
Abstract
Objective:
This study aimed to identify maternal and neonatal risk factors associated with admission to special or intensive neonatal care in a referral hospital in Indonesia.
Methods:
A hospital-based cross-sectional study was conducted from November 2024 to April 2025. Data were collected from medical records and analyzed using binary logistic regression. Adjusted odds ratios (AOR) with 95% confidence intervals (CI) were reported, with P < .05 considered significant.
Results:
Among 348 neonates, 60 (17.2%) were admitted to special or intensive neonatal care. Significant predictors included no antenatal care attendance (AOR: 2.54; 95% CI: 1.23, 5.24), low birth weight (AOR: 3.07; 95% CI: 1.28, 7.34), Apgar score <7 at first minute (AOR: 7.87; 95% CI: 3.70, 16.73), and preterm birth (AOR: 5.69; 95% CI: 2.50, 12.92).
Conclusion:
No antenatal care attendance, low birth weight, low Apgar score, and preterm birth were independent predictors of neonatal care admission.
Introduction
Neonatal morbidity and mortality represent critical public health challenges in low- and middle-income countries (LMICs), particularly among infants requiring advanced levels of care immediately after birth. Globally, complications related to prematurity account for approximately 40% of neonatal deaths, emphasizing the urgent need for early risk identification and appropriate neonatal support. 1 In LMICs, poor neonatal outcomes often result from limited neonatal intensive care capacity, delayed referrals, and inadequate prenatal surveillance.2,3
According to the World Health Organization (WHO), an estimated 2.3 million newborns die within the first month of life each year, with nearly three-quarters of these deaths occurring during the first week. The leading causes include preterm birth complications, intrapartum-related events, and neonatal infections. WHO emphasizes that improving the quality of care around the time of birth and expanding access to essential newborn interventions—particularly for small and sick infants, are pivotal strategies to accelerate progress toward ending preventable neonatal mortality. 1
Several studies across diverse settings have consistently identified factors such as gestational age, birth weight, Apgar score, and the quality of antenatal care (ANC) as significant predictors of admission to the neonatal intensive care unit (NICU).4 -6 In a Romanian population-based study, maternal age ≥35 years, preeclampsia, and peripartum infections were associated with increased risk of NICU admission (odds ratios ~1.6-2.3). 7 Similarly, a Swedish cohort demonstrated that a low 5-minute Apgar score strongly predicts neonatal death even among preterm infants, underscoring the clinical value of early postnatal assessment. 4
Moreover, meta-analytic evidence indicates that advanced maternal age (≥35 years) increases the risk of obstetric complications such as preeclampsia, gestational diabetes, and preterm delivery, thereby elevating the likelihood of neonatal morbidity and subsequent NICU admission. 8
At the policy level, the Every Newborn Action Plan (ENAP) a global strategy jointly led by WHO and UNICEF calls for integrated maternal and newborn care, emphasizing early identification of at-risk pregnancies, improved intrapartum management, and equitable access to quality neonatal services to reduce preventable newborn deaths. Recent updates of the ENAP and Ending Preventable Maternal Mortality (EPMM) framework highlight the need to accelerate progress toward high-quality, facility-based care for small and sick newborns within Universal Health Coverage. In alignment with these global strategies, generating context-specific evidence from hospital-based studies is crucial to inform national and regional efforts to optimize neonatal outcomes. 9
Therefore, this study aimed to determine maternal and neonatal risk factors associated with the need for special or intensive neonatal care admission at RSUD Haji Provinsi Jawa Timur (Haji Provincial General Hospital of East Java), a provincial referral hospital in Surabaya, East Java, Indonesia. Recognition of these predictors is expected to improve early clinical decision-making and contribute to reducing preventable neonatal morbidity and mortality in similar low-resource settings.
