
Abstract
Distal renal tubular acidosis can present with acute-onset quadriparesis caused by severe hypokalemia, and primary Sjögren’s syndrome is a significant potential cause of distal renal tubular acidosis in such patients. The extrahepatic manifestations of chronic hepatitis C virus infection can mimic those of primary Sjögren’s syndrome, creating a diagnostic dilemma. Here, we present the case of a woman in her mid-20s who presented with sudden-onset quadriparesis. Laboratory investigations showed severe hypokalemia, normal anion gap metabolic acidosis, and positivity for antinuclear and anti-Ro/Sjögren’s syndrome–related antigen A antibodies. Further evaluation confirmed a positive hepatitis C virus antibody test but a negative viral load. A diagnosis of primary Sjögren’s syndrome with distal renal tubular acidosis was established, accounting for the hypokalemia. Potassium supplementation and correction of acid–base disturbances led to significant patient improvement. This case highlights the importance of including autoimmune conditions such as primary Sjögren’s syndrome in the differential diagnosis of patients presenting with hypokalemic quadriparesis and distal renal tubular acidosis, even in the absence of glandular symptoms. Early diagnosis and management are essential to improve outcomes.
Introduction
Hypokalemic quadriparesis can be an initial manifestation of distal renal tubular acidosis (dRTA), with Sjögren’s syndrome (SS) being the most common cause of acquired dRTA. 1 SS is a chronic autoimmune disease characterized by lymphocytic infiltration of exocrine glands and various extraglandular manifestations. 2 It can occur as primary SS (pSS) or secondary SS, associated with other autoimmune diseases. 3 Notably, hepatitis C virus (HCV) infection can mimic pSS by presenting with similar clinical and laboratory characteristics. 4 Here, we report the case of a woman in her mid-20s who initially presented with acute quadriparesis due to dRTA secondary to pSS with concurrent HCV infection. This case report has been written in accordance with the Case Report (CARE) guidelines. 5
Case report
A woman of Mongolian ethnicity in her mid-20s presented to the emergency department at B.P. Koirala Institute of Health Sciences, Dharan, Nepal, in September 2024 with a 1-week history of lower abdominal pain and recurrent vomiting. She also reported experiencing bilateral thigh and calf pain for 1 week. On the day of presentation, she had developed weakness in both her upper and lower limbs, rendering her unable to stand up from a sitting position. On further questioning, she reported having mild lower abdominal pain for 1 month, associated with nausea. She had visited the gynecology outpatient clinic 1 week prior to this presentation and was managed symptomatically. Her medical history included HCV infection, diagnosed 2 years ago during the birth of her second child. Her surgical history was significant for a cystectomy for a right ovarian cyst 4 years ago during the birth of her first child. Both her children were born via cesarean section. She had a history of receiving four pints of blood transfusion 4 years ago and two pints 2 years ago during childbirth. She had no history of diabetes, hypertension, or thyroid disease. At the time of presentation, she lived with her son, daughter, and husband. She was a nonsmoker and social drinker. She followed a nonvegetarian diet and was a homemaker. She had no family history of HCV infection and denied any high-risk behaviors. On examination, her pulse rate was 88 beats/min; blood pressure, 110/70 mmHg; respiratory rate, 18 breaths/min; temperature, afebrile; and oxygen saturation, 98% on room air. Abdominal examination revealed a soft, mobile, and fluctuant mass approximately 15 × 15 cm in size, palpable in the periumbilical, hypogastric, and right lumbar regions. Nervous system examination showed decreased power of 4/5 in the bilateral shoulders across all ranges of motion, 1/5 in the neck, and 1/5 in the bilateral hips and knees. Deep tendon reflexes were normal, and plantar responses were bilaterally down-going. The results of sensory, cranial nerve, and cerebellar examination were within normal limits. The remainder of the systemic examination was unremarkable.
