
Abstract
Carbonic anhydrase II deficiency is an extremely rare inborn error of metabolism that constitutes a triad osteopetrosis, renal tubular acidosis and intracerebral calcification. Unlike other subtypes of osteopetrosis, the presence of developmental delay and relative infrequency of skeletal fractures may not be a typical signs of symptoms indolent trajectory. This case report demonstrates a 11-year-old boy who had a bilateral midshaft tibial fracture despite low mechanism of injury. He was found to have severe respiratory distress with hypokalemia shortly after arriving to the emergency department venous blood gas (VBG) showed moderate metabolic acidosis. Potassium was corrected but he persistently had low potassium level despite frequent corrections. He was then started on sodium bicarbonate boluses. Whole exome sequencing (WES) was sent, and result was consistent with autosomal recessive osteopetrosis type III with renal tubular acidosis (RTA) evident by pathologic variant on CA2 gene confirming the diagnosis of carbonic anhydrase II (CA II) deficiency consistent with the unique Arabic mutation. Conversely, low mechanism of fracture injury in the context of severe form of fracture type should raise the concern of (CA II) deficiency especially in a pediatric patient who show no signs of developmental of cognitive delay.
Keywords
Background
CA II deficiency is an extremely rare autosomal recessive inborn error of metabolism. It encompasses a triad of osteopetrosis, RTA and intracerebral calcification.1-3 CA II is crucial for the skeleton and renal tubules functions. 4 It plays a significant role in acid-base homeostasis and facilitates the augmentation of osteoclast activity for the purpose of bone resorption. In general, individuals of Arabic descent with CA II deficiency commonly exhibit symptoms such as mental disability and severe metabolic acidosis, while demonstrating a lower susceptibility to fractures. In contrast, individuals of European and North American descent with CA II deficiency are more susceptible to easily fractured bones and a lesser degree of cognitive impairment. 4 Although different ethnic backgrounds have been associated with this condition, predominance has been strongly reported in patients of Arabic descent pertained to a homozygous splice junction mutation at the 5’ end of intron 2. These patients portray a unique mutation in the CA2 gene (c.232 + 1G > A) which is previously described as the Arabic mutation. 5 Nearly more than 75% of CA II-deficient patients that have been recognized so far were from Arabic descent. 6 These patients exhibit a severe form of developmental delay and metabolic acidosis with a comparatively lower incidence of bone fractures. Unlike other subtypes of osteopetrosis, the onset of symptoms is insidious and follows a protracted course. 6 The presence of developmental delay and the relative infrequency of skeletal fractures differentiate the course of illness and presentation from any other mutation that may cause CA deficiency.5,7
In the present report, we demonstrate an unusual presentation of CA II deficiency in a pediatric patient.
Case Presentation
An 11-year-old boy known to have mild intermittent asthma recently sustained bilateral midshaft tibial fractures following a fall while navigating multiple flights of stairs at school. He immediately felt excruciating pain with rapidly evolving swelling around the anterior part of the bilateral tibia along with a markedly restricted range of motion. No neurovascular deficits were noted. Past medical history is noncontributory. Past surgical history is consistent with a previous left tibial fracture in spite of a minimal mechanism of injury 3 years ago treated conservatively. The patient is not on any regular medication. Immunization is up-to-date. Psychomotor development is appropriate for chronological age. Family history did not reveal any recurrent fractures in the context of mild mechanisms of injury among family members. He was born to healthy consanguineous parents (third-degree relatives). He also has one healthy sister.
