
Abstract
The aim of this study is to evaluate the prevalence of low birth weight and other perinatal risk factors in children diagnosed with neurodevelopmental disorders. This is one of the first studies in the Arabian Gulf region focused on the contribution of these factors toward the development of various disorders such as attention-deficit/hyperactivity disorder, autism spectrum disorder, and other mental disorders. This descriptive study was based on qualitative data analysis. We reviewed retrospective information from the electronic medical records of 692 patients in Dubai, United Arab Emirates. The prevalence of low birth weight in children with mental disorders was significantly higher as compared to the general population (16% vs 6% respectively). Furthermore, other risk factors, including high birth weight and preterm birth were noted to have a significant association with neurodevelopmental disorders. Future research on the impact of perinatal risk factors will contribute to advancement of early intervention guidelines.
Introduction
Low birth weight in newborns has become an issue of significant concern in many parts of the world. According to UNICEF data (2019), approximately 21 million babies die of being born low birth weight every year, which represents 15% of the world’s newborns. 1 This study aims to shed light on the prevalence of low birth weight in children and adolescents who develop neurodevelopmental disorders.
Neurocognitive illnesses, including neurodevelopmental disorders, have become one of the main causes of the overall disease burden worldwide. 2 Recent studies have indicated a higher prevalence of neurodevelopmental abnormalities in patients who were below normal birth weight. 3
Research in this field in the Arabian Gulf region, and particularly in the United Arab Emirates (UAE), is lacking. Since neurodevelopmental disorders contribute to enormous burden on quality of life, research toward identifying risk factors is highly warranted. This will subsequently contribute to developing early preventative measures.
Methods
A descriptive research approach was implemented for this study where information was extracted from patient medical records. Data were extracted from mental health intake forms, completed prior to the initial assessment, and diagnoses based on the psychiatric assessment by certified child and adolescent psychiatrists of the Mental Health Center of Excellence at Al Jalila Children’s Specialty Hospital. The data was collected retrospectively over a time frame that included all available patient intake forms from August 30, 2017 to September 9, 2018.
The main inclusion criteria for this study was established to include all pediatric cases from 1 to 18 years of age that were assessed by psychiatrists at Al Jalila Children’s in the allocated time frame. A total of 692 charts were reviewed. The exclusions were listed based on missing intake forms, incomplete assessment, absent appointments, and those that did not meet criteria for mental illness according to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) 4 (Figure 1).

Breakdown of reviewed charts and referrals to Al Jalila Children’s Mental Health Services in the timeframe between August 30, 2017 and September 9, 2018.
The data was tabulated using a Microsoft Excel Sheet where demographic data relevant to the study was included, without recording any identifying information.
The diagnoses were based on the Diagnostic and Statistical Manual fifth Edition (DSM-5) criteria, and included attention-deficit/hyperactivity disorder (ADHD), autism spectrum disorder (ASD), language disorder, learning disorder, intellectual disability, and tic disorders. Besides these neurodevelopmental disorders, other common mental disorders that were presented to the outpatient clinics were also included; namely anxiety disorders, major depressive disorder (MDD), bipolar disorder, post-traumatic stress disorder (PTSD), obsessive compulsive disorder (OCD), and eating disorders.
Birth weight being the key variable in this study was included as a numerical data. Perinatal factors with regards to pregnancy that potentially increased the risk of low birth weight were also included such as smoking, alcohol, or drug abuse by the mother during pregnancy. 5 Gestational age in accordance to the WHO classification of term and preterm, was also deemed relevant and was included in this study.
Family history was previously discussed to be of significance when it comes to mental disorders and their prevalence.6,7 Considering the strong genetic component that is associated with mental disorders, and more particularly in attention-deficit/hyperactivity disorder and autism spectrum disorder, and the genetic overlap between the 2 disorders that has been observed in previous studies; 8 a family history showing the presence of these 2 neurodevelopmental disorders has also been included as a variable in this study.
SPSS version 24.0 was used to analyze the prevalence of low birth weight and other risk factors in this pediatric population diagnosed with neurodevelopmental disorders.
