
Abstract
Objective. To evaluate the evidence regarding the association between iron deficiency anemia (IDA) and dental caries in children and adolescents. Methods. Searches were conducted in 4 international databases from the beginning of records until October 2023. Studies evaluating the association between IDA and dental caries in individuals aged 6 months to 18 years were included. Risk of bias was assessed using the Newcastle Ottawa Scale. Quantitative synthesis was performed using the inverse variance or Mantel-Haenzel method, depending on the type of outcome analyzed. Measures of association included odds ratios and mean differences, employing a random-effects model with a 95% confidence interval. Results. A total of 1161 studies were identified, of which 12 were selected for qualitative review and 9 for meta-analysis. A significant association was found between IDA and dental caries (odds ratio of 3.54; 95% CI: 2.54-4.94) and a higher rate of dental caries in the presence of IDA (mean difference of 1.96; 95% CI: 1.07-2.85). The certainty of evidence according to GRADE was rated as very low. Conclusions. Despite the limited certainty, the findings indicate a significant association between IDA and dental caries. It is prudent to interpret these results with caution, considering the methodological limitations of the studies. However, given the potential relevance of this association for public health, recommending oral health strategies, including preventive and corrective dental interventions, for anemia control programs underlines the importance of more rigorous future research to strengthen the certainty of the evidence and guide the implementation of these strategies.
Background
Dental caries is a prevalent chronic disease that affects both children and adults, significantly impacting overall health. 1 This condition tends to be progressive; late diagnosis and treatment can lead to local pain, bad breath, infections, tooth loss, and may even compromise organs beyond the oral cavity. 2 Globally, it is estimated that 2 billion people suffer from caries in permanent dentition, while 514 million children have caries in primary dentition, with higher frequencies observed in low and middle-income countries. 3 In the United States, the prevalence of dental caries (treated and untreated) among individuals aged 2 to 19 is 45.8%. 4
Dental caries not only affects oral well-being but can also be an indicator of systemic imbalances. Among systemic diseases, IDA stands out due to its prevalence and significant global impact, being considered one of the concurrent conditions of dental caries. 5 IDA can initially manifest in the oral cavity, reflecting complex interactions between oral and general health. IDA is associated with dental caries through various biological mechanisms. Evidence suggests that IDA can alter the function of the salivary glands, reducing saliva production and its functions of cleaning, lubrication, and remineralization, thereby increasing the risk of dental caries. 6 Additionally, some medications used to treat anemia, such as iron supplements, may have side effects that affect oral health and salivary function. This dynamic underscores the importance of studying how specific systemic conditions like IDA contribute to oral pathology, emphasizing the relevance of our research to better understand these links. Although studies have been conducted to evaluate the association between these 2 conditions, the findings to date are inconclusive.7,8
Therefore, the aim of this study was to conduct a systematic review and meta-analysis of the available evidence to determine whether iron deficiency anemia is associated with dental caries in children and adolescents. Our results could assist healthcare professionals and policymakers in identifying individuals at risk and implementing interventions to optimize outcomes in the battle against anemia and dental caries.
Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 9 as detailed in Supplemental Table S1. The protocol is registered on the PROSPERO database (registration code: CRD42020197010).
The PECO components of the question were as follows:
P: children aged 6 months to 18 years
E: iron deficiency anemia
C: No iron deficiency anemia condition
O: Dental caries
Eligibility Criteria
Inclusion and exclusion criteria were established using the PECO method, focusing on comparative studies that evaluated the association between IDA and dental caries in individuals aged 6 months to 18 years. This age range was chosen for its importance in critical periods of dental development and general health. Studies specifically assessing IDA as a factor associated with dental caries were included, presenting data on the presence or absence of caries, measured numerically (eg, dmft index) or categorically, in both exposed (individuals with IDA) and unexposed groups. Studies were also considered that evaluated the reverse relationship (dental caries as a factor influencing anemia) and provided useful data that could be reinterpreted due to the univariate property of measures like odds ratios. No restrictions were applied for language, publication date, follow-up duration, or sample size. Exclusion criteria covered review studies, conference abstracts, case reports, and those conducted on animals or ex vivo samples.
Search Strategy
A systematic search of articles published up to October 2023 was conducted using Medline (accessed through PubMed), Scopus, Cochrane Library (CENTRAL), and Web of Science (WoS). Search terms related to “dental caries,” “anemia,” and “iron deficiency” were employed. The search strategy for each database is specified in Table 1. Additionally, the references of included studies were assessed to identify potential studies not located in the databases.
Search Strategy for Each Search Engine.

