
Abstract
Aim. This study aimed to assess the effectiveness of 3 interventions—skit video, pictorial, and sign language—in improving the oral hygiene of children with hearing impairment. Materials and Methods. Sixty children randomly divided into 3 groups: Skit video, Pictorial, and Sign language. The mean gingival and Oral Hygiene Index scores were recorded before and after interventions. A 1-way ANOVA was used for statistically significant difference between pre and post intervention scores. Results. A significant difference in mean oral hygiene and gingival index scores before and after interventions was found in Group A (P < .005). A statistically significant difference was also found between group A and B in inter group comparison of OHI and GI scores post intervention (P < .004). Conclusion. Skit video and pictorial intervention effectively improves oral health resulting in reduced mean oral hygiene and gingival scores.
Introduction
Due to communication obstacles, hearing-impaired children frequently struggle to comprehend and follow oral hygiene instructions. 1 Lack of access to dental services and misconception about oral health maintenance increases risk of developing dental diseases. 2 Children’s oral health is regarded as a crucial aspect of overall health and its significance cannot be understated. 3 Maintaining oral health and preventing oral diseases, including dental caries, gingivitis, and periodontitis, depends profoundly on good oral hygiene practices. 4 Communication difficulties may create difficulties for children with hearing impairment to comprehend oral hygiene procedures, making them particularly susceptible to oral health issues. 5 The obstacles of providing oral health care for young kids must be addressed with efficient educational interventions. Although sign language is frequently used in daily life, its efficacy as a tool for oral health education has not been examined in the literature to date. 6 It can be extremely difficult for people with special needs to maintain their oral health, which can have a substantial negative influence on an individual’s general wellness. 7 Therefore, in order to treat this particular population, 8 healthcare professionals need specialized knowledge. A hearing impairment is a reduction in the capacity to perceive sound, and it affects about 34 million children globally. 9 These children frequently experience difficulties with communication, schooling, and social integration in their daily lives, which may have a long-term negative impact on their health and wellbeing. 10 No exemption applies to oral health, as children with hearing loss have a higher risk of acquiring dental problems because of things like limited access to oral health information, low oral health literacy, and difficulty communicating with medical professionals. 11 A child’s whole growth and maturity can be impacted by hearing impairment, which can also have a substantial impact on speech and linguistic results, cognitive abilities, and academic progress. 12
Several studies have been conducted on the oral health status of individuals with special needs. According to a study by Zini et al, 13 individuals with special needs, including those with hearing impairment, are at higher risk of developing dental problems due to poor oral hygiene practices, limited access to dental care, and inadequate communication with dental professionals. Another study by Duker et al 14 highlights the need for dental professionals to receive specialized training in treating individuals with special needs to provide appropriate care. Regarding hearing impairment specifically, Olusanya et al conducted a systematic review of 49 studies and found that children with hearing impairment are at a higher risk of developing oral health problems, including dental caries, gingivitis, and periodontal disease, compared to their peers with normal hearing. 15 Additionally, the Joint Committee on Infant Hearing (2007) recommends that children with hearing impairment receive regular dental checkups to ensure early identification and treatment of oral health problems. 16 Despite the existing literature on effectiveness of educational interventions to improve oral hygiene and prevent dental problems in children with hearing impairment, there is a lack of evidence to support which method is more effective. Therefore, the present study aims to compare the effectiveness of 3 educational interventions skit video, pictures and sign language to improve oral hygiene status of children with hearing impairment.
Materials and Methods
Location and Duration of the Study
This non-blind randomized controlled trial was conducted in Karachi, Pakistan, from April to July 2023, on individuals with hearing impairment. Out of the 12 schools dedicated to individuals with special health care needs, 3 participated in the research and were treated as a single population block. Data were collected at different times corresponding to the allocation of groups in these schools.