Ethical Approval and Informed Consent
No patients were excluded from this study based on racial, gender, religious, or cultural backgrounds. Consent was not required for this study, as it was based on assessing anonymous archival data. The local ethical review boards, at Mohammed Bin Rashid University of Medicine and Health Sciences (MBRU), and Dubai Healthcare City Authority (DHCA), approval was sought before conducting the study under the IRB approval MBRU/IRB/SRP2018-035.
Results
The study sample consisting of 210 patients had an age group distribution ranging from 1 to 17 years old with a mean age of 8 years ± 3.75SD. There was no missing data recorded in terms of age. According to the results, 168 out of the 210 patients in this population were males and 42 were females. This shows that males represent 80% of the patients’ sample during the study timeframe, that is, a 4:1 ratio of males to females.
Birth weight is a key variable in this study and the prevalence in our sample for patients born normal birth weight is 70% of the sample size. The maximum birth weight reported was 4500 g (9.92 lb) whereas the lowest was 730 g (1.6 lb) with the mean birth weight at 2940 g ± 0.73SD (6.48 lb ± 0.73SD).
A noteworthy observation is that 16% of the research population were born low or very low birth weight. The prevalence of high birth weight in the study sample was 3%. The total of cases with no reported birth weight, that is, missing data, was 22 (10%) (Figure 2).

Birth weight distribution.
Smoking, alcohol intake, and drug abuse were also explored during the study. There was no significant trend noticed in this data with only 2 reported cases of smoking, 1 reported case for drug abuse during pregnancy, and no cases with reports of alcohol consumption. A significant portion (46%) of this data was classified as “missing.”
The gestational age at delivery, particularly the rate of preterm birth, was another key finding from these results where 15% of the patients in this sample were born preterm. The results acquired from patient diagnoses of mental disorders had 187 (89%) patients diagnosed with at least 1 neurodevelopmental disorder. From these, 32 (17%) patients were born low birth weight. The results are illustrated with how neurodevelopmental as well as other mental disorders correlate with the different ranges of birth weight in Figure 3.

Overlap between mental disorders and birth weight.
On analyzing a possible correlation between neurodevelopmental disorders and patients born low birth weight, we found no significant association between the 2 variables (Chi-Squared P >.05). On the contrary, high birth weight patients had a significant association with developing neurodevelopmental disorders (Chi-Squared P < .05).
Comorbidities in more than 1 diagnosed mental disorder, ranging from 39% of patients diagnosed with at least 2 mental disorders up to 3% of patients diagnosed with 4 mental disorders were observed in this sample of 210 patients (Table 1).
Number of Comorbid Mental Disorders.

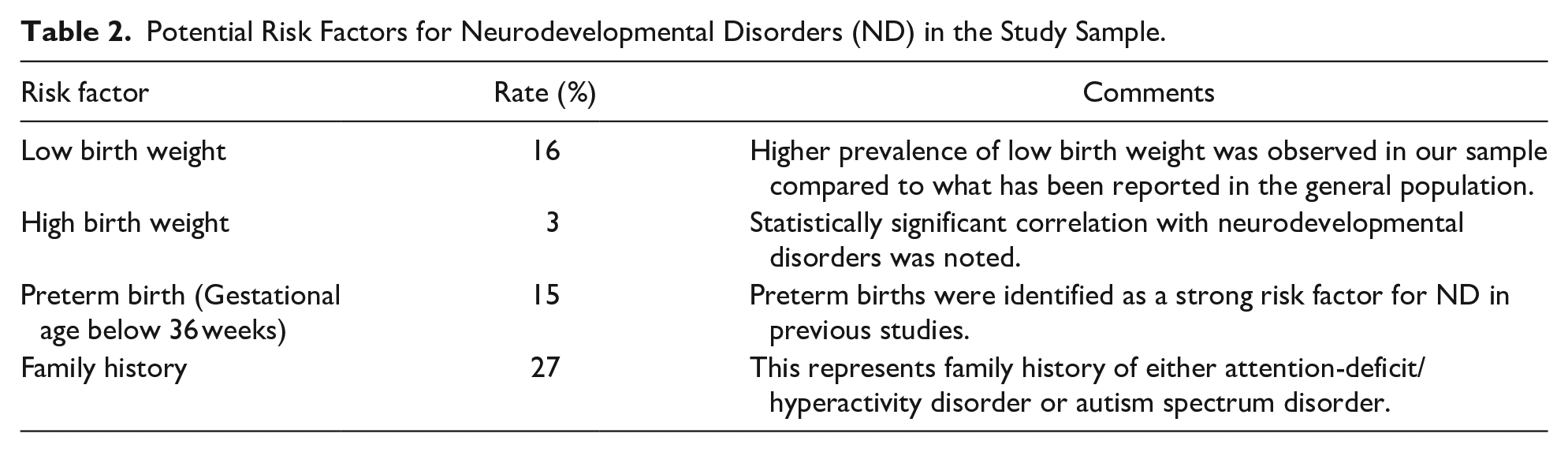
According to the data extracted, 56 patients (27%) had a positive family history of either ADHD or ASD. Table 2 summarizes the correlation to the rates of potential risk factors for neurodevelopmental disorders in our sample, including rates of low birth weights, high birthweights, gestational age, and family history.
