
Abstract
Background. Autoimmune hepatitis (AIH) is increasingly seen in children worldwide and it is more severe in children compared to adults. This study highlights the biochemical and clinical aspect, treatment given and outcome of the disease including pediatric liver transplantation. Study. Retrospective review (2012-2022) was done in Shifa International Hospital, Islamabad. Patients under 18 years diagnosed with AIH were included. Data related to age, gender, clinical features, laboratory investigations including liver function test, liver biopsy findings and imaging modalities were included. Results. Fifteen patients were included 7 (47%) were males and 8 (53%) females. AIH type 1 was the most common type seen in 7 (46%), AIH type 2 in 5 (33%) and seronegative in 3 (20%). Jaundice was the most common symptom. Liver biopsy showed findings characteristic of AIH. Liver transplant performed in 3 patients. Conclusion. The study highlights the varied clinical presentation of AIH in Pakistani children.
Introduction
Autoimmune hepatitis (AIH) is a progressive inflammatory liver disorder. 1 It is more common in age groups between 10 and 30 years with a female predominance. Family history is positive in 40% of patients and 20% have association with other autoimmune diseases like thyroiditis, celiac disease, insulin dependent diabetes mellitus, vitiligo and inflammatory bowel disease. 2 The incidence has increased between 1990 and 2000 by 6-fold. The recently reported incidence is 0.23 per 100 000 children. In US the prevalence is 3 per 100 000 and 9.9 per 100 000 in Canadian children. 3
AIH is more severe in children than adults. 4 There are 2 main types, Type 1 is positive for antinuclear antibody (ANA) and anti-smooth muscle antibody (SMA). Type 2 is positive for anti-liver kidney microsomal (LKM) or anti liver cytosol antibody. Another type is seronegative characterized by absence of antibodies but has typical histological findings. 5 Type 1 is more common than Type 2. Type 2 is common in males and is associated with raised GGT. 6
Like any other autoimmune disease, pathogenesis of AIH include immunization to liver targets. The environmental triggers result in thymic failure, and auto reactive CD4 and CD8 T cell break the self-tolerance of hepatic auto antigens. The auto antigen specific natural and inducible T cells are unable to prevent auto reactivity. This results in production of antibodies against nuclear proteins (ANA), smooth muscle (SMA). Hepatotropic viral infections, drugs for example methyldopa, infliximab indomethacin, and herbal medicine are possible extrinsic factors. Human Leukocyte Antigen (HLA) alleles have been linked with progression and severity of AIH. 7 Class II HLA and Class I HLA alleles present the peptide auto antigens to autoreactive T cells receptors on CD4 T helper cell and CD8 cytotoxic T lymphocytes. Alteration in gut microbiome and pathobionts can also contribute to triggering immune system resulting in AIH complex. 8
International Autoimmune Hepatitis Group (IAIHG) has designed a scoring system which is mainly for comparative and research purposes. The sum of the scores points to definite or probable AIH. The scoring system include age of patient, gender, antibody titers, IgG level, liver histological finding and exclusion of viral hepatitis. The typical histological features on liver biopsy include interface hepatitis, portal lymphoplasmacytic infiltrate, emperipolesis, and rosette formation. The latter two features are significantly associated with autoimmune process. The presence of hyaline droplets in Kupffer cells is specific for AIH and help in distinguishing it from other forms of hepatitis. It is associated with a 2-fold increase in IgG level. 9
AIH can have varied presentation ranging from asymptomatic to acute liver failure. The disease can progress to advance hepatic fibrosis and cirrhosis. Patients can also present as vague symptoms like anorexia, malaise, joint pain, abdominal pain. 10 Steroids are used as first line treatment and azathioprine is the drug of choice regarding maintenance of remission. 11 AIH respond well to immunosuppressive therapy. 12 Normalization of biochemical, clinical, histological, and immune parameters is considered as disease remission. When patient remains in complete and sustained remission, the treatment is continued for a minimum of 2 years. Follow up is continued lifelong despite treatment discontinuation and normalization of diagnostic parameters. After discontinuation of therapy AST, ALT, Ig G, and autoantibodies should be regularly measured 3 monthly. 13 If the patient develops advanced liver disease despite immunosuppressive therapy, or present as fulminant liver failure then liver transplantation is required.
In Pakistan scarce data is available for AIH in children. Although the prevalence of disease is less in our part of world but the clinicians should have high index of suspicion when other common cause of acute and chronic liver disease have been ruled out. This study highlights the biochemical and clinical aspect of autoimmune Liver disease in Pakistani children. It also emphasizes on the treatment and outcome of the disease including liver transplantation.