Materials and Methods
Study Setting and Period
The study was conducted from November 2024 to April 2025 at RSUD Haji Provinsi Jawa Timur (Haji Provincial General Hospital of East Java), a provincial referral hospital in Surabaya, East Java, Indonesia (hereafter referred to as RSUD Haji). The hospital is a government-owned secondary referral hospital providing comprehensive obstetric and neonatal care services.
The neonatal care services include routine neonatal care, special neonatal care, and Neonatal Intensive Care Unit (NICU) facilities. Based on international neonatal care classification standards established by the American Academy of Pediatrics, the hospital provides Level II neonatal care, which includes continuous monitoring, thermoregulation, intravenous therapy, respiratory support such as continuous positive airway pressure (CPAP), and limited mechanical ventilation for moderately ill and preterm neonates, as well as stabilization of critically ill newborns prior to referral when advanced subspecialty care is required. 10 The neonatal unit consists of approximately 4 NICU beds and 6 special neonatal care beds. The hospital manages approximately 703 deliveries annually.
Study Design and Population
A hospital-based cross-sectional study design was employed.
The source population included all live-born neonates delivered at RSUD Haji during the study period. The study population consisted of all live-born neonates delivered at the hospital and admitted to routine neonatal care, special neonatal care, or the neonatal intensive care unit (NICU) between November 2024 and April 2025.
Data were obtained from both electronic and printed hospital medical records. Deliveries occurred in the Emergency Department, Delivery Room, or Operating Room, depending on the clinical condition and urgency of the mother.
Neonates were included if complete maternal and neonatal medical records were available. Neonates with intrauterine fetal death (IUFD), major congenital anomalies, or incomplete medical records were excluded from the study.
Sample Size Determination and Sampling Procedures
A total population sampling approach was used. All live-born neonates delivered during the study period who met the inclusion criteria were included in the analysis. A total of 348 neonates were eligible and included in the final study sample.
Variables
Dependent variables
Admission to neonatal care units (routine neonatal care or higher-level neonatal care [special neonatal care or neonatal intensive care unit]).
Independent variables
Mode of delivery, maternal age, parity, mode of hospital arrival, antenatal care attendance, low birth weight, gestational age, and Apgar score.
Data Collection Tools and Procedure
Data were collected using a structured extraction checklist developed after reviewing relevant literature and similar studies. The checklist, prepared in English, covered maternal socio-demographic characteristics, obstetric history, antenatal care status, and neonatal factors such as birth weight, gestational age, Apgar score, and admission status (routine care, special care, or intensive care).
Data extraction was conducted directly by the principal investigator from both electronic and printed medical records of neonates admitted during the study period. The checklist ensured consistency and completeness of the data, and key variables were carefully verified. The entire process was performed independently by the investigator in compliance with ethical standards of confidentiality and data protection.
Data Quality Control
To ensure data quality, a structured extraction checklist was carefully designed and pretested on 5% of the sample (17 neonatal records) before the actual data collection. This pretest helped confirm that the variables were consistent and clearly documented in the patient medical charts. During the main data collection, the principal investigator independently reviewed each record, verified completeness, and cross-checked key variables to minimize missing data or inconsistencies. Any discrepancies identified during the process were immediately addressed to ensure accuracy and reliability of the dataset.
Data Processing and Analysis
Data were entered, coded, and cleaned using SPSS version 25. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were computed after assessing the distribution of the data. The assumptions of the binary logistic regression model were verified using the Hosmer–Lemeshow goodness-of-fit test, with a P-value > .05 considered to indicate a good model fit.
All independent variables were included in the multivariable logistic regression model regardless of their significance in the bivariate analysis to control for potential confounding effects. Multicollinearity was assessed using variance inflation factor (VIF) <10. In the final model, a P-value ≤ .05 was considered statistically significant. Adjusted odds ratios (AOR) with 95% confidence intervals were reported to assess the strength of association between independent and dependent variables. Potential confounding factors were examined and controlled for during the analysis.