Potential Risk Factors for Neurodevelopmental Disorders (ND) in the Study Sample.
Discussion
Previous research has explored multiple factors contributing to the development of neurodevelopmental disorders, including gender, perinatal risks, and family history. These will be discussed and correlated to our findings in the following section.
Based on worldwide research exploring the gender ratio in mental disorders, it was noted that the prevalence of males: females was 4:1.9,10 This is in line with our findings. Females probably present less often to mental health services due to multiple reasons. One of the possible reasons could be the hypothesis of the difference in spatial development of the brain, which allows the female brain to take advantage of certain “protective factors.” 11 Another possible explanation is the reporting bias that is encountered with female patient intake, where females tend to seek medical help on a higher level of severity. 11
The World Health Organization (WHO) defines low birth weight as a weight at birth being less than 2500 g (5.5 lb). A birth weight of below 1500 g (3.3 lb) is classified as “very low birth weight” while a birth weight of above 4000 g (8.8 lb) is defined as “high birth weight.” 12 The overall prevalence of low birth weight in the Gulf Cooperation Council (GCC) countries has been found to be 8.5% with the United Arab Emirates at a prevalence of 6% of the country’s population. 13 Low birth weight can drastically affect the quality of life and make the newborn prone to an increased risk of hypothermia, impaired nutrition, ophthalmological complications, immune disorders, hearing defects as well as long term cognitive and motor impairments.14-16
The prevalence of low birth weight in the general population in the United Arab Emirates was estimated to be 6%. 13 Our study concluded a prevalence of 16% for children born low birth weight. This is significantly higher than the prevalence in the GCC being 8.5% for babies born low birth weight, 13 as well as the worldwide estimate of preterm births being 9.5%. 17 However, this could possibly be due to our sample not being representative of the general population, where the population was selected based on patients presenting to mental health services in a tertiary care institution. This could have added to a selection bias, which lead to an increased prevalence in low birth weights.
Some of the maternal factors that put the fetus and the mother at risk of complications during pregnancy include smoking, alcohol intake, and drug abuse. 5 Although a large component of our data on maternal social history was classified as missing, this further highlights the challenges of conducting research in a background of cultural sensitivity and under-reporting of information on this topic. Research has also shown that gestational age, and particularly preterm birth, increases the rates of complications in the newborn. 18 Preterm birth is defined by the World Health Organization as infants born alive before the completion of 37 weeks (term) of pregnancy. 19 Family history is also known to have a significant impact on the occurrence of neurodevelopmental disorders.6,7
Studies have also shown that individuals who were born very preterm have higher rates of psychiatric diagnoses compared to term-born controls. 20 This also highlights the factors included in this study, such as preterm births playing a vital part in the increase in prevalence of low birth weight which has been previously reported. 21 Our sample demonstrated a 15% prevalence of preterm births in children and adolescents with neurodevelopmental disorders. This supports the current trends of high prevalence of neurodevelopmental disorders and preterm births seen in studies with larger sample sizes worldwide.22-24 Further research is needed to explore the specific risk factor(s) involved in affecting the birth weight status.