Study Selection
To eliminate duplicate publications, search results were exported to EndNote X9 (Thomson Reuters, Philadelphia, PA, USA). Before commencing the selection process, 2 authors (RAI and WNG) conducted a pilot of the inclusion criteria to reduce errors in the selection process, using the first 100 studies. Subsequently, these authors independently examined titles or abstracts of retrieved publications to identify studies that potentially met the inclusion criteria. This was accomplished using the Rayyan application (https://rayyan.qcri.org/), enabling the classification of publications as included, excluded, or potentially included. Conflicts regarding the inclusion of any publication were resolved through discussion between reviewers. All studies included based on titles and abstracts progressed to the full-text assessment phase. These studies were independently assessed by the same review team members, and conflicts were resolved through discussion between reviewers.
Data Extraction
Two reviewers (WC and PJC) independently performed relevant data extraction. They extracted the following data into a matrix, including study characteristics (author, publication year, country, study design, exposure measure, outcome), participant characteristics (age, gender, number of participants), and relative measures (raw and adjusted) with their confidence intervals obtained from the association of anemia and caries. Any disagreements were resolved through discussion with a third author (WHC).
Study Quality and Certainty of Evidence
Two reviewers (RAI and WHC) independently assessed the risk of bias of included studies using the Newcastle Ottawa tool for case-control studies and the adapted version for cross-sectional studies. 10 This tool consists of 3 domains: selection, comparability, and exposure or outcome. For case-control studies, the selection domain allows for up to 4 stars, comparability up to 2 stars, and exposure or outcome up to 3 stars. In the case of the adapted tool for cross-sectional studies, up to 5 stars can be assigned in the selection domain, 2 in comparability, and 3 in exposure or outcome. Higher scores indicate higher study quality. Stars are awarded based on the answer to each element’s question. Responses are graded with 1 or 2 stars, signifying a lower risk of bias for the assessed component. In cases of disagreement, a third reviewer acted as an arbitrator (PJC).
To assess the certainty of the evidence for each outcome, we used The Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology, which evaluates the study design, risk of bias, inconsistency, indirectness, imprecision, and other factors as a publication bias.
Statistical Analysis
Data Synthesis and Analysis
Review Manager software version 5.4.1 was employed for data compilation and analysis of each study, using measures such as odds ratios and mean differences in random-effects models, providing 95% confidence intervals. Due to observed heterogeneity among studies, random-effects models were applied, including inverse variance and Mantel-Haenszel methods for data analysis. To address heterogeneity beyond the I2 test and P-value, subgroup analyses were conducted by age range and according to indicators used for IDA diagnosis, such as hemoglobin alone or in combination with ferritin and/or mean corpuscular volume (MCV), by caries severity, and by study design. Additionally, heterogeneity was evaluated using the I2 statistic, considering that heterogeneity might not be significant when I2 was below 40%. 11 Fixed-effects sensitivity analysis and another for studies with a risk of bias assessment of 7 or more stars on the Newcastle-Ottawa Scale were performed. It is noteworthy that a publication bias assessment was not conducted due to the limited number of studies included in each analysis. Primary outcomes focused on the presence or absence of caries, measured numerically or categorically, in groups exposed and unexposed to IDA according to their study design. Secondary outcomes included the mentioned subgroup analyses and proposed sensitivity analyses.