Sample Size Calculation
In order to detect a difference as high as 10% between the groups, as was observed in previous literature, the required sample size was found to be 18 per group, with 95% confidence interval, design effect of 1, type I error of 5%, power of study at 80%, and 20% attrition in follow up was also considered. Hence, the number of children to be required was 18, which were further rounded off to 20 per group. 17
Trial Registration and CONSORT Checklist
The trial was registered on “clinicaltrials.gov” with NCT ID number NCT06089564 on 10/13/2023 in accordance with CONSORT guidelines. 18 The CONSORT checklist is given as Supplemental File 1.
Participant Selection Criteria
Eligible participant included children with hearing impairment and total hearing loss at birth, aged 7 to 20 years of both sexes, with a minimum of 20 teeth. The children in which dental plaque covered more thantwo-thirds of their tooth surface, had a plaque score of >1.0, and had fair to poor oral hygiene were included.
Participants who had previously participated in any oral health program within the previous 6 months, those with mild to moderate hearing loss, long-term antibiotic use, recent mouthwash use, ulcerative gingivitis, systemic diseases, extensive dental calculus, or uncooperative behavior were disqualified.
Participant Selection, Educational Intervention Allocation and Content
The 322 individuals with hearing-impairment aged between 7 and 20 were selected using a purposive sample technique. Ninety-two individuals were determined to be qualified for this trial. Sixty individuals were chosen at random from among 92 using a “random number table” to create a numbered list. The selected hearing impaired individuals were allocated into 3 oral health educational intervention groups, group A (skit video), group B (pictorial) and group C (Sign language/control) by using Sequentially Numbered Sealed Opaque Envelopes (SNOSE) as shown in Figure 1. The oral health educational intervention was written on paper, sealed in Sequentially Numbered Sealed Opaque Envelopes (SNOSE) and then shuffled to blind both the investigator and participants during selection process. Study participants picked a sealed envelope randomly and assigned to oral health education intervention group A, B and C. All the communication with study participants was done in Pakistani sign language with the help of their teachers. There was no blinding, as the intervention and evaluation was carried out by the main investigator and study participants cannot be blinded because the 3 interventions were visibly distinct. Participants in group A were assigned a skit video method of oral hygiene intervention and shown 5 minute video on what to eat and how to brush their teeth. The video included that what is good and bad for teeth, and how to brush which includes method, time and duration of tooth brushing. The tooth brushing technique shown in video was horizontal scrub technique with 2 minutes brushing for 2 times. Participants assigned to group B and C was provided same instructions for tooth brushing and eating habits in the form of pictures and sign language respectively. The children of Group B received instructions in the form of laminated cards and asked to take with them at home. Participants in group C received instructions in sign language provided by certified deaf interpreter (CDI) in Pakistani sign language. The teachers were there for assistance and facilitation to participants in provision of all interventions. Only hearing impaired individuals were involved in to guide for proper technique of tooth brushing.