Method
This retrospective review from 2012 to 2022 was done in Pediatric OPD of Shifa Falahee community health center and pediatric gastroenterology division of Shifa International Hospital, Islamabad. Two patients were referred from Military Hospital Rawalpindi. All patients under 18 years diagnosed with autoimmune hepatitis on the basis of history, laboratory investigation was included in the study. Detailed performa was filled related to age, gender, anthropometry, clinical features, laboratory investigations including liver function test, liver biopsy findings and imaging modalities used like Ultrasound, CT abdomen, MRCP.
Autoimmune antibodies profile (ANA, ASMA, Anti LKM) were noted. Further classification of AIH was done on the basis on antibodies profile. Treatment given and liver transplant details and outcomes were noted. Review of medical records was done to check for other associated diseases with autoimmune hepatitis like celiac disease, inflammatory bowel disease and overlap syndrome.
Statistical Analysis
Data was entered and analyzed on SPSS version 23. Continuous variables are described as mean and standard deviation and categorical variables as number and percentage, respectively. Chi-square was applied to study the significance of associations. A P value of .05 was taken as significant. Written informed consent was taken from parents. Institutional ethic and review board approval was taken (IRB no 068-23).
Results
The study includes 15 patients, of these 7 (47%) were males and 8 (53%) females (P .47). Mean age of our study cohort was 10 ± 4.5 years. The youngest child of AIH-2 was of 2 years 6 months. Three patients were under 5 years of age. Mean weight was 31 ± 18 kg, mean height was 122 ± 27 cm.
AIH type 1 was the most common type seen in 7 (46%) patients, followed by AIH type 2 in 5 (33%) and Seronegative was seen in 3 (20%). Consanguinity was reported in 4 (26.6%) patients, one patient had family history of AIH, her aunt died of autoimmune hepatitis. The most reported symptoms and clinical signs as seen in our cohort of patients are reported in Table 1. Liver function tests are reported in Table 2. ANA was positive in 7 patients, Anti LKM in 5, SMA in 3 patients (P .003). Only 2 patients had IgG > 16 gm/dL.
Clinical Sign and Symptoms at Diagnosis in Children With AIH.
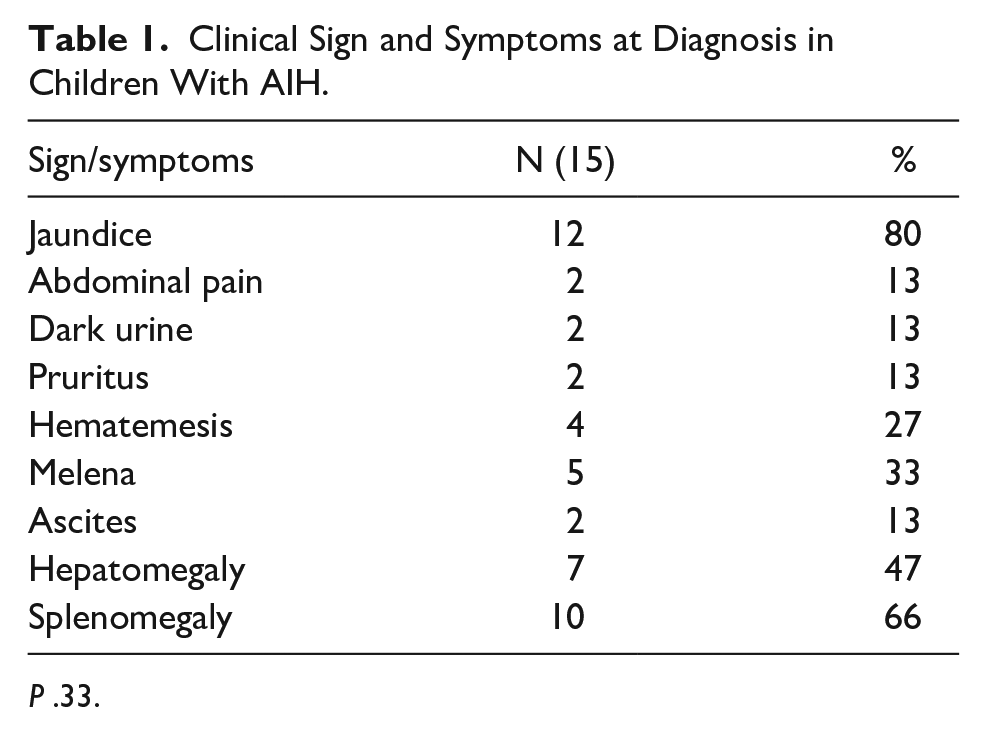
P .33.
Liver Function Test.

P .35.
Fulminant course of disease progressing rapidly within days and weeks was seen in 2 (13%) children. Others presented with chronic liver disease. Liver biopsy was performed in 12 patients. Marked interface hepatitis with plasma cell infiltrate was the most common finding. Giant cell formation and cirrhotic changes were other notable findings. Remaining patients were diagnosed on the basis of liver function tests, autoimmune antibodies profile and exclusion of other liver diseases in the absence of histology.