Results
Search Results
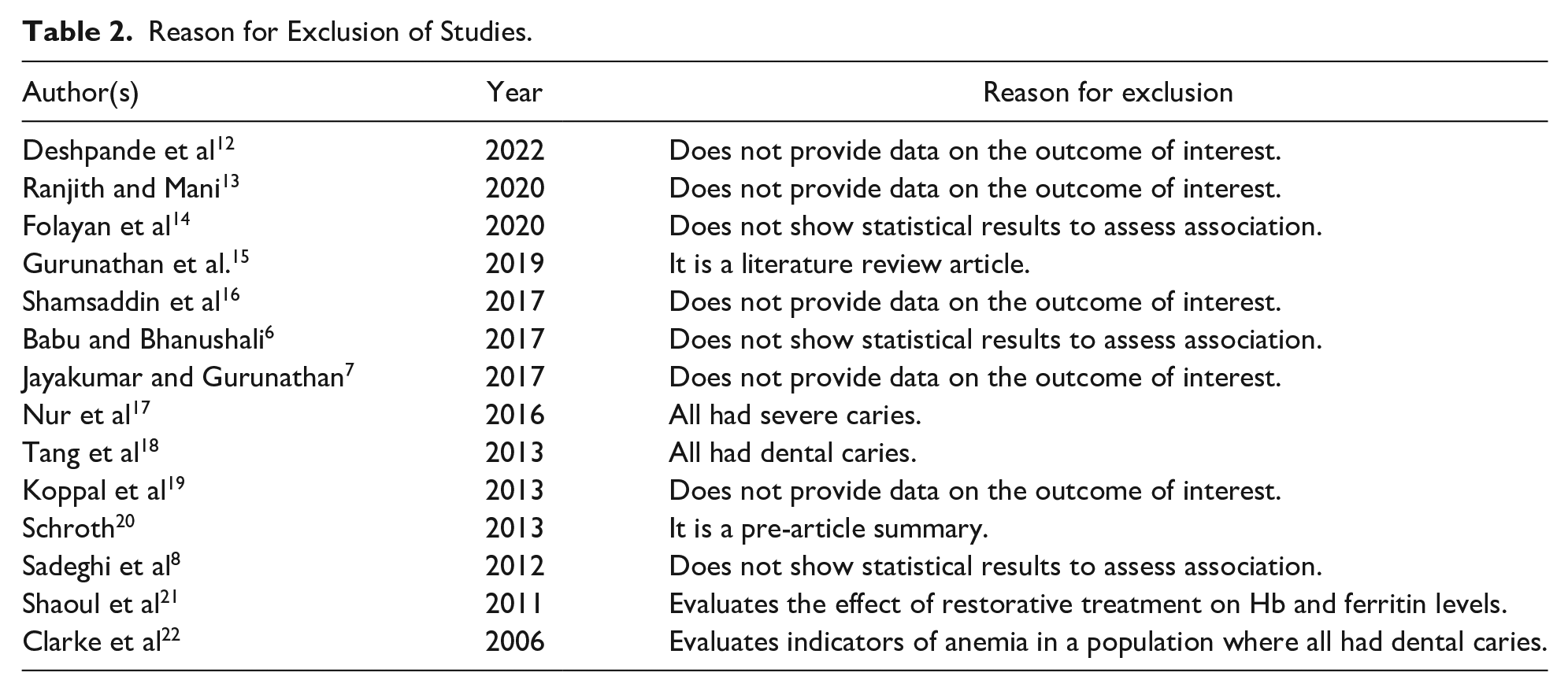
A comprehensive search, both electronic and manual, resulted in a total of 1161 records. From these, an initial search yielded 825 records, of which 70 were duplicates and were removed, leaving 755 records for examination. After evaluating titles and abstracts, 20 full-text articles were selected as potentially eligible. Subsequently, an updated search identified an additional 406 records for exploration. After reviewing the titles and abstracts of these, 400 records were excluded. Finally, of the 26 studies initially selected, 12 met the inclusion criteria and were included in the analysis (Figure 1). The reasons for the exclusion of the remaining studies are detailed in Table 2.

PRISMA flow diagram of the study selection process.
Reason for Exclusion of Studies.
Characteristics of Included Studies
In total, 9 studies with a cross-sectional design23-31 and 3 case-control studies32-34 were included. Regarding the setting, articles originated from 8 different locations: Canada,33,34 China,23,27,31 Egypt, 24 Peru, 25 Brazil, 26 Saudi Arabia, 28 India,29,32 and the USA. 30 One notable characteristic is the age of the patients, with 10 studies including children under 6 years,23,24,27-34 one study including children from 6 to 12 years, 25 and one study including adolescents aged 17 to 18. 26 Concerning caries data, 8 studies23-28,33,34 used validated WHO criteria DMFT/dmft (D: decayed, M: missing due to caries, F: filled; in permanent and primary dentition, respectively), while 4 studies did not specify the criteria used for recording caries. Various parameters were reported for the assessment of IDA: hemoglobin, serum ferritin, and mean corpuscular volume (MCV). IDA is diagnosed by abnormal values in 2 of 3 blood analysis parameters in the study by Ji et al, 23 Mohamed et al, 24 Bansal et al, 29 Jha et al, 32 Deane et al 33 and Schroth et al 34 Regarding result extraction, 7 studies reported data to calculate the crude OR, and 3 studies reported their means and standard deviations. Therefore, for the meta-analysis, studies were considered where crude ORs were obtained, and studies reporting the mean value of dental caries in the exposure groups with their respective standard deviations (Table 3).
Characteristics of Included Studies.

Abbreviation: NR, no record.
OR: odds ratio
MD: mean difference of DMFT/dmft index
Months.
Adjusted measures.
Risk of Bias Analysis of Studies
Risk of bias analysis was applied to 3 case-control studies using the Newcastle-Ottawa Scale (NOS) and 9 studies using the modified NOS for cross-sectional studies. There were differences in the risk of bias between the study designs. Included cross-sectional studies exhibited significant risk of bias, mainly in the selection domain, specifically in the “representativeness of the sample” and “sample size” items. Case-control studies also presented a risk of bias, primarily in the selection domain, specifically in the “representativeness of the cases” item. This situation hinders the proper extrapolation of results, which should be considered when interpreting the findings of this review (Figure 2). However, there was no difference in the direction of effect between the overall findings and when only the low-risk-of-bias studies were evaluated (Figure 3).

Risk of bias.
Forest plot of sensitivity analysis with studies scoring 7 or more stars on the Newcastle-Ottawa Scale for risk of bias assessment.