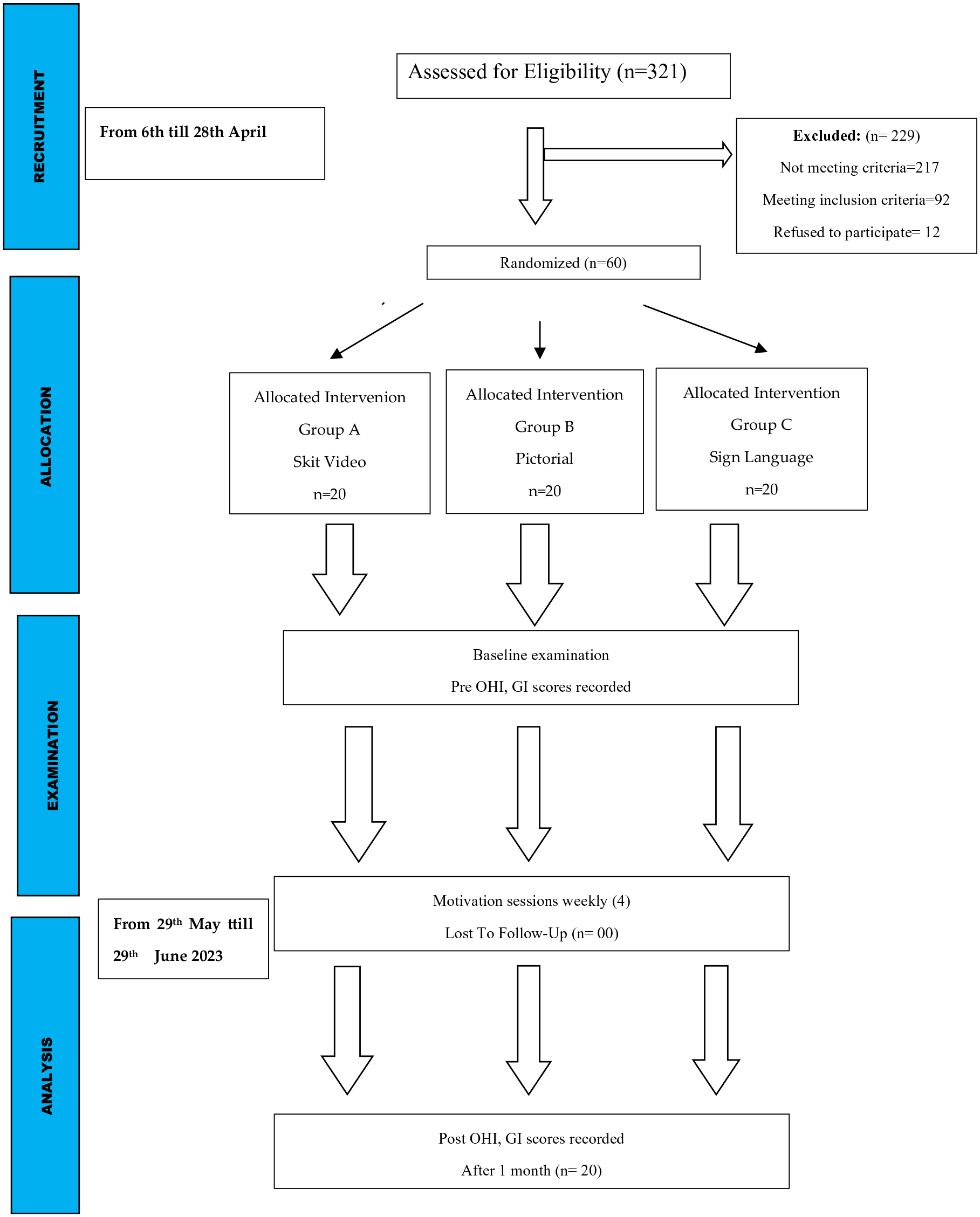
Flow diagram of the study.
Data Collection
A self-structured questionnaire was used to record demographic details and oral hygiene habits. Thereafter, oral examination was performed using sterilized instruments on portable dental unit under daylight. The Gingival (GI) by Loe & Silness 19 and simplified oral hygiene index (OHI-S) index 20 scores of the participants was recorded. The scores were recorded on the mesial, distal, and middle surface of the buccal and lingual surface of 6 index teeth for permanent dentition which are 16, 12, 24, 44, 32, and 36, respectively. The scores were recorded on 6 index teeth for deciduous dentition was 54, 61, 82, 75, 26 and 46. The index gives no instructions about which teeth to select when use index in primary dentition, primary predecessors were used where index teeth was missing. A total of 6 measurements were taken, and their average score was calculated. Oral hygiene was categorized as “Good,” “Poor,” and “Fair.” Gingival health was categorized as “healthy,” “mild gingivitis,” and “moderate gingivitis.” The clinical oral examination of each of the participant was performed by single examiners (M.M.) dentist by profession and calibrated.