An ultrasound examination of the abdomen and pelvis showed a large cystic mass (14.6 × 7.4 cm) on the right side of the pelvis with multiple septations suggestive of a complex adnexal cyst. Laboratory examination (Table 1) revealed severe hypokalemia. An electrocardiogram showed a normal sinus rhythm. A working diagnosis of quadriparesis secondary to hypokalemia was established. She was treated with intravenous fluids, potassium supplementation, and antiemetics. Despite adequate potassium and fluid supplementation, her potassium levels persistently remained low. An arterial blood gas (ABG) analysis was performed to rule out dRTA, which showed normal anion gap metabolic acidosis (Table 2). Her creatine kinase (CK), aspartate transaminase (AST), and alanine transaminase (ALT) levels were highly elevated. At this time, she was treated according to the established therapeutic protocol for dRTA, with sodium bicarbonate (1 g twice daily), spironolactone (50 mg once daily), and potassium chloride supplementation. However, inflammatory myopathy was considered an important differential diagnosis given the markedly elevated muscle enzyme levels. An antinuclear antibody (ANA) test was performed to rule out any underlying autoimmune disease; the result was positive.
Results of the laboratory investigations.
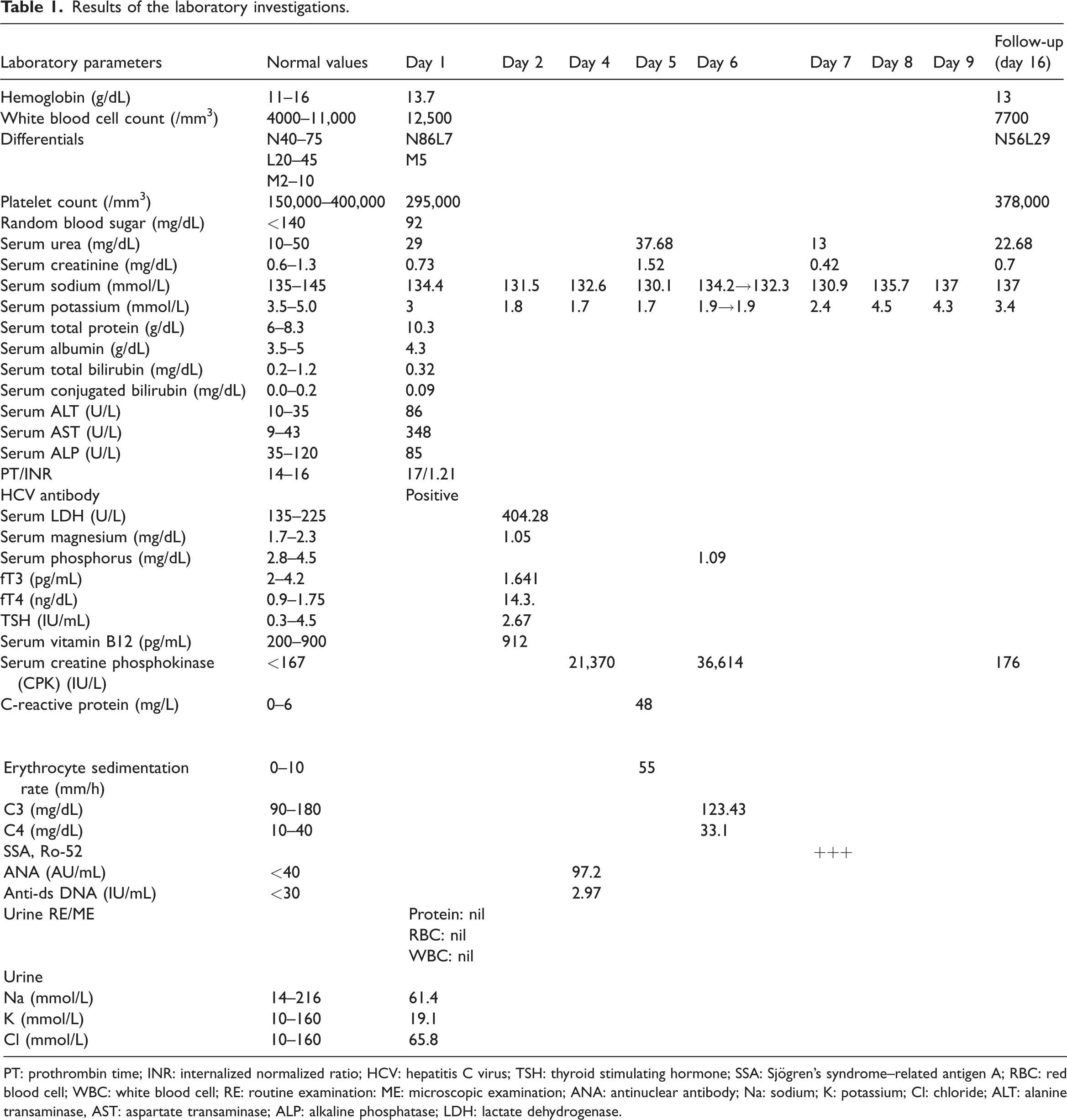