Quantitative Analysis: Results Synthesis
Nine of the 12 included studies23-25,27-29,31,33,34 provided data for the meta-analysis. The studies by Jha et al, 32 Prado et al 26 and Ramos-Gomez et al, 30 were not included in the quantitative analysis. The first 2 were excluded because they reported adjusted effect measures of the inverse of the association (dental caries as an exposure) or different measures of effect (eg, mean ratio) and did not provide absolute data for each exposed group. The last study reported an adjusted measure by age, which precluded one of the main subgroup analyses by age. However, this study reported results similar to our systematic review in both direction and magnitude.
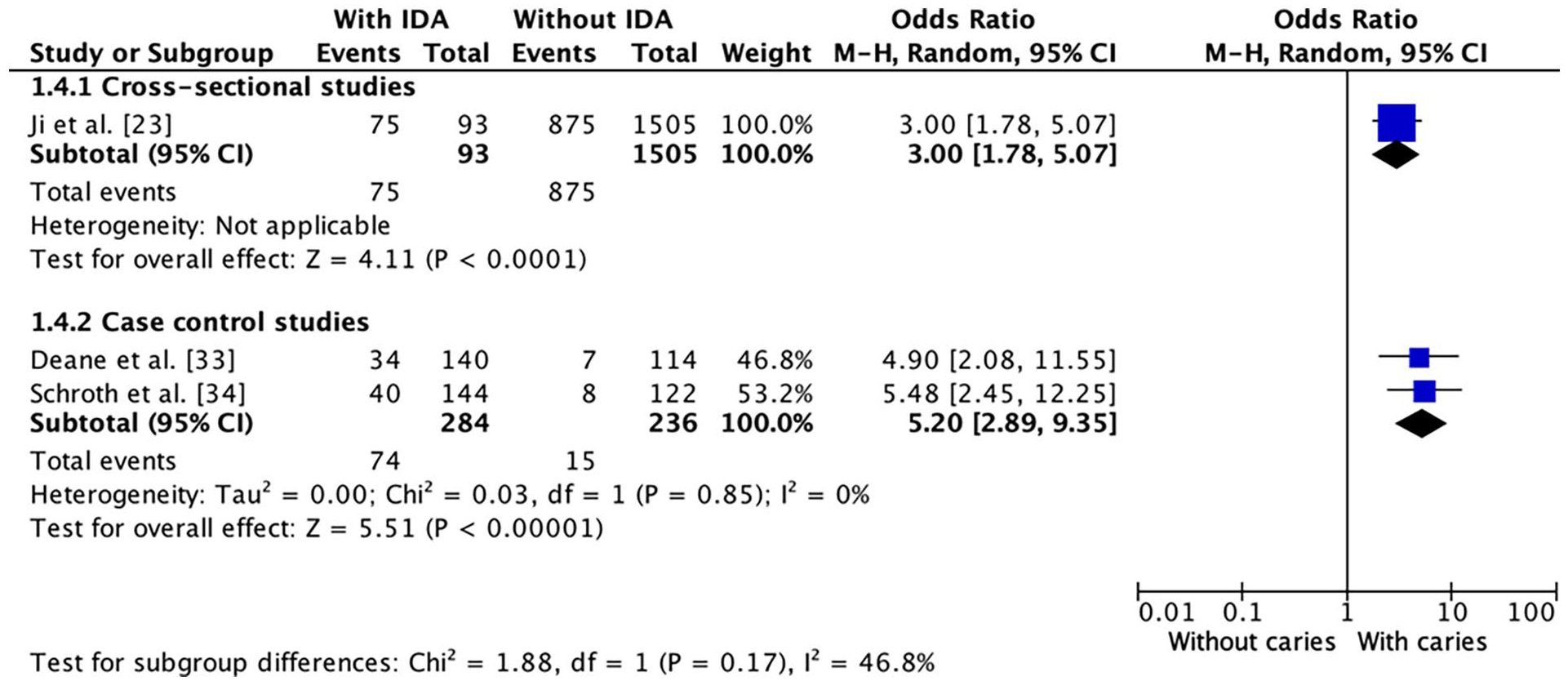
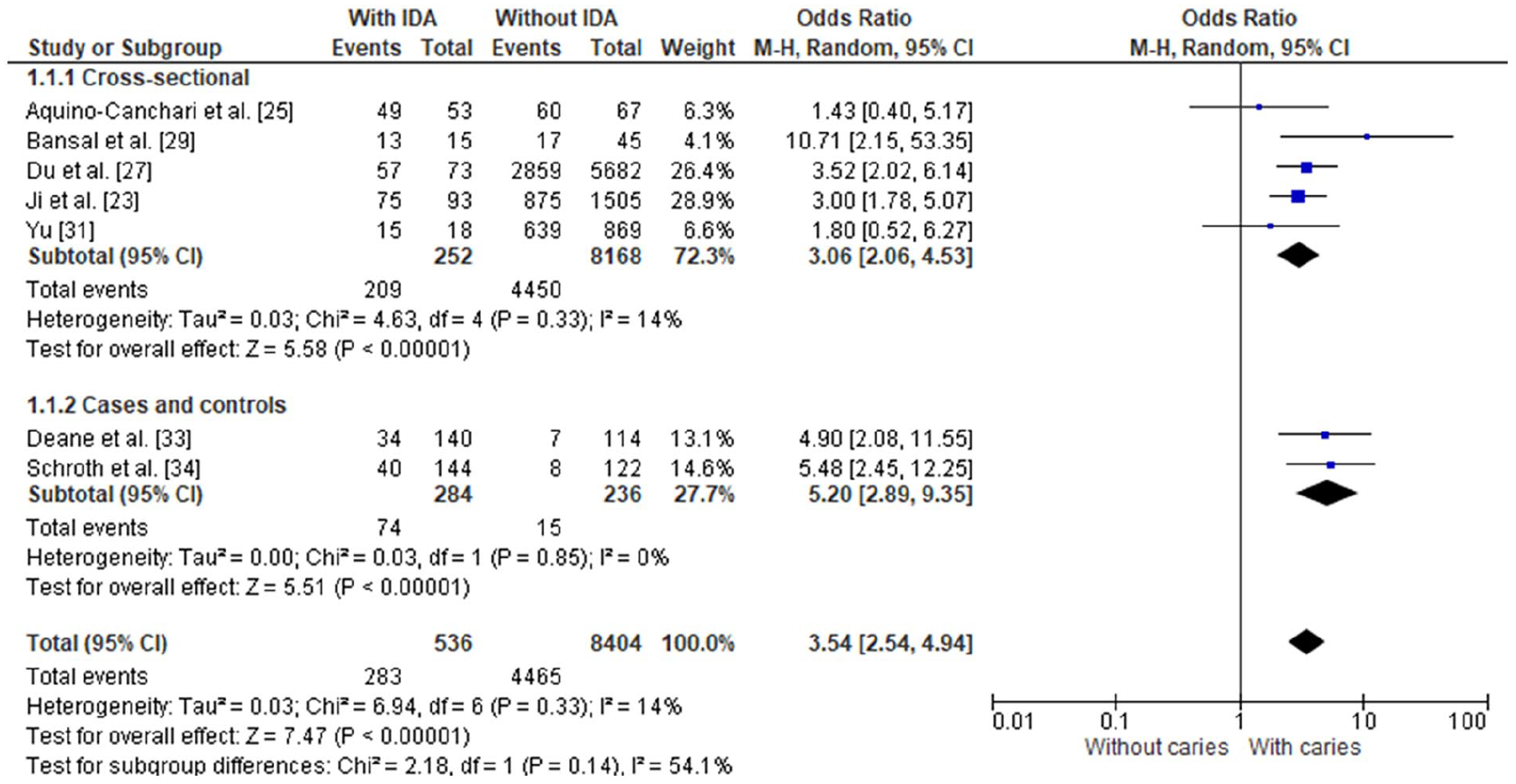
The meta-analysis suggests significantly higher odds of dental caries in the IDA group compared to the non-IDA group in both cross-sectional studies (OR = 3.06, 95% CI 2.06-4.53, P = .33) and case-control studies (OR = 5.20, 95% CI 2.89-9.35, P = .85), as shown in Figure 4. No statistical significant heterogeneity was detected among the study designs (I2 = 54.1%, P = .14, Figure 4), and a similar result was obtained in the sensitivity analysis using a fixed model (Figure 5).
Forest plot comparing dental caries in individuals with and without IDA by study design.

Forest plot of sensitivity analysis with fixed-effects model comparing dental caries in individuals with and without IDA.
Only the cross-sectional studies provided data for dental caries evaluated with the dmft index, suggesting higher dmft index levels in the anemic group compared to their non-anemic control group (MD = 1.96, 95% CI 1.07-2.85, P = .002), as represented in Figure 6.