Reinforcement Sessions and Post-Intervention Evaluation
Motivation sessions were conducted every week to reinforce the oral hygiene education provided to the study population at baseline. In reinforcement sessions the same method of education was repeated and 4 sessions were performed by principal investigator (MM). During sessions the doubts and questions of study participants were answered to clear any confusion. After 1 month, a post intervention examination was performed on the same parameters as evaluated at the baseline to compare the effects of the 3 intervention methods to improve oral health status.
Ethical Approval and Informed Consent
Ethical approval for the study was obtained from the Ethical Review Committee of Bahria University, Karachi, Pakistan (reference number ERC 23/2023). A written consent was taken from children parents before execution of study and only consenting children were included in the study.
Statistical Analysis
The Statistical Package for the Social Sciences software SPSS (IBM, version 25, Chicago, Illinois, United States) was used. The mean values and standard deviation were calculated for oral health habits, OHI and gingival scores along with descriptive analysis such as frequencies and percentages of the given data. In each of the groups, pre intervention and post intervention scores were recorded. A 1-way ANOVA test was used to see any statistically significant difference between pre and post intervention scores within and between each group. A P-value of ≤ .05 was considered to be as statistically significant.
Results
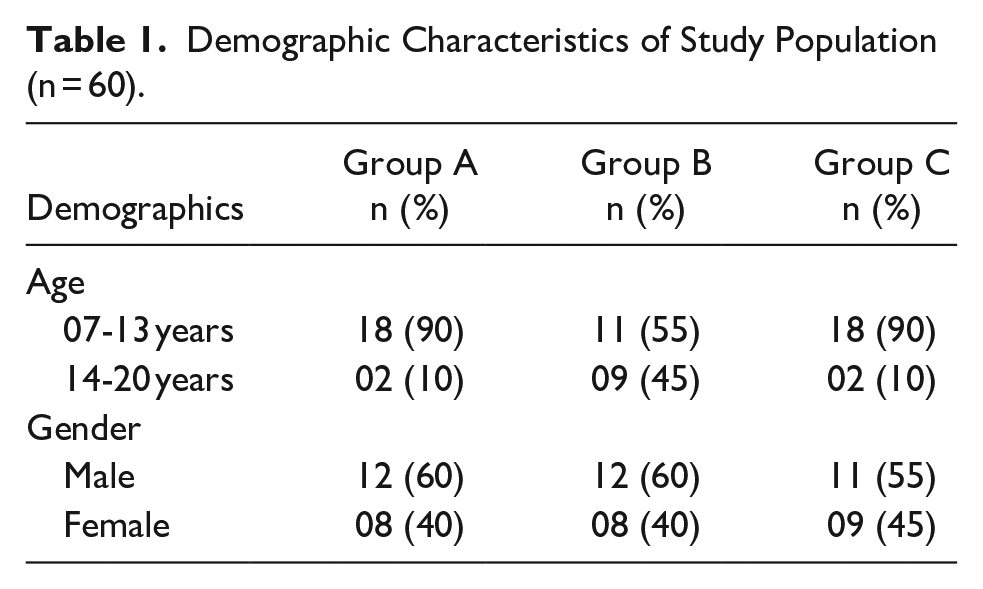
In this study, a total of 60 children were included and successfully completed the study after 1 month of follow-up. Out of 60 children, there were 35 males (58.3%) and 25 females (41.6%). Regarding age, 47 (78.3%) belonged to 07 to 13 years of age; 13 (21.7%) belong to 14 to 20 years of age. In group A (Tailor made video), there were 20 hearing impaired children; in group B (Pictorial) there were 20 children, and 20 children in group C (Sign language/control). In both groups A and C, there were 18 children aged between 07 and 13 years and 2 children between 14 and 20 years of age. For group B, there were 11 children aged between 07 and 13 years and 9 children between 14 and 20 years of age. About the gender of each group, there were 12 males and 08 females in groups A and B, and 11 males and 09 females’ in-group C. (Table 1).