Operational Definition
Admission to neonatal care unit
The level of neonatal care to which the newborn was admitted immediately after delivery was classified as routine care (rooming-in or well-baby nursery), special neonatal care (perinatology care unit), or neonatal intensive care unit (NICU). The level of care was determined by the attending pediatrician (neonatologist or general pediatrician) based on the newborn’s clinical condition and standard hospital protocols.
For the purpose of analysis, special neonatal care and NICU admissions were combined into a single composite outcome representing the need for enhanced clinical monitoring and medical management beyond routine newborn care. Both levels of care reflect clinically significant neonatal conditions requiring increased surveillance, therapeutic interventions, or intensive support. This composite outcome was used to capture the overall burden of neonatal morbidity requiring escalation of care and to improve statistical robustness.
Mode of delivery
Classified as vaginal delivery (spontaneous or operative vaginal delivery) and cesarean section (elective or emergency).
Maternal age
The chronological age of the mother at delivery, categorized as <35 years (optimal reproductive age, low risk) and ≥35 years (advanced maternal age, high risk).
Parity
The number of live births the mother had before the index delivery, classified as primipara (1) and multipara (≥2).
Mode of maternal arrival to hospital
The way the mother arrived at the hospital for delivery, categorized as referred (via outpatient or antenatal referral system) or direct self-arrival (direct walk-in without referral).
Antenatal care (ANC) attendance
ANC attendance was defined based on documented ANC visits at the study hospital during pregnancy. Women with at least 1 recorded ANC visit were classified as having ANC attendance at the study hospital, while those without any documented visit were classified as having no ANC attendance at the study hospital. This classification reflects ANC utilization at the study hospital and may not capture ANC received at other healthcare facilities.
Low birth weight
A new born with weight less than 2500 g will considered as low birth weight irrespective of gestational age. 11
Apgar score
Composite score (0-10) assessed at 1 and 5 minutes after birth, based on appearance, pulse, grimace, activity, and respiration. Categorized as normal (≥7) and low (<7).
Gestational age
The duration of pregnancy calculated from the first day of the last normal menstrual period (LNMP) or by early ultrasound estimation. Categorized as term (≥37 completed weeks) and preterm (<37 completed weeks).
Ethical Approval and Informed Consent
This study was approved by the Health Research Ethics Committee of RSUD Haji, East Java, Indonesia (Approval No: 445/168/KOM.ETIK/2025). The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
As this study involved a retrospective review of anonymized medical records, the requirement for informed consent was formally waived by the Health Research Ethics Committee. All data were fully anonymized prior to analysis, and no identifiable personal information was accessed or recorded. Permission to access hospital medical records was also obtained from the hospital administration.
Results
Socio-Demographic Characteristics of Mothers and Neonates
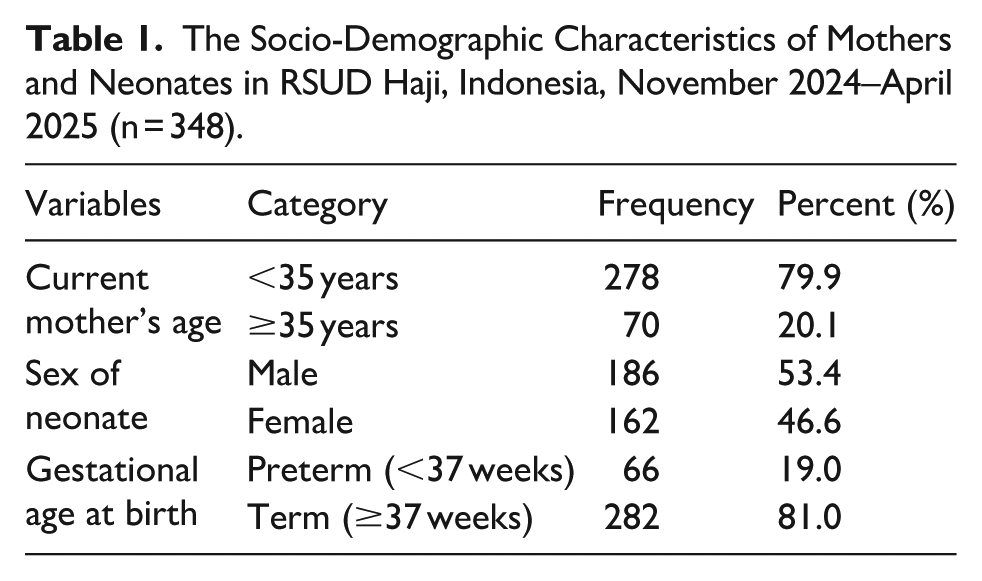
A total of 351 neonatal records were initially reviewed. After excluding 3 records due to intrauterine fetal death (IUFD), 348 live-born neonates were included in the final analysis. As shown in Table 1, most mothers were younger than 35 years (79.9%), while 20.1% were aged 35 years or older. Slightly more than half of the neonates were male (53.4%). The majority of births occurred at term gestation (≥37 weeks) accounting for 81.0% of deliveries, whereas 19.0% of neonates were born preterm (<37 weeks).