Steroids were used for all patients, 13 also received Azathioprine. Other immunosuppressant’s used in resistant cases were tacrolimus, Mycophenolate mofetil (MMF).
Two patients had underlying celiac disease in association with AIH. One patient had underlying inflammatory bowel disease, underwent colectomy also had type 1 AIH along with primary sclerosing cholangitis (PSC) with raised GGT and MRCP findings fulfilling the criteria for overlap syndrome.
Of the total cohort 8 patients are alive on treatment, 3 have died. Liver transplant performed in 3 patients. Two in Shifa International and one in Military Hospital. Two have survived and one passed away.
Liver Transplant Outcomes
Liver transplant was performed in 1 patient with AIH-1, 1 each with AIH- 2 and Seronegative AIH. Two male patients and 1 female underwent liver transplant. All patients had living donor liver transplant (LDLTx) from first degree relatives with compatible blood groups. No donor related complications or mortality was noted. Table 3 shows the description of AIH patients undergoing LDLTx in our cohort.
Description of AIH Patients Who Underwent Liver Transplantation.

Mean hospital stay was 14 ± 2 days. Immunosuppressant used post-transplant were Tacrolimus, cyclosporine, sirolimus along with steroids. Maximum survival noted so far is 8 years.
Acute complications observed were acute cellular rejection, perihepatic collection needing drainage. One patient that expired had a stormy immediate post-operative course having seizures and 2 episodes of asystole requiring cardiopulmonary resuscitation and inotropes but didn’t recover.
Discussion
The study shows slight female (53%) gender predilection. Literature supports the fact that AIH is 3 times more common in females than males. 14 It is estimated that 70% to 80% of patients with AIH are females. 15 Mean age of our study population was 10 years and 3 patients were under 5 years of age. Two of these were males with AIH-1 and 1 was female with AIH-2 she was the youngest patient 2.6 years. Majority of our patients (46%) had AIH-1, followed by AIH-2 in 33% patients. literature shows that AIH-1 is the most common type seen in majority of pediatric population presenting during adolescents while AIH-2 is reported in infancy. 16 Our patients with AIH-2 also presented at a younger age compared to AIH-1.
Clinically there are no differences between the types. Jaundice was the most common presentation reported in 80% of patients. Followed by abdominal pain, dark urine and pruritus.
Acute fulminant course of the disease was seen in 2 patients. Others had a more insidious chronic disease. Pediatric AIH has an aggressive course compared to adults and high index of suspicion should be maintained in children with liver diseases where other identifiable causes like Wilson disease, hepatitis B and C have been ruled out. 17
Celiac disease, autoimmune hemolytic anemia along with AIH-1 was an unusual presentation in a very young child. 18 One child had Ulcerative colitis (UC) had findings consistent with AIH- overlap syndrome. Literature shows a significant association of UC with overlap syndrome and resistant to steroid therapy. 19 Other known associated diseases with AIH include systemic lupus erythematosus (SLE), Autoimmune polyendocrinopathy syndrome (APECED), autoimmune thyroiditis, diabetes mellitus and lymphoproliferative disorders. 20
Although AIH is classified according to seropositivity for antibodies (ANA, SMA, LKM), Seronegative hepatitis is also reported in children. 21 Three patients had seronegative hepatitis (20%) diagnosed based on characteristic histopathological findings on liver biopsy. 22 This type of AIH has been reported in literature and shows a good response to steroids. 23
Our patients responded well to dual therapy with steroid and Azathioprine. AIH responds well to steroids and treatment should be started promptly. Second line agents approved for treating steroid resistant or relapses include tacrolimus, MMF, cyclosporine, Rituximab. 24 It is postulated that low vitamin D levels and oxidative stress contribute to the progression of AIH. 25
Liver transplant offers promising treatment for AIH patients not responding to medical therapy. 26 Three (20%) patients in our cohort underwent LDLTx, 2 have survived with a maximum survival of 8 years reported. More research is warranted to understand the disease pathology with link to the gut microbiome, similarly dietry modifications might also play an important role in management of AIH. 27 Limitations of our study include limited number of patients, a larger multicenter prospective study will give us more insight about AIH in children.
Conclusion
Autoimmune hepatitis is less studied in children in Pakistan. The study highlights the varied presentation of AIH and improved outcome with emergence of liver transplantation. However, early diagnosis and treatment are imperative to improve the outcome of children with AIH.
Footnotes
Author Contributions
SAK: manuscript drafting, data collection, analysis and review, NA: data collection, manuscript writing, MAF: data analysis, review and drafting, SH: data analysis, final drafting, MIM: data review, manuscript writing and drafting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.