Demographic Characteristics of Study Population (n = 60).
Oral hygiene habits of 3 groups were compared, significant difference was found for all oral hygiene habits in Group A, water rinses, tooth brushing time showed significant difference in group B. On the other hand, only mouthwash use was found to be significant in group C (Table 2).
Comparison of Oral Hygiene Habits of Group A, B and C Pre and Post Intervention.

significant p-value <0.05.
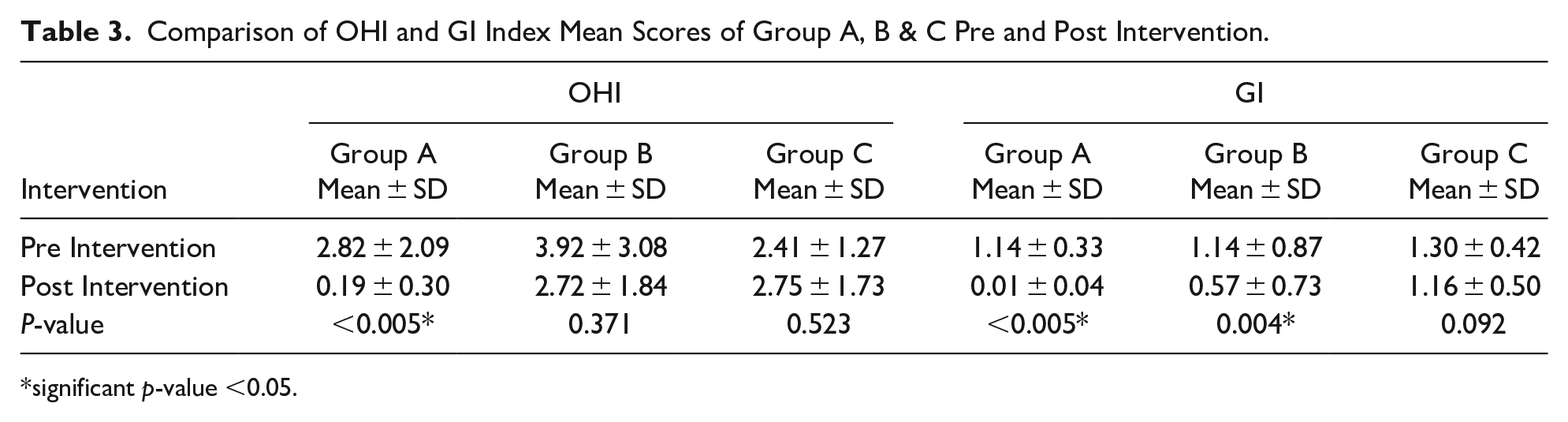
The mean OHI score pre intervention for group A was 2.82 ± 2.09, group B 3.92 ± 3.08, and group C 2.41 ± 1.27. After the intervention, the mean OHI scores were as follows: group A: 0.19 ± 0.30, group B: 2.72 ± 1.84 and group C: 2.75 ± 1.73. The mean GI index scores pre intervention for group A was 0.01 ± 0.04, group B 0.57 ± 0.73, and group C 1.30 ± 0.42. A statistically significant difference (P < .005) was found for OHI score as compare to group B and C. On the other hand statistically significant difference was found for GI scores in group A (<0.005) and B (0.005), whereas no significant difference (P = .37, 0.52) was found for OHI scores in group B and C respectively. Similarly, no significant difference was observed for GI scores in group C, (Table 3).
Comparison of OHI and GI Index Mean Scores of Group A, B & C Pre and Post Intervention.
significant p-value <0.05.
About the comparison of OHI and GI scores among the 3 group post interventions, a statistically significant difference was found between group A and group B (P < .005). Similarly in group A and group B, OHI and GI scores were also found to be statistically significant (<.004). On the other hand, no statistically significant difference was found between OHI and GI scores of groups B and C (.353), Table 4.
Inter group Comparison of OHI and GI Scores Post Intervention.

Regarding OHI status of the 3 groups post intervention, “good” oral hygiene was noted in 20(100%) hearing impaired children in group A, 3(15%) in group B, and 1(05%) in group C. “Fair” oral hygiene was noted in 11 (55%) children belonging to group B, 13 (65%) in group C and none reported fair and poor oral hygiene in group A. On the other hand fair oral hygiene was noted 06(30%) in group B and C. About the health of the gingiva (GI), 19 hearing impaired children (95%) in group A, 5 (25%) and 4(20%) reported having “healthy” gingiva respectively. Furthermore, “mild” gingivitis was found in 1 (5%) children in group A, 11 children (55%) in group B, and 5 children (25%) in group C. Lastly, “moderate” gingivitis was not established in any of the children belonging to group A, but it was found in 4 children (20%) in group B, and 11 children (55%) in group C (as presented in Table 5).
Gingival & Oral Hygiene Index Status Amongst Participants at Post Intervention.

Discussion
It is crucial that we design instructional methodologies to provide students with disabilities with an inclusive learning environment in the modern world. Research suggests that, learning with visual aids is more efficient than learning from written instructions. It is important to comprehend how HI people learn in a culture where mostly auditory learning is used to get by in daily life. According to specific researches, HI people rely heavily on visual cues to learn new information. 23 In literature, numerous studies have evaluated different strategies to improve oral health such as giving direct or indirect personal tasks, written instructions, and audio-visual modalities provision.21-24 In current study, video was used as an oral hygiene education intervention, to help children with hearing impairment to improve their oral health. According to our findings, video-based interventions significantly decreased both the mean oral hygiene and gingival scores for the children as compared to group C in which oral hygiene education intervention was given in sign language. These findings correspond with a study by Saikiran et al, where a decrease in plaque scores was noted by using video intervention. 24 Similarly, another study by Yanti et al reported a decrease in OHI scores when oral health educational video was used as an oral hygiene education intervention. 25 The advantages associated with video-based interventions are that they can be repeatedly seen and imitated by the children when they are brushing their teeth and recall the information provided, cost effective as well.
The visual technique of oral health education intervention was employed in the form of laminated cards in this study to help children with hearing impairment to maintain better oral health. In this study, it was discovered that showing children illustrations of dental care instructions significantly decreased the mean gingival scores. These results are consistent with the research by Arunakul et al, which found that illustrated books helped hearing-impaired children increase their gingival scores. 22 These results also line up with a number of studies where hearing challenged kids’ oral health education improved as a result of seeing graphics in a book.26,27 Additionally, lip reading and sign language have been employed as a way to help hearing-impaired kids take control of their oral health. According to Hashmi et al’s study, using sign language as a means of delivering dental health education results in a mean reduction in simplified oral hygiene and gingival index. 17
According to a study, the modified bass method is noticeably more effective than the horizontal scrub method. When compared to other procedures, Zhang et al demonstrated that the Bass technique efficiently eliminated interdental plaque. 28 Due to their incapacity to use alternative tooth brushing procedures, young children have previously been reported in several studies to prefer the horizontal scrub technique. In the present study majority of children used the horizontal scrub technique. Tooth brushing skill and the required manual dexterity for tooth brushing are developed in children aged 8 years and above. 29 Mescher et al reported that children aged 6 years and younger do not have the hand functions which are required for tooth brushing, and hence concluded that the sulcular brushing technique could be mastered by children 8 years and above. 30 Similarly, children in our study were instructed to clean their teeth horizontally. However, it could be challenging to stick to a specific tooth-brushing technique, especially for young children.