PT: prothrombin time; INR: internalized normalized ratio; HCV: hepatitis C virus; TSH: thyroid stimulating hormone; SSA: Sjögren’s syndrome–related antigen A; RBC: red blood cell; WBC: white blood cell; RE: routine examination: ME: microscopic examination; ANA: antinuclear antibody; Na: sodium; K: potassium; Cl: chloride; ALT: alanine transaminase, AST: aspartate transaminase; ALP: alkaline phosphatase; LDH: lactate dehydrogenase.
Results of ABG analysis.
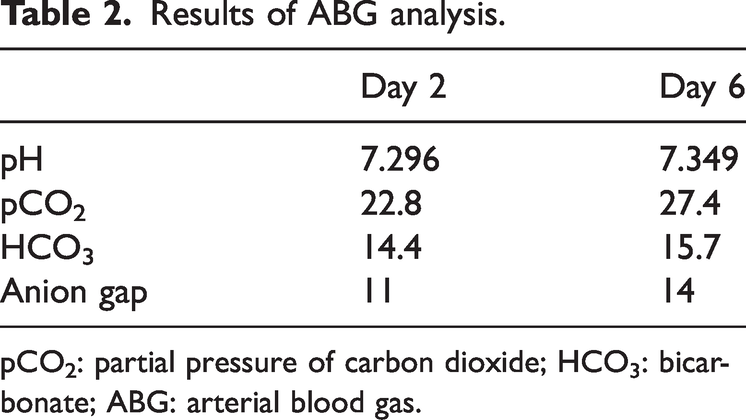
pCO2: partial pressure of carbon dioxide; HCO3: bicarbonate; ABG: arterial blood gas.
Upon further questioning, she reported experiencing symptoms of dry eyes for a few months, which she had initially considered a minor issue. Schirmer’s test was performed, which was positive (2 mm in both eyes), indicating bilateral severe dry eyes. A diagnosis of SS was considered due to the presence of dRTA and a positive ANA test. An extractable nuclear antigen (ENA) panel was also prescribed, although it was unavailable at our center.
After 4 days of treatment, the patient showed gradual improvement in her weakness and could walk by day 5 following hypokalemia correction. She was discharged with oral potassium chloride supplementation, 50 mg spironolactone once daily, and 1 g sodium bicarbonate twice daily. Surgery for the complex adnexal cyst was planned once her medical condition stabilized. At the 1-week follow-up, she reported no weakness; muscle power was normal in all limbs, and most laboratory parameters had normalized. The ENA panel subsequently revealed a strongly positive SSA antibody. Written informed consent was obtained from the patient for the publication of this case report and any accompanying images.