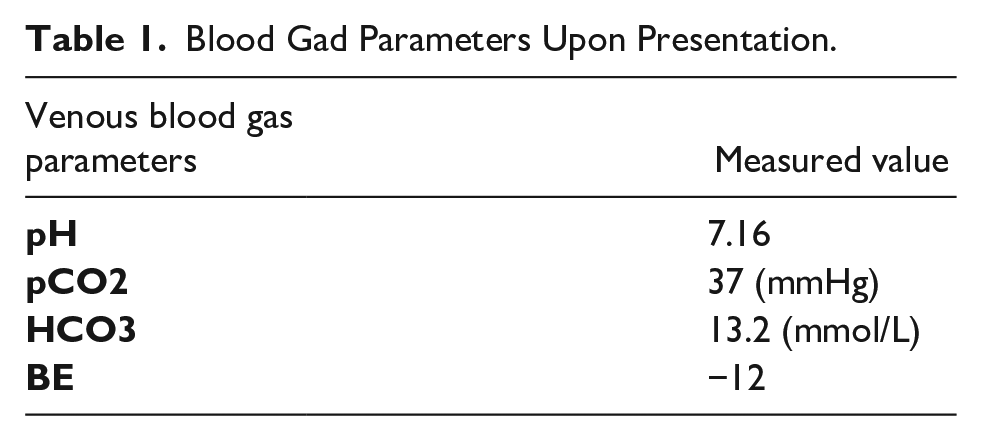
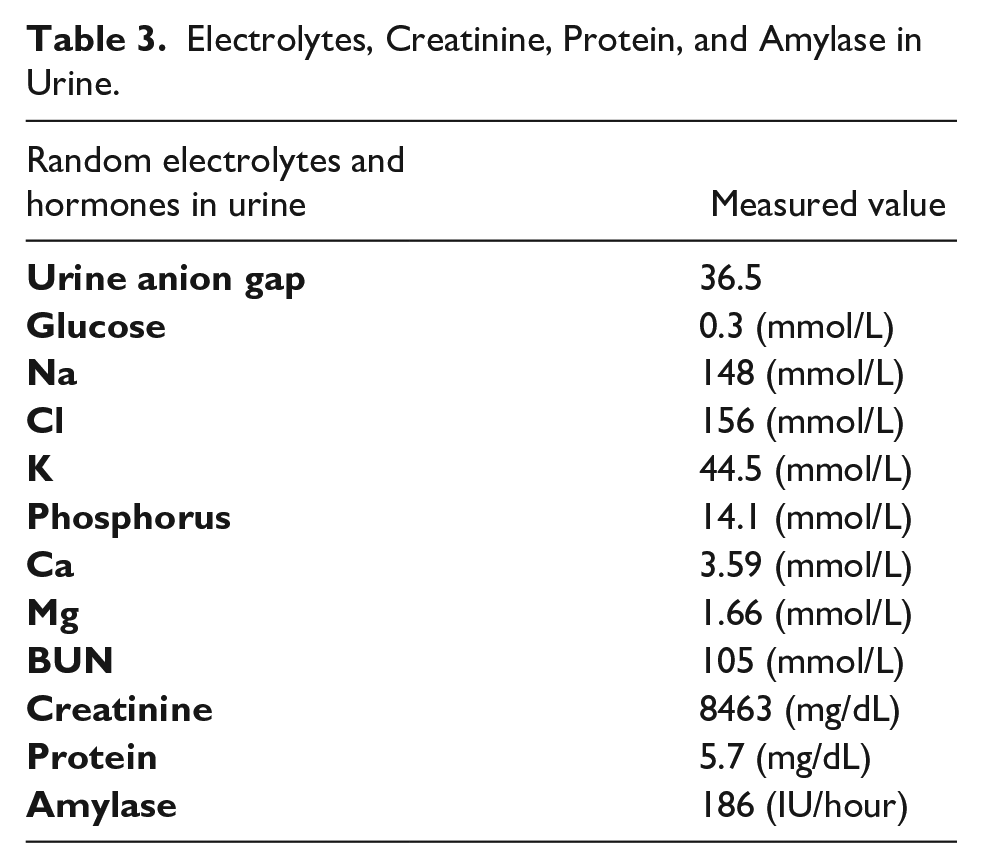
Upon physical examination, the general appearance showed a well-hydrated child, severely in pain, conscious and alert. Bilateral lower limbs deformities were observed more profoundly on the left side. Musculoskeletal examination revealed tenderness over bilateral lower limbs with soft compartments. Cardiopulmonary and gastrointestinal examinations were unremarkable. Cranial nerves functions were appreciated and intact sensory and motor systems. The orthopedic team was informed. Subsequently, he suddenly developed severe respiratory distress with hypokalemia of 2.7 mmol/L. 5 L/min O2 via a nonrebreather mask was promptly commenced. VBG showed signs of moderate metabolic acidosis as shown in Table 1. The pediatric team started him on frequent salbutamol and budesonide nebulization. As a part of the respiratory distress investigation, a chest X-ray was performed, and it showed incidental findings of generalized high bone density (Figures 1 and 2). Surgical reduction was rescheduled for the next day after patient optimization of respiratory status and potassium level. A closed reduction and above-knee cast was applied after stabilization. His serum electrolytes and hormonal function are depicted in Table 2. On the fifth day of admission, he was reported to have a low potassium level again (2.9 mmol/L). He was started on potassium chloride (KCl) 30 mEq/L added to intravenous (IV) fluid. Pediatric nephrology evaluated the patient due to persistent metabolic acidosis. The level of random electrolytes in urine, creatinine and amylase are shown in Table 3. The first anion gap (AG) was 22.8, consistent with high AG metabolic acidosis. IV fluid was increased to one and a half maintenance. Urine and serum osmolality were requested. The kidney, ureter, and bladder (KUB) ultrasound was unremarkable. The patient was started on sodium bicarbonate boluses every 8 hours. Pediatric genetic and metabolic team was consulted regarding increased bone density seen on pelvic and lower extremities X-rays. WES study was requested. The sample was collected from the blood and the result was consistent with autosomal recessive osteopetrosis Type III with RTA evident by a pathological variant on the CA2 gene (c.232 + 1G > A). A constellation of findings constituting a genetic diagnosis of CA II deficiency. WES report details are shown in Table 4. An in-house bioinformatics pipeline including read alignment to GRCh37/hg19 genome assembly and revised Cambridge reference Sequence of the human mitochondrial DNA (NC_012920), variant calling, annotation and comprehensive variant filtering was applied. All variant with minor allele frequency lf <1% in the Genome Aggregation Database and Human Gene