In this study, oral hygiene was rated as good, fair, or poor. At the conclusion of the interventions, the majority of the children in group C (Sign language) had mediocre dental hygiene, while all of the children in group A (video) had good oral hygiene. However, there were equally as many children with poor dental hygiene in areas where oral health education was given using graphics and sign language. These findings are consistent with a study that used oral hygiene educational treatments to find similar oral hygiene improvement in children with intellectual disabilities. 31 There were few limitations in this study despite its positives, such as the random assignment of children to interventional groups to eliminate biases and the adherence to ADA (American Dental Association) and CONSORT principles. First, the dental plaque was evaluated solely by eye inspection without the use of plaque disclosing agents. Second, the follow-up period was only 1 month long. One of the limitations of this study is that it is non-blind trial and blinding was not possible which may leads to conscious or unconscious influence on the behavior of participants and researcher, researchers may inadvertently influence the study outcomes if they know which participants are receiving the treatment. Participants who know they are receiving the treatment might have certain expectations about its effectiveness. Another limitation is difference in the ages of participants in each group may have influenced the results because child’s age may favor some of the methods studied. Ideally, sampling would be stratified by age which was not performed. Calibration was also not performed for the parameters which is also a limitation of the study. In the future, customized oral health services and programs should be planned to increase access and delivery of essential oral health care. To further understand efficient and patient-centered communication techniques for people with HI during oral health education and treatment, the findings suggest the necessity for longitudinal evaluation-based randomized trials research on a wide scale.
Conclusions
Our findings demonstrated that the skit video intervention significantly enhanced oral hygiene status, as evidenced by a reduction in mean oral hygiene and gingival scores. This highlights the effectiveness of skit videos as an educational tool for improving the oral health of children with hearing impairments. In addition, gingival parameters were also improved with pictorial interventions. Overall, this study emphasizes the significance of innovative approaches in addressing the unique challenges faced by this vulnerable population, emphasizing the vital role of oral health in their overall well-being. Further research and the development of tailored interventions are warranted to continue improving the oral health of children with hearing impairments and promoting their overall health and quality of life.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241240302 – Supplemental material for Enhancing Oral Hygiene in Children With Hearing Impairment: The Impact of Skit Video Interventions -A Randomized Controlled Trial
Supplemental material, sj-docx-1-gph-10.1177_2333794X241240302 for Enhancing Oral Hygiene in Children With Hearing Impairment: The Impact of Skit Video Interventions -A Randomized Controlled Trial by Maria Moin, Muhammad Mohsin Haider, Kulsoom Fatima Rizvi, Rabia Imtiaz, Afsheen Maqsood, Sara Altamash, Naseer Ahmed and Artak Heboyan in Global Pediatric Health
Footnotes
Acknowledgements
The authors want to take this opportunity to express their appreciation to the patients who agreed to participate in this study. The authors are grateful to the research development and review cell of Altamash Institute of Dental Medicine Karachi, Pakistan, for guidance and support in this study. The author’s team also oblige the Yerevan State Medical University after Mkhitar Heratsi, Yerevan, Armenia, for supporting this project.
Author Contributions
MM: contributed to conception or design; contributed to acquisition, analysis; drafted the manuscript; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. MMH: contributed to conception or design; contributed to acquisition, analysis; drafted the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. KFR: contributed to conception or design; contributed to acquisition, analysis; drafted the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. RI: contributed to conception or design; contributed to acquisition, analysis; drafted the manuscript; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. AM: contributed to conception or design; contributed to acquisition, analysis, interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. SA: contributed to conception or design; contributed to interpretation; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. NA: contributed to conception or design; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. AH: contributed to conception or design; critically revised the manuscript; gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Bahria University Health Sciences, number (ERC 23/2023) and was conducted in agreement with the ethical standards of the declaration of Helsinki.
Ethics Approval
Ethical approval for the study was obtained from the Ethical Review Committee of Bahria University, Karachi, Pakistan; under the reference number ERC 23/2023.
Informed Consent
A written consent was taken from children parents before execution of study and only consenting children were included in the study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.