Forest plot comparing dmft index in individuals with and without IDA (only cross-sectional studies).
Subgroup Analysis
We identified a higher effect size in the population under 6 years of age in both cross-sectional (OR = 3.27; 95% CI 2.26-4.75) and case-control studies (OR = 5.20; 95% CI 2.89 – 9.35) compared with those older than 6 years (evaluated only in cross-sectional studies). The association shows a statistically significant difference for the exposure and outcome in younger children. In contrast, the association is not statistically significant in the older group (OR = 1.43; 95% CI: 0.40, 5.17), with only 1 study contributing to this estimate (Figure 7).

Forest plot of subgroup analysis by age range.
When stratified by the diagnostic method of IDA, some cross-sectional studies used only the hemoglobin method, while others used a combination of hemoglobin, serum ferritin, and/or mean corpuscular volume (MCV). However, case-control studies solely utilized hemoglobin. There is a noted difference in effects when studies are evaluated using hemoglobin only versus a combination of hemoglobin and other methods, with a lower magnitude of effect seen in the hemoglobin-only method. Nevertheless, both estimates are statistically significant. In cross-sectional studies assessing IDA through hemoglobin, the odds of dental caries increase in the exposure group (OR = 2.74, 95% CI 1.62-4.61), as well as in those assessing IDA using both hemoglobin and serum ferritin and/or MCV (OR = 4.48, 95% CI 1.41-14.26) (Figure 8).

