
Abstract
Objectives. To assess knowledge of ethics knowledge among child healthcare professionals. Methods. We translated the Test of Residents’ Ethics Knowledge for Pediatrics (TREK-P) in Azeri and administered it to: (i) third-year medical students (n = 21), (ii) pediatrics residents (n = 24), (iii) practicing pediatricians (n = 21), and (iv) fellows (n = 9) who participated in a Fogarty International Center/National Institute of Health (Fogarty/NIH) R25 research ethics education program. The difference in the TREK-P score between the groups and the correlation between the TREK-P score and other factors were evaluated. Results. The fellows scored significantly higher than the other groups (P = .006). There was no significant difference between the other 3 groups. Within a joined group of pediatricians and fellows, previous training on ethics was the only factor that correlated with the higher TREK-P scores (P < .05). Conclusions. The higher scores in fellows support the effectiveness of postgraduate Fogarty/NIH training programs in research ethics.
Introduction
Research ethics, as underlined in the Belmont Report, is based on 3 main principles—beneficence/nonmaleficence, respect for persons, and justice.1,2 Drawing on more extensive philosophies underlying major ethics codes, declarations, and other documents, Emanuel et al 3 proposed 7 universal requirements that elucidate a coherent framework for evaluating the ethics of clinical research studies. The knowledge of ethical principles and adherence to them are essential components of professionalism. 4 In 2007, the Accreditation Council for Graduate Medical Education added the teaching and evaluation of professionalism to the Common Program Requirements for all residency programs in the US. 4 Residency training programs are also expected to include great attention to ethical training, as well as allocating requisite didactic hours for postgraduate trainees engaged in research work as part of Responsible Conduct of Research. There are few validated assessment instruments to measure knowledge of ethical principles. 5 The Test of Residents’ Ethics Knowledge for Pediatrics (TREK-P) is a standardized instrument to evaluate residents’ knowledge of pediatric ethics. 6 The TREK-P is easy to administer and can highlight content areas in which knowledge may be deficient.
Previous surveys showed that a significant proportion of researchers did not receive research ethics training. 7 Furthermore, there was inadequate and inconsistent knowledge of responsible conduct of research among new graduate biomedical sciences students. 8 Despite the increasing availability of training materials in research ethics, as well as attempts to integrate these resources into medical education and residency training program curricula, there remains an important need for improving teaching in this domain.9-14 The need is nowhere more salient than in low- and middle-income country (LMIC) settings. Medical practice and research in LMICs are burdened by different ethical complexities as underlined in the aftermath of clinical trials to interrupt the transmission of human deficiency virus (HIV) from mother to infant 15 that has subsequently led to the foundation of research education and training programs funded by Fogarty International Center/National Institute of Health (Fogarty/NIH) worldwide.16,17 The methods available for analyzing the ethical issues affecting scientific research and development in post-Soviet countries are limited. 18
In this study, we translated the TREK-P into Azeri to assess and compare the level of knowledge of research ethical principles among medical students, pediatric residents, pediatric practitioners, and other medical professionals working with children. Based on the original TREK-P research results 6 our initial hypothesis was that residents would score higher than students, and pediatricians would score higher than residents. We also sought to identify areas of deficits in knowledge in pediatric research ethics principles for the future guiding the development of ethics knowledge in Azerbaijan.
Methods
Study Instrument
The TREK-P is an open-source structured questionnaire that consists of 23 items covering 6 domains (Table 1). The questions are in a binary true/false format and correspond to statements written or endorsed by the American Academy of Pediatrics Committee on Bioethics. 6 The TREK-P was translated into the Azeri language by medical professionals with experience in translation and adaptation of similar tools. Only forward translation was conducted as the items were clear reflecting situational descriptions and there were no medical terms that could lead to ambiguous interpretation.
TREK-P Domains and Items.

Study Population
We administered the TREK-P to consenting participants with 4 levels of training and clinical experience at the Azerbaijan Medical University (AMU) in Baku, the only public medical university providing medical and postgraduate specialty training in the country as follows: (i) third-year medical students (novice group); (ii) residents across all 3-years of pediatric specialty training (residents group); (iii) practicing pediatricians with more than 4-years post-residency experience based in Baku (pediatricians group); and (iv) postdoctoral medical professionals working with children who had participated in a Fogarty/NIH-funded R25 research education program in the previous 5-years (fellowship group).
Since entry for medical studies in Azerbaijan can begin at ages 16 to 18 years, we focused on third-year medical students who were 18 years and older and could provide individual consent for participation. The pediatric residents were the only specialty trainees in Azerbaijan based at AMU. Medical students and pediatric residents were randomly selected from the list of students and residents attending the university clinic of AMU during the data collection period, and consecutively, approached and invited to participate. The Fogarty/NIH groups included the entire R25 program participants. The practicing pediatricians comprised an eclectic group of trainees and included former graduates of AMU residency in pediatrics, as well as graduates of pediatric residency programs in Turkey and the Russian Federation. The fellowship group was a mixture of postdoctoral former trainees who participated in a research education program based at AMU and in the United States.
Study Design and Data Collection
This was a cross-sectional descriptive study using a standardized questionnaire of ethics knowledge that effectively discriminates among learners in pediatric training that had been shown to be reliable and valid in prior research in the United States. 6 We conducted a survey using the Azeri version of the questionnaire in the settings of participants recruited from students and graduates of AMU in Baku. This data was collected over a 2-month period, from May to June 2021. Subjects who did not fulfil the inclusion criteria (required level of education; sufficient knowledge of the Azeri language) we excluded from the study.
Statistical Analysis
We
Results
There were 75 participants in 4 groups: 21 third-year medical students, 24 residents, 21 practicing pediatricians, and 9 former Fogarty/NIH fellows. Beyond the students and residents (graduates in specialty training), the average duration of the medical experience was 19.1 ± 13.1 (minimum 4 years and maximum 43 years) for the pediatrician and 12.1 ± 5.6 (minimum 6 years and maximum 22 years) for the fellowship groups respectfully.
ANOVA showed a significant difference between 4 groups of participants in TREK-P score (F(3, 71) = 4.522, P = .006). The fