = 2.19; 95% CI: [6.72, 2.32]).
Contingency Analysis Between Auditory Risk Factors and Their Combination With Language, Socio-Emotional, and Socioeconomic Development.
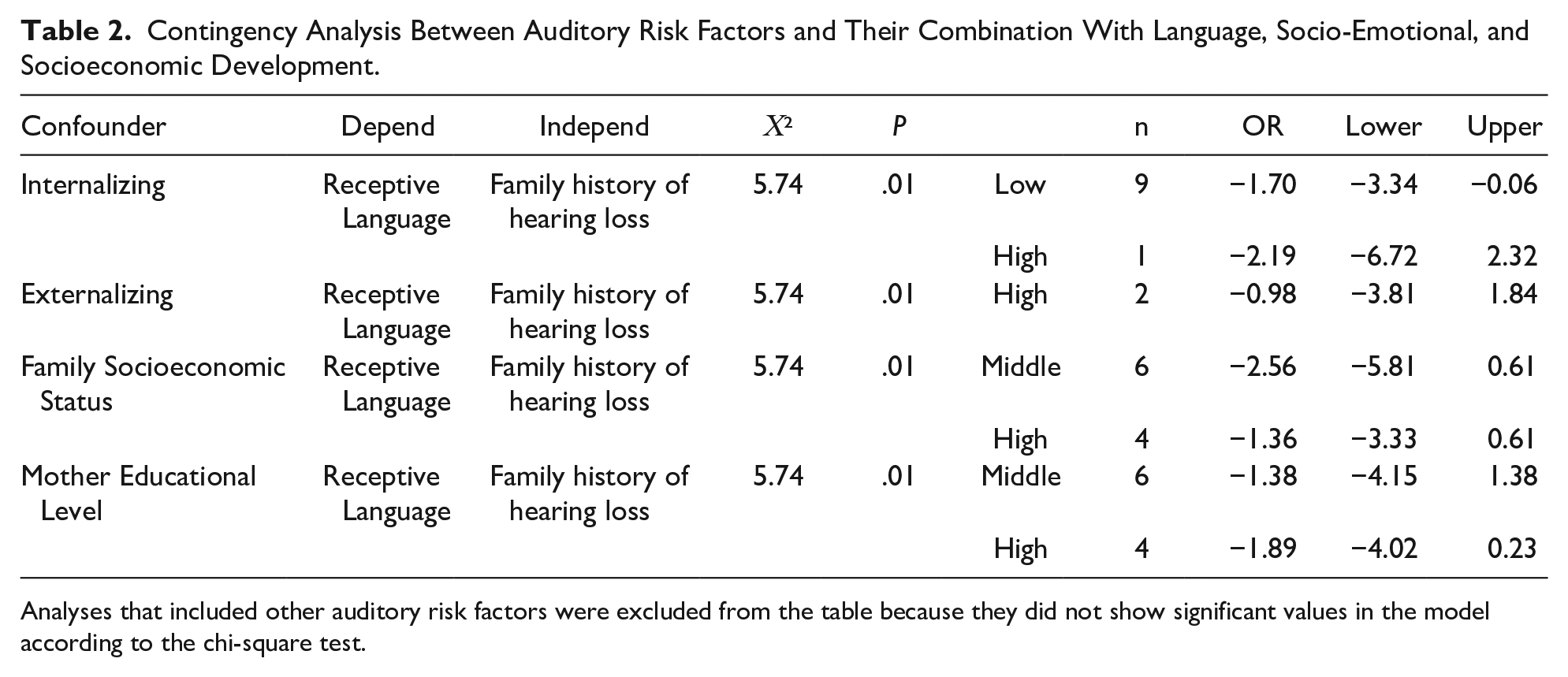
Analyses that included other auditory risk factors were excluded from the table because they did not show significant values in the model according to the chi-square test.
Children with a family history of hearing loss at birth and a high internalizing profile were found to have an increased risk of atypical receptive language development at 2 years of age. The other control variables, combined with family history of hearing loss, did not show significance as the odds ratio values, together with confidence intervals, included the value of 1 (see Table 2).
Research Question 2: What Language Development Differences Are Observed at Age 2 Years Between Children With/Without Risk Factors at Birth?
Table 3 reports equality of Variances Test results that compare the variability of the receptive and expressive language development variables between group A (children without auditory risk factors at birth) and group B (children with auditory risk factors at birth and normal hearing).
Equality of Variances Test to Compare the Variability of the Receptive and Expressive Language Development Variables Between Group A (Children Without Auditory Risk Factors at birth) and Group B (Children With Auditory Risk Factors at Birth and Normal Hearing).

Results showed significant differences only in receptive language development between the groups (U = 2155, P < .001, Cohen’s d = 0.32) (Table 3). Subsequently, a significant difference was found in the internalizing profile of the children at 2 years of age between the two groups (U = 2204, P < .001, Cohen’s d = 0.35), while the remaining variables showed no significant differences. These findings support the hypothesis that auditory risk factors at birth may have a negative impact on children’s language and socio-emotional development.
Research Question 3. What is the Effect of Socio-Economic Status on Children With/Without Hearing Risk Factors at 2 Years of Age?
Table 4 provides unstandardized regression coefficients (with standard errors) reflecting the relationship between language development at age 2 and hearing, socio-economic and socio-emotional development risk factors.
Unstandardized Regression Coefficients (With Standard Errors) Reflecting the Relationship Between Language Development at Age 2 and Hearing, Socio-Economic and Socio-Emotional Development Risk Factors.
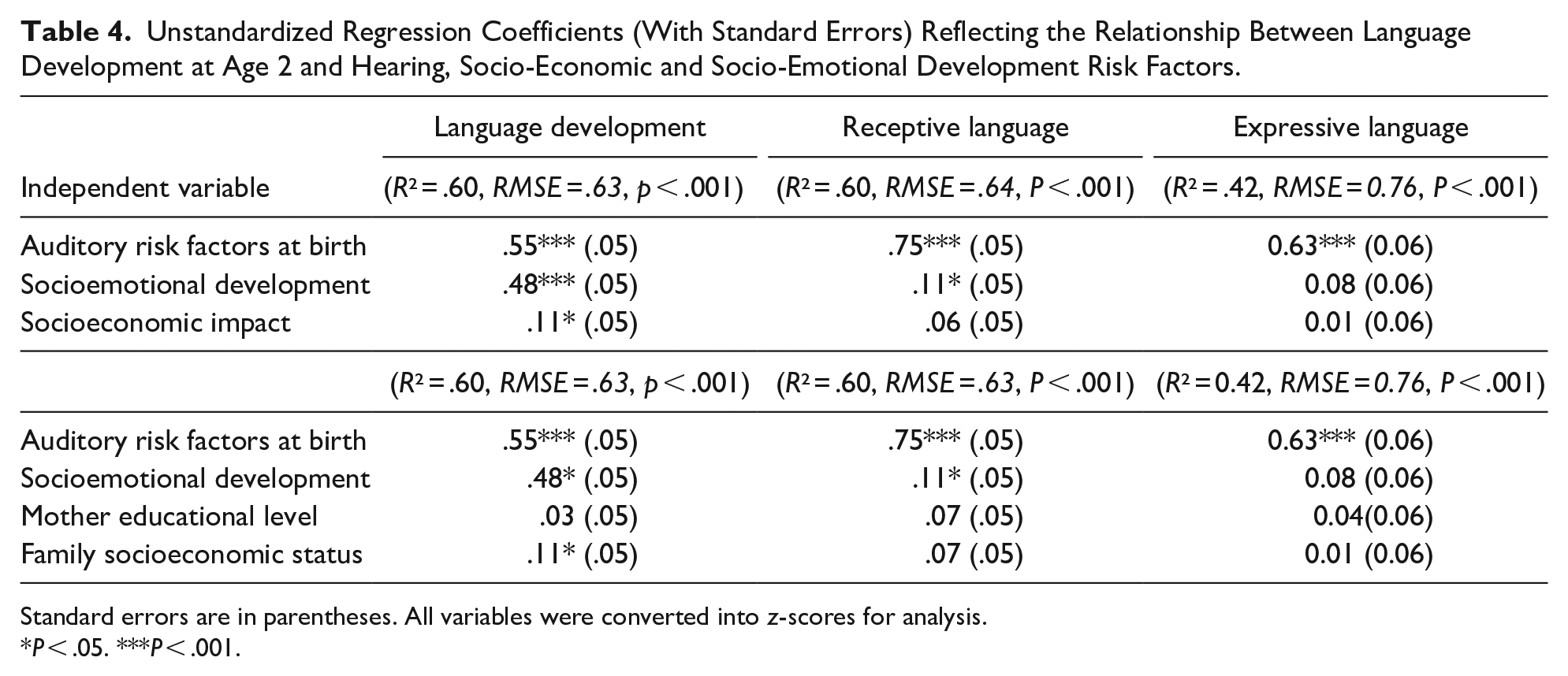
Standard errors are in parentheses. All variables were converted into z-scores for analysis.
P < .05. ***P < .001.
Six linear regressions were computed. Socio-economic status was significantly associated with language development of children, even when confounding variable such as auditory risks at birth and socio-emotional characteristics of the child were considered. The 6 linear regressions showed good model fit, as indicated by the R2 values and the RMSE (Table 4). In addition, it was observed that the socio-economic status of the family, measured by family income, had a significant influence on its own, without the need to consider the global economic indicators of the Cuban economy. The inclusion of these global economic indicators of the country in the last 5 years (such as GDP per capita in 2022, inflation rate in 2023, Gini index in 2022, Human Development Index in 2019 and unemployment rate in 2022) had a significant impact on the analysis.
Discussion
The findings suggest that the presence of auditory risk factors at birth is associated with language development at 2 years of age. More than 40% of children with risk factors at birth evidenced atypical language development. However, this number of children was reduced when the combination of risk factors at birth with other developmental variables was considered. The findings with children with a hearing risk factor at birth indicate that several factors may influence language development at 2 years of age. These include family history of hearing loss, internalizing, externalizing, family socioeconomic status, and maternal education level. An internalizing profile in the first 2 years of life, combined with a family history of hearing loss, was identified as the only significant risk factor for language development. Other factors did not show significance, making it difficult to determine whether they act as risk or protective factors for language development. Nevertheless, it is suggested that family socioeconomic status and maternal education level may play a protective role, as most children with auditory risk factors at birth did not show atypical language development at 2 years of age.
Influenced by both genetic and environmental factors, language development can be significantly affected by gestational factors that affect hearing problems at birth. 50 This makes early detection important. The main motivation behind this study was to investigate the relationship between false-negative results of clinical neurophysiological tests and speech and language development. However, after reviewing the medical records, we realized that not all children presented with the risk factors as consistent variables. Therefore, we set out to investigate the relationship between the 3 variables, focusing on low birth weight and prematurity as significant risk factors that had increased in our province in the last 3 years. These factors had been identified as explanatory for hearing loss in several regions of the country.37-42 This observation led us to hypothesize that the relationship between low birth weight and prematurity might be key, influenced by both national and provincial data. To our surprise, prematurity and low birth weight were not associated with atypical language development at 2 years of age. However, family history of hearing loss did have a significant impact.
The number of false positives found in the analyzed period was remarkable (wherein of 136, 105 without risk factors, and 31 with risk factors). It was striking that children with false positives could have atypical language development at 2 years of age even though they had no auditory risk factors. Although otoacoustic emission testing has an internationally recognized weakness in the presence of many false positives, it is still used as a technique to detect early hearing loss. In this study, it was decided to select all children, since there were few children with auditory risk factors, and we were interested in working with language development, regardless of whether or not they had risk factors.
An important finding of this study was that the combination of socio-emotional and socio-economic development and auditory risk factors at birth significantly predicted language development at age 2. Significant differences were observed between groups A (without risk factors at birth) and B (with risk factors at birth), especially in the internalizing profile and language development. These findings suggest that auditory risk factors at birth may play a critical role in children’s socio-emotional and language development during the first 2 years of life. The presence of these risk factors may influence children’s emotional relationships and their ability to acquire and use language appropriately.
An important factor influencing children’s overall development is the level of monthly family income, which was found to have a significant impact on children’s overall development, even after controlling for the effect of socio-emotional development and the presence of risk factors at birth.
In the specific context of Cuba, it is important to note that the economic difficulties experienced in the last 5 years due to the pandemic, an economic embargo, and the tensions arising from the conflict between Russia and Ukraine have had a significant impact on Cuban families and, consequently, on child development. In this sense, the present study suggests the analysis of family income in future research since the socio-economic effects have a long-term impact on the family and the child.
The present longitudinal study has some important limitations. First, this study found associations between auditory risk factors at birth, language development, socio-emotional development, and family socio-economic status. However, it was not possible to establish a causal relationship between these factors. Therefore, further research is needed to better understand these relationships. Second, the sample used in the study was small, which may have affected the generalizability of the findings. For example, previous studies have used samples of more than 1000 infants, highlighting the need to consider more representative samples in future research.22-24 Such limitations represent a challenge for future research in the Cuban educational context, since the health program includes all children born during the year, but it is necessary to provide adequate and systematic follow-up of language development in infancy.
It is essential to address this issue in Cuba, especially given its economic challenges and educational and health challenges that the country is facing. The findings of this study can be an impetus to further improve the education and health systems in Cuba, based on best practices and informed decisions. These considerations can contribute significantly to the continuous improvement of education and health in the country.
Conclusion
This study underscores the importance of sensitizing medical and allied professionals at birth about hearing assessments and a comprehensive approach to language development during the early years. It underscores the contribution of physical assessment as well as socio-economic and socio-emotional assessment factors. It also highlights the need for policies and programs that support families, especially in the context of economic hardship, to promote optimal language development in children during this crucial period.
Footnotes
Acknowledgements
We would like to thank the Hearing Screening Program in Cienfuegos, directed by the Hearing Center of the province. We thank the children and parents who participated in the study, as well as Dr. Nelson Geroy Amador for his collaboration in the data analysis. We also thank Dr. Shawn Carlson, Ph.D., Purdue University, USA, for reviewing the English text.
Author Contributions
YR: Contributed to conception and design; Contributed to analysis; Drafted the manuscript; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. YC: contributed to acquisition de los dates; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. SA: contributed to acquisition de los dates; Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. LSP: Critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Data Availability
All authors had full access to the data and take responsibility for its integrity and accuracy of analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was carried out within the framework of the National Project “Evaluation of the Impact of Scientific Results on the Quality of Education” (Code PS221LH001-007), associated to the Sectoral Program “Cuban Educational System. Development Perspectives” (Code PS221LH001).