Forest plot of subgroup analysis by diagnostic indicators.
Regarding the severity of caries, significant associations were observed across all subgroup categories. Cross-sectional studies provided estimates for both severe and non-severe early childhood caries, while case-control studies reported only on severe early childhood caries. A higher effect is observed in the severe group, although it is based solely on the estimate of one study. In the cross-sectional studies, the exposure increases the odds of severe early childhood caries (OR = 10.71, 95% CI 2.15-53.35) and also of non-severe early childhood caries (OR = 3.08, 95% CI: 2.13-4.43) (Figure 9).

Forest plot of subgroup analysis by caries severity.
Certainty of Evidence
We evaluated the certainty of the evidence based on the main results, divided by study design. For all outcomes, we identified a very low level of certainty, particularly due to concerns in the domains of risk of bias, heterogeneity, and imprecision. Given our very low confidence in the results, the evidence remains uncertain for all outcomes. However, out results suggest that the exposure to IDA might increase the incidence of dental caries by 241 more cases (range: 167-299 more) per 1000 individuals in cross-sectional studies and by 4 more events (range: 2-8 more) per 1000 individuals in case-control studies. Additionally, IDA exposure might increase the dmft index by 1.96 points (range: 1.07-2.85 more; Table 4).
Summary of Finding.
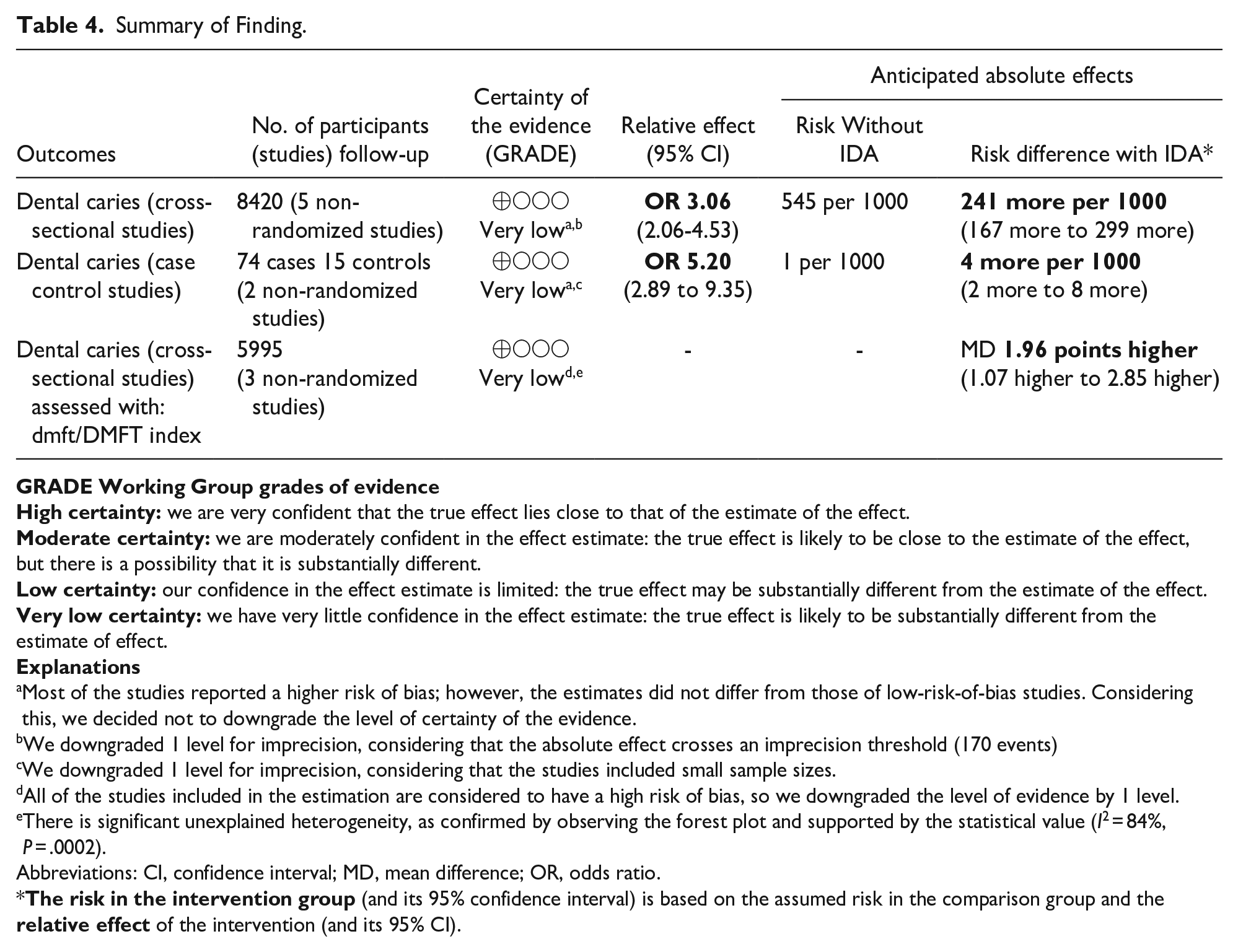
Most of the studies reported a higher risk of bias; however, the estimates did not differ from those of low-risk-of-bias studies. Considering this, we decided not to downgrade the level of certainty of the evidence.