Mutation Database (HGMD®) were evaluated. The investigation for the relevant variants is focused on coding exons and flanking ±10 intronic nucleotides of genes with a clear gene-phenotype evidence based on Online Mendelian Inheritance in Man (OMIM®). Moreover, biochemical analysis was performed upon detection of the variant by sequencing to confirm the diagnosis of metabolic disorder optimize the variant classification based on American College of Medical Genetics and Genomics (ACMG) recommendation. The copy number variation (CNV) detection has a sensitivity of more than 95% for all homozygous/hemizygous and mitochondrial deletions as well as heterozygous deletions/duplications and homozygous/hemizygous duplications spanning at least 3 consecutives exons. Variants with unclear zygosity or low sequencing quality were confirmed by orthogonal methods such as single nucleotide variants and small insertions/deletions by Sanger sequencing, CNV by multiplex ligation-dependent probe amplification, quantitative polymerase chain reaction, or chromosomal microarray.
Blood Gad Parameters Upon Presentation.

Osteoporotic changes of the right lower leg consistent with CA II deficiency.

Bilateral view of the lower extremities showing osteoporotic changes manifested by high bone density.
Serum Electrolytes, Kidney, and Hormonal Functions.

Electrolytes, Creatinine, Protein, and Amylase in Urine.
WES Report Details.

The mutation has been previously described to cause the latter disease2,5,7 with a contextual emphasis on the triad of the clinical picture as a classical presentation unlike the current presentation for this patient.
A skeletal survey was done and showed markedly increased bone density. KUB ultrasound revealed no nephrocalcinosis or renal calculi. Kidney size was within the normal range for age. The patient was started on IV sodium bicarbonate boluses. Adenoid hypertrophy grade II was recognized as well. After stabilization, the patient was discharged with potassium, sodium, hydrogen citrate powder, and vitamin D. He was then followed in pediatric orthopedic clinic within 2 weeks, pediatric metabolic and genetic within 6 months as well as pediatric nephrology through 2 weeks period. He underwent magnetic resonance imaging for the brain as planned by the metabolic/genetic team to evaluate for cerebral calcification after 4 months from discharge (Figure 3). Regular follow up with pediatric nephrology was mandated to evaluate response to therapy and compliance. Pediatric orthopedic stated that rapid recovery and healing was noted. Written informed consent was obtained from the legal next of kin of the subject in the case report for publication.

Axial MRI study showing symmetrical bilateral basal ganglia calcification consistent with CA II deficiency.