In the context of ADHD and ASD being the most prevalent neurodevelopmental disorders, there has been extensive research done in identifying a familial component often found in ASD and ADHD between siblings in twin studies as well as first degree relatives. 8 Our study observed that 27% of the patients diagnosed with mental disorders had a positive family history for ASD or ADHD present. On exploring further, we also noticed that 30% of these patients who had a positive family history were also diagnosed with ADHD or ASD. This might contribute to the significant genetic component established in previous studies conducted on these 2 neurodevelopmental disorders and encourages further research into identifying their heritability. 8
However, it was difficult to determine an association in this study with regards to family history because we expect under-diagnosis of mental health conditions in the previous generations in this region due to the lack of mental health awareness and services. The information on family history used in this study was obtained from health intake forms that were completed by parents, which probably was influenced by information bias as well.
Interestingly, high birth weight seemed to show a significant association with neurodevelopmental disorders. Previous studies have revealed that risk factors leading to high birth weight includes post term birth. 25 Additionally, research has proposed that infants born post term are exposed to decreased blood flow to the brain due to the changes that affect the placenta in the post term period. 26 The finding in our study as well as previous research probably highlights that further study needs to be done in understanding this pathophysiology on a more clinically relevant level.
Regarding the strengths of this study, we made sure to include all the patients in the set time frame from August 30, 2017 to September 9, 2018. This helped reducing selection bias in the study. Another positive aspect to this study was the variety of mental disorders that were looked at with regards to low birth weight in the pediatric population. In terms of limitations, there was no statistical association observed between infants born low birth weight and developing neurodevelopmental disorders, however, due to the study design it aimed to describe the prevalence rather than assess an association between these variables. The reliability of this non-association is also questionable due to the selection bias in this sample. Another limitation to this study could have been in the form of a recall bias due to missing information encountered in various parts of the intake form during the data collection phase. Gestational age was classified to be “less than 36 weeks” as “1,” indicating preterm births, and “36 or greater” as “0” for babies born at term. This limited the scope of the study for exploring gestational age even further and warrants further research on this topic.
In conclusion, we found a high prevalence of low birth weight, and preterm birth in children and adolescents presenting to a tertiary care institution and being diagnosed with a neurodevelopmental disorder. The presence of low birth weight was not statistically significant in our sample as a correlation with development of neurodevelopmental disorders. Furthermore, family history of ADHD as well as ASD was high in the sample included in our study which probes the need for future research on statistically relevant correlations on these most common neurodevelopmental disorders. This is the first study to our knowledge that has explored risk factors for neurodevelopmental disorders in Dubai, United Arab Emirates. Future research, using other methodologies, for instance a case-control design that includes a healthy population control group as well as larger sample size in the form of a longitudinal study, along with exploring potential correlations between the rate of low birth weights and patients with 2 or more neurodevelopmental disorders is warranted. This will probably help in better understanding of potential modifiable risk factors for these neurodevelopmental conditions that have a long-term significant functional impact.
Footnotes
Acknowledgements
We would like to thank the Research Committee at Mohammed Bin Rashid University for facilitating this study and Al Jalila Children’s Specialty Hospital for their approval. Special thanks to Dr. Amar Hassan, Associate Professor of Biostatics at Mohammed Bin Rashid University, Mr. Hawk Kair, Psychologist at Al Jalila Children’s Specialty Hospital and Mr. Abdul Rahman Yusuf Ali, Medical Student at Mohammed Bin Rashid University, for their support and expertise with the statistics involved in this study. Many thanks to all the members of the Mental Health Centre of Excellence at Al Jalila Children’s Specialty Hospital for conducting comprehensive multidisciplinary assessments. We also thank Dr. Yasser Ad-Dab’bagh, Consultant Child and Adolescent Psychiatrist at King Fahad Specialist Hospital, for his guidance and support.
Author Contributions
FAN: Contributed by conducting the literature search and review; study design; developing the data collection tool, data analysis, and manuscript preparation.
MAS: Contributed to developing the research question; study design; literature review, revision of the data analysis, manuscript preparation, and supervised the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.