We downgraded 1 level for imprecision, considering that the absolute effect crosses an imprecision threshold (170 events)
We downgraded 1 level for imprecision, considering that the studies included small sample sizes.
All of the studies included in the estimation are considered to have a high risk of bias, so we downgraded the level of evidence by 1 level.
There is significant unexplained heterogeneity, as confirmed by observing the forest plot and supported by the statistical value (I2 = 84%, P = .0002).
Abbreviations: CI, confidence interval; MD, mean difference; OR, odds ratio.
Discussion
The aim of this systematic review and meta-analysis was to determine the association between IDA and dental caries. The results revealed significantly higher odds (OR 3.54) of dental caries in children affected by IDA compared to those without IDA. Of the studies included in the meta-analysis, 5 studies23,27,29,33,34 reported that children with IDA were at a higher risk of dental caries, while 2 studies found no association between IDA and dental caries.25,31
This reported association could be attributed to the fact that IDA may alter salivary gland function, reducing salivary secretion and its sweeping, lubricating, and remineralizing functions, increasing the risk of dental caries. 6 However, it should be noted that data from the studies by Aquino-Canchari et al 25 and Yu 31 did not show a significant association between the 2 variables. The study by Aquino-Canchari et al 25 was conducted in a native community, which could be linked to a population with a low socioeconomic status; according to Schroth et al 34 and Deane et al 33 socioeconomic status is one of the factors that can mask the association. On the other hand, the study by Yu 31 shows different hemoglobin categories (<10.9, 11.0-11.9, 12.0-12.9, and > 13.0) without finding a significant difference between hemoglobin groups and the presence of dental caries; this aligns with our quantitative analysis, which was conducted by collecting data to group participants with IDA and without IDA. However, it should be clarified that this study reported that the anemia group (Hb <10.9) had the highest rate of dental caries.
Moreover, within the evidence supporting the association between IDA and dental caries,23,27,29,33,34 2 cross-sectional studies and 2 case-control studies were found, all of which concurred in reporting a significant association. These studies reported a large effect size; however, we must consider that IDA and dental caries are multifactorial diseases that can be influenced by social determinants of health, such as social and economic conditions, education level, among others.35,36 Therefore, it is necessary to take into account possible confounding factors to determine a causal relationship; since such factors can mask the true association between IDA and dental caries. For this reason, the economic condition could compromise the validity of these studies. However, Schroth et al 34 and Deane et al 33 reported a significant association in both their bivariate and multivariate analyses, in which they considered economic status as a confounding factor. In this multivariate analysis, significance was maintained, revealing in Schroth et al 34 study an OR of 6.58 with a 95% confidence interval between 1.01 and 2.76 and a P-value < .001; similarly, Deane et al 33 study showed a regression coefficient of 16.84 with a 95% confidence interval between 11.04 and 22.65 and a P-value < .001.
Similarly, our study conducted a meta-analysis of the correlation between IDA and dental caries, including 3 studies, which reported a higher mean value of the caries indicator in the iron-deficient group, resulting in a statistically significant relationship. These results align with the reported effects through odds ratios and reinforce the current evidence on the possible association between the variables of interest in this study.
Regarding studies not included in the meta-analysis, the study by Ramos-Gomez et al 30 conducted in 146 children under 6 years did not report a significant association between iron deficiency anemia and dental caries; meanwhile, the study by Prado et al 26 conducted in 363 adolescents aged 17 to 18 years and the study by Jha et al 32 conducted in 266 children under 6 years showed a significant relationship between IDA and dental caries.
The subgroup and sensitivity analysis indicate an association between IDA and dental caries, with significant variations based on age. The observed association in children under 6 years and the absence of the same in children aged 6 to 12 years can be explained by various factors. During the early years of life, iron deficiency can directly impact dental development due to being a critical phase of growth and mineralization. Children under 6 years, in full development, depend on nutrition for oral health, and iron deficiency can compromise dental enamel, increasing susceptibility to caries. 24 In contrast, older children may have better oral hygiene habits and access to preventive measures, reducing the impact of iron deficiency anemia. 14 Additionally, differences in diet and sugar exposure between ages could influence the prevalence of caries, regardless of iron status. 4 It is important to highlight that a single study contributed to the analysis in children older than 6 years. On the other hand, it was noted that those diagnosed with hemoglobin plus serum ferritin parameters and/or mean corpuscular volume, as well as those with severe early childhood caries, showed a stronger association with IDA compared to those diagnosed with hemoglobin alone and those with early childhood caries, underscoring the importance of accurately defining IDA and understanding that its presence at an early age can affect oral health, predisposing to greater severity of caries due to changes in saliva and oral microbiota. 6 Sensitivity evaluations, using fixed-effect models and including studies with a high score on the Newcastle-Ottawa scale, confirmed the consistency of the main findings.