The Socio-Demographic Characteristics of Mothers and Neonates in RSUD Haji, Indonesia, November 2024–April 2025 (n = 348).
Maternal, Obstetric, Neonatal and Health Service Related Characteristics
The maternal, obstetric, neonatal, and health service-related characteristics of the study participants are summarized in Table 2. More than half of the mothers were multiparous 203 (58.3%), and a similar proportion of deliveries were by cesarean section 207 (59.5%). Most mothers had registered for antenatal care 231 (66.4%) and the majority arrived through outpatient referral 268 (77.0%). Among neonates, most infants were classified as non–low birth weight 302 (86.8%) and an Apgar score ≥7 at first minute 274 (78.7%).
Maternal, Obstetric, Neonatal, and Health Service-Related Characteristics at RSUD Haji, Indonesia, November 2024–April 2025 (n = 348).

Factors Associated With Admission to Special or Intensive Neonatal Care
The results of the bivariate and multivariable logistic regression analyses are presented in Table 3. Bivariate analysis showed that several maternal and neonatal factors were associated with the likelihood of neonatal admission to special or intensive care units. Model goodness-of-fit was assessed using the Hosmer–Lemeshow test. The result indicated a good fit between the model and the observed data (χ2 = 9.35; df = 8; P = .314), suggesting that the logistic regression model adequately describes the data. After adjusting for potential confounders in the multivariable analysis, no antenatal care attendance, low birth weight, low first-minute Apgar score, and preterm birth were independently associated with increased odds of special or intensive neonatal care admission. Newborns with an Apgar score at first-minute <7 had approximately 8-fold higher odds of special or intensive care admission (AOR: 7.87; 95% CI: 3.70, 16.73). Similarly, preterm neonates (<37 weeks) were about 6 times more likely to require special or intensive care (AOR: 5.69; 95% CI: 2.50, 12.92), and low-birth-weight infants (<2500 g) had 3-fold higher odds (AOR: 3.07; 95% CI: 1.28, 7.34). Mothers who did not attend antenatal care were 2.5 times more likely to have neonates admitted to special or intensive care (AOR: 2.54; 95% CI: 1.23, 5.24; Table 3). In the bivariate analysis, low birth weight showed a strong crude association with special or intensive care admission (COR: 10.24; 95% CI: 5.17, 20.29). After adjusting for gestational age and Apgar score, the association attenuated (AOR: 3.07; 95% CI: 1.28, 7.34), indicating a confounding effect from these perinatal factors.
Analysis of Factors Associated with Special or Intensive Neonatal Care at RSUD Haji, Indonesia, November 2024–April 2025 (n = 348).

Abbreviations: SVD, spontaneous vaginal delivery; CS, cesarean section; COR, crude odds ratio; AOR, adjusted odds ratio.