Discussion
CA II belongs to a family of metalloenzymes comprising 7 isomers. The primary function is to catalyze the conversion of carbon dioxide into carbonic acid for the purpose of pH regulation. Despite the importance of all subtypes in many physiological processes, CA II remains the most widely distributed enzyme expressed in the cytoplasm of nearly every tissue and organ. The aforementioned cellular entities encompass a range of diverse types such as osteoclasts, oligodendrocytes, the ciliary body of the eye, the lens, hepatocytes, the proximal and distal tubule of nephrons, acinar cells of the salivary gland, gastric parietal cells, endometrium, endothelial cells, epithelial cells of the seminal vesicle, erythrocytes, platelets, and spermatozoa. 6 CA II plays a pivotal role in the regulation of acid-base homeostasis. It facilitates H+ secretion by gastric partial cells as well as renal tubular cells in order to contribute to urinary acidification and by osteoclasts to ensure acidity in the bone resorbing compartment. Furthermore, CA II enhances CO2 exchange in the proximal kidney tubules. 6 Hence, CA II deficiency results in a variety of organ dysfunctions, mainly osteopetrosis, RTA and intracerebral calcifications. Despite the latter triad of clinical manifestations, several other less common manifestations may be exhibited such as growth suppression, mental regression, and obstructive sleep apnea. The antecedent statements are consistent with the demonstrated case elucidating a rare presentation of CA II deficiency with bilateral tibial fracture secondary to osteopetrosis with RTA evident by metabolic acidosis in the context of hypokalemia. 8
The majority of patients diagnosed with CA II deficiency present initially with a failure to thrive or motor delay.9,10 Similarly to some extent, Alhuzaim et al. 2 reported a case of an adult female who was evaluated for high bone density, delayed developmental milestones and poor school performance as well as multiple bone fractures started at the age of 15 that required operative reduction. Prior to presentation, she developed profound weakness due to severe hypokalemia. Although she presented with a protracted course of developmental delay, frequent complex fractures that occur in the setting of low mechanisms of injury raise the suspicion index of an underlying CA II deficiency as was incidentally found in our reported case. Patients may initially show subtle incidental signs of osteopetrosis and RTA prior to the emergence of developmental delay as shown in our reported case raising a suspicion on the influence of puberty on the developmental regression. Hypokalemia and metabolic acidosis seem to be of chronic course that can be subtle. Moreover, the severity of bone metabolism dysregulation could lead to unpredictable complications, as reported by di Palmo et al., 10 who described a CA II deficiency case complicated by severe obstructive sleep apnea pertained to abnormal craniofacial bone growth without significant tonsillar hypertrophy. Furthermore, cranial nerves entrapment could also be the result of a long-standing CA II deficiency as reported by Ali et al., 11 who described an adult male of Arabian descent with deafness and decreased visual acuity.
Conclusion
Disproportionate low mechanism of injury to the severe form of fracture in the context of incidental finding of metabolic acidosis and refractory hypokalemia in a patient from an Arabic descent indicates relatively higher index of suspicion for CA II deficiency. Various organ dysfunction such as osteopetrosis, RTA and intracerebral calcification are anticipated among the clinical presentation. Failure to thrive, developmental delay and mental regression might be an associated features as well. Subtle signs of RTA and osteopetrosis might precede onset of developmental delay in patients prior to onset of puberty. Hence, developmental delay might not emerge until later in the adolescence period.
Footnotes
Authors’ contributions
Authors testify that all persons designated as authors qualify for authorship and have checked the article for plagiarism. If plagiarism is detected, all authors will be held equally responsible and will bear the resulting sanctions imposed by the journal thereafter. YA conceived the case report, collected, and analyzed data. WG wrote the initial draft of the article and provided logistic support. RY reviewed the final draft and provided supervision. All authors have critically reviewed and approved the final draft and are responsible for the manuscript’s content and similarity index.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Approval from the institutional review board (IRB) of King Saud Medical City (KSMC) was obtained (H2RI-14-Sep23-01). Informed consent was also signed by next of kin.
Informed consent
Written Informed consent was obtained from legally authorized next of kin to publish the details pertained to the case report of the subject involved.