Despite the appropriate methodology employed, our study presented the following limitations. First, the inclusion of cross-sectional studies limits the establishment of a cause-and-effect relationship. Furthermore, interpretation is limited by the potential confounding effect of other established risk factors such as economic status, which could not be controlled in all studies. An adaptation of the Newcastle-Ottawa Scale (NOS) for cross-sectional studies was used to evaluate risk of bias, though this is not standardized by NOS and may be considered a limitation. Second, studies varied in sample size, age, parameters used to assess and define IDA, and the index used to report dental caries. Finally, the lack of longitudinal studies that could better determine the causal relationship between dental caries and IDA.
Recommendations
The relevance of this systematic review is that IDA and dental caries could be interrelated; therefore, we propose the following actions:
Awareness and Education
Our results indicate that it is crucial to increase awareness among health professionals who care for children and adolescents about the impact of IDA on oral health. It is necessary to implement specific educational programs aimed at these professionals, emphasizing the importance of comprehensive care that considers both systemic health and the oral health of patients.
Preventive Interventions and Integration Into Health Programs
It should be considered that preventive and timely dental intervention could prevent further severity of the condition and facilitate its treatment. A person with untreated carious processes could experience pain, resulting in nutritional deficiencies due to difficulty in chewing. Due to these reasons, the integration of preventive care and dental interventions into national anemia control programs is crucial. Likewise, it is imperative to reassess existing multisectoral plans, leveraging the comprehensive framework of Peru’s multisectoral anemia control plan, 37 and the Multisectoral Plan for the Prevention and Reduction of Maternal and Child Anemia in Peru, period 2024-2030, 38 as a case example.
Specific Dental Interventions
Despite the fact that oral evaluation is included in the guidelines for the monitoring and development of children from the first check-up, which establishes that every child must be examined by a dentist or pediatric dentist specialist before the age of one, 39 specific dental interventions should be included as a strategic activity to be conducted by the Ministry of Health within the broader strategy to combat anemia on a national scale.
We advocate for the inclusion of these dental interventions, emphasizing a comprehensive approach that not only targets anemia but also addresses related oral conditions. This holistic strategy holds the potential to significantly enhance the overall health status of the population, concurrently tackling both anemia and associated oral health issues.
Conclusions
Despite the uncertainty in the certainty of the evidence, the results suggest a significant association between IDA and dental caries. Prudent interpretation of these findings is essential, considering the methodological limitations intrinsic to observational designs, which are prone to biases. However, the potential relevance of this association to public health underscores the need to consider oral health strategies, including preventive and corrective dental interventions, within anemia control programs. The importance of future rigorous research is emphasized to strengthen the certainty of the evidence and effectively guide the implementation of these strategies.
List of Abbreviations
IDA: Iron Deficiency Anemia
PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
PROSPERO: International Prospective Register of Systematic Reviews
PECO: Population, Exposure, Comparator, Outcome
DMFT/dmft: Decayed, Missing, Filled Teeth (permanent and primary dentition)
WHO: World Health Organization
NOS: Newcastle Ottawa Scale
CI: Confidence Interval
OR: Odds Ratio
MCV: Mean Corpuscular Volume
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241273130 – Supplemental material for Iron Deficiency Anemia and Dental Caries: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-gph-10.1177_2333794X241273130 for Iron Deficiency Anemia and Dental Caries: A Systematic Review and Meta-Analysis by Rubén Aguirre-Ipenza, Wendy Nieto-Gutiérrez, Winnie Contreras, Pavel J. Contreras and Walter H. Curioso in Global Pediatric Health
Footnotes
Acknowledgements
We sincerely thank Cusi Ferradas and Michael Sciaudone for their invaluable support and suggestions during the review of this manuscript.
Availability of Data and Materials
The dataset supporting the conclusions of this article is included within the article. However, additional information can be requested from the corresponding author upon reasonable inquiry.
Contributions
RAI conceived the study. All authors contributed to the study design. RAI and WNG planned, supervised, and validated the work. WNG and RAI performed the literature search and eliminated duplicate records. RAI, WNG, WC, and PJC selected and extracted data from the included studies. RAI and WHC assessed the quality of the studies. RAI, WNG, WC, and PJC analyzed the results and wrote the manuscript. RAI created tables and figures. RAI, WNG, WC, PJC, and WHC critically reviewed, approved, and assumed responsibility for the content of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from Universidad Continental S.A.C.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.