Discussion
Renal involvement is observed in approximately 5% of patients with pSS. The spectrum of kidney disease may include tubular dysfunction, nephrogenic diabetes insipidus, nephrolithiasis, tubulointerstitial disease, glomerular disease, immunoglobulin G4 (IgG4)-related disease, and progressive chronic kidney disease. 6 The incidence of dRTA in patients with pSS varies across studies, ranging from 5% to 70%. 7 dRTA, also known as type 1 RTA, is characterized by an impaired ability of the distal tubule to excrete H+ ions, consequently leading to normal anion gap metabolic acidosis and hypokalemia. 8 The mechanism of dRTA in pSS remains unclear; however, immunocytological analysis of the kidney biopsies of these patients has shown the absence of hydrogen adenosine triphosphatase (H-ATPase) pumps in the intercalated cells of the collecting ducts.9–10 Hypokalemia is usually asymptomatic; however, it can lead to muscle weakness or even paralysis in severe cases. 11 Our patient presented with quadriparesis, which was explained by a persistent low serum potassium level. Initially, the hypokalemia was attributed to vomiting. However, despite appropriate potassium and fluid replacement and no recurrence of vomiting, the patient showed no improvement, prompting further investigations. Other common causes of hypokalemia, including gastrointestinal losses (diarrhea), drugs such as diuretics, and intracellular shifts, were excluded. Although the initial serum magnesium level was low, correction of hypomagnesemia did not improve the serum potassium levels. Normal anion gap metabolic acidosis with refractory hypokalemia and exclusion of other potential causes supported the diagnosis of dRTA. Other causes of acute-onset quadriparesis, such as spinal trauma, thyrotoxicosis, acute transverse myelitis, acute inflammatory demyelinating polyneuropathy (AIDP), and other central nervous system conditions, were excluded through appropriate tests. Positive ANA and Schirmer’s tests suggested pSS, which was confirmed by the presence of SSA antibodies. However, given the patient’s positive HCV antibody, it remained uncertain whether the patient had true pSS or was exhibiting extrahepatic manifestations of chronic HCV infection mimicking pSS. The association between chronic HCV infection and pSS has been a subject of debate, with some studies showing a higher association while others revealing no significant link.12,13 Studies have shown that extrahepatic manifestations of chronic HCV infection may include sicca symptoms, positive ocular tests and antibodies, and lymphocytic infiltration of the salivary glands. 14 This necessitates the exclusion of chronic HCV infection, confirmed by a positive polymerase chain reaction (PCR) for HCV RNA, from the classification criteria for pSS. 15 However, in our patient, the PCR test was negative for HCV RNA, making chronic HCV infection an unlikely cause. However, HCV may have triggered an autoimmune process leading to the development of pSS, as both HCV and pSS are associated with similar B-cell-driven processes. 4 Other interesting findings in our patient were the elevated levels of creatine phosphokinase (CPK), AST, ALT, and lactate dehydrogenase (LDH), which favored the diagnosis of inflammatory myopathy. However, the acute onset of symptoms, absence of rash, absence of lung involvement, and constitutional symptoms as well as normalization of these enzymes without the use of immunosuppressants, contraindicated this diagnosis. In addition, hypokalemia itself is reported to cause rhabdomyolysis leading to elevations in muscle enzyme levels. 16 Although a minor salivary gland biopsy could not be performed due to technical issues, our patient met the classification criteria for pSS with a score of 4 out of 9, in the absence of other exclusion criteria. 15 The presence of HCV antibodies may have been coincidental rather than causative. Several case reports have described acute quadriparesis as a rare presentation of dRTA in pSS, highlighting the importance of considering tubular dysfunction in patients with refractory hypokalemia and muscle weakness.17–19 Early recognition and normalization of potassium levels can lead to rapid recovery of muscle strength, as observed in our patient.
Conclusions
This case highlights the diagnostic complexities encountered when distinguishing pSS from overlapping conditions such as HCV infection and inflammatory myopathies. Despite elevated muscle enzymes and HCV antibodies, the absence of active infection and normalization of muscle enzymes without immunosuppressants supported a diagnosis of pSS. The role of hypokalemia-induced rhabdomyolysis as a contributing factor highlights the importance of thorough evaluation.
Footnotes
Acknowledgments
The Grammarly tool was used for refining the language of this manuscript.
Author contributions
All authors contributed equally to the conception, manuscript writing, data curation, editing, and supervision of this study.
Code availability
None.
Consent for publication
Written informed consent was obtained from the patient to publish this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal. All patient details have been deidentified.
Data availability statement
The data supporting the findings of this case report are not publicly available due to patient privacy and confidentiality concerns. Deidentified data may be available from the corresponding author upon reasonable request.
Declaration of conflicting interests
None.
Ethical approval
Not applicable.
Funding
None.