Significant at (P-value ≤ .05).
Discussion
This study identified 4 key predictors of neonatal admission to special or intensive care units: no antenatal care attendance at RSUD Haji, low birth weight, low first-minute Apgar score, and preterm birth. These findings are consistent with previous studies and highlight the importance of prenatal surveillance and early neonatal assessment.1,2,4 The observed confounding between birth weight and gestational age is biologically plausible, as preterm birth frequently results in low birth weight, both contributing to an increased need for intensive neonatal care. Adjusting for these factors revealed the independent effects of each variable, in line with findings from similar hospital-based studies.
Although special neonatal care and NICU admission represent different levels of care intensity, both reflect clinically important neonatal conditions requiring escalation beyond routine care. The use of a composite outcome allowed comprehensive identification of neonates requiring enhanced monitoring and treatment, although the severity of conditions may vary between levels of care.
No antenatal care attendance at RSUD Haji was associated with a 2.54-fold increased likelihood of neonatal admission, consistent with previous evidence indicating that inadequate ANC results in missed opportunities for early detection and management of pregnancy-related complications.3,9,12,13 A systematic review in Indonesia reported that inadequate ANC was linked to adverse neonatal outcomes, noting that mothers with fewer than 4 ANC visits had significantly higher risks of delivering low birth weight infants (OR = 6.29) and experiencing neonatal mortality (OR = 2.59). 12 A systematic review and meta-analysis conducted in sub-Saharan Africa reported that attending at least 1 antenatal care (ANC) visit with a skilled health provider significantly reduced the risk of neonatal mortality by approximately 39% (RR = 0.61; 95% CI: 0.43-0.86). This finding underscores the crucial role of ANC in preventing adverse neonatal outcomes through early detection and management of maternal and fetal complications. 13
Preterm birth, defined as delivery before 37 completed weeks, is widely recognized as a strong predictor of neonatal intensive care unit admission. Studies from high- and low-income settings consistently report elevated respiratory morbidity in preterm infants. For instance, recent evidence demonstrates that respiratory distress syndrome occurs substantially more frequently in preterm groups than in term infants. 14 Recent systematic reviews have shown that up to 40% of very preterm infants experience hypothermia shortly after birth, which is associated with increased mortality and morbidity. 15 Similarly, in low-resource settings, over 70% of preterm neonates still exhibit hypothermia within 24 hours of admission. 16 Premature infants commonly face respiratory distress, hypothermia, and feeding difficulties, all of which necessitate intensive monitoring and care.
Low birth weight (<2500 g) was also significantly associated with admission (AOR = 3.07), reinforcing its established role in predicting neonatal complications such as sepsis, hypoglycemia, and respiratory instability.5,7,17,18 In Indonesia, low birth weight remains 1 of the contributors to neonatal mortality, as confirmed by findings from the study Analysis Determinants of Neonatal Death in Indonesia from the Indonesian Health Demographic Survey 2017. 17 A systematic review found that LBW neonates have a markedly higher risk of prolonged NICU stay and complications including sepsis, necrotizing enterocolitis, bronchopulmonary dysplasia, and retinopathy of prematurity. 18
An Apgar score at first-minute <7 had the strongest association with special or intensive care needs (AOR = 7.87), highlighting the clinical utility of this immediate postnatal assessment tool in guiding resuscitation and care. The first-minute Apgar score reflects the newborn’s immediate physiological condition and transition to extrauterine life and plays a critical role in guiding early clinical evaluation, monitoring, and decisions regarding admission to higher levels of neonatal care. 19 Consistent evidence from studies conducted in Asia and Africa has also demonstrated that low Apgar scores are significantly associated with increased risk of NICU admission and adverse neonatal outcomes.4,20
In contrast, the fifth-minute Apgar score reflects the infant’s response to initial stabilization and resuscitative interventions and is more strongly associated with longer-term neonatal outcomes, including morbidity and mortality, rather than the immediate decision for admission.4,19 While the fifth-minute Apgar score remains an important prognostic indicator, the present findings demonstrate that the first-minute Apgar score is more directly associated with the need for immediate specialized neonatal care. 19
Interestingly, maternal age, parity, mode of delivery, and mode of hospital arrival did not show significant associations with neonatal care level after adjustment. Although other studies have linked advanced maternal age and emergency referrals with adverse outcomes, these effects may be indirectly mediated by more immediate neonatal indicators like prematurity or asphyxia.7,21
These findings emphasize the importance of strengthening both the coverage and quality of ANC. Early attendance at ANC visits enables the timely identification of high-risk pregnancies and allows for better preparedness regarding neonatal care requirements. Furthermore, integrating simple clinical indicators such as Apgar score and birth weight into delivery room decision-making processes can enhance triage efficiency, especially in hospitals with limited neonatal bed availability.
The present findings also support the need for developing and validating localized neonatal risk scoring systems to guide triage and referral decisions within Indonesian referral hospitals. Implementing such tools could contribute to reducing preventable neonatal deaths in resource-limited healthcare environments.
This study has several limitations. First, the retrospective design limited control over the completeness and accuracy of recorded data, resulting in unavoidable missing or incomplete entries. Second, maternal clinical conditions and diagnoses during labor, particularly those occurring in the second stage of labor, were not consistently documented, despite their potential influence on neonatal outcomes. Third, although neonatal vital signs are routinely recorded in clinical practice, these parameters were not included in the analysis, which limited the assessment of early neonatal physiological adaptation. The exclusion of these potentially relevant variables may have introduced residual confounding and limited the comprehensiveness of the findings. Fourth, antenatal care (ANC) attendance was defined based on documented visits at RSUD Haji. Some women classified as having no ANC attendance at the study hospital may have received ANC at other healthcare facilities, such as primary health centers, private clinics, or other hospitals, which were not captured in the hospital medical records. This may have resulted in nondifferential misclassification bias and could underestimate the true utilization of ANC.
Finally, the single-center design and local setting may limit the generalizability of the findings to other healthcare settings or populations. Nevertheless, this study provides important baseline evidence on maternal and neonatal risk factors in a secondary referral hospital in Indonesia and may serve as a foundation for future multicenter studies or analyses using integrated healthcare databases.
Although the associations were statistically significant, the relatively wide confidence intervals, particularly for Apgar score at first minute <7 and preterm birth, indicate some degree of imprecision in the estimates, possibly due to the limited number of cases in these subgroups. These findings provide evidence-based insight for risk stratification in neonatal triage, particularly in resource-limited hospitals in Indonesia. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. 22
Conclusion
This study identified several key maternal and neonatal factors associated with the need for special or intensive neonatal care in a hospital setting. No antenatal care attendance at the study hospital, low birth weight, low first-minute Apgar score, and preterm birth showed significant associations with higher odds of neonatal admission. These findings underscore the importance of strengthening ANC services and enhancing early risk detection during pregnancy to reduce the need for intensive neonatal interventions. Improved prenatal monitoring and timely referral of high-risk pregnancies are essential to improving neonatal outcomes in resource-limited settings.
Footnotes
Acknowledgements
We are deeply grateful to Haji Provincial General Hospital of East Java, East Java, Indonesia for granting permission and facilitating the data collection for this study.
Ethical Considerations
Ethical approval was obtained from the Health Research Ethics Committee of Haji Provincial General Hospital of East Java, Indonesia (Approval No: 445/168/KOM.ETIK/2025). The requirement for informed consent was waived due to the retrospective nature of the study and the use of anonymized medical records.
Consent to Participate
The requirement for informed consent was waived because the study used secondary data from medical records with all patient identifiers removed to ensure confidentiality.
Author Contributions
All authors contributed equally to the conception, design, data collection, analysis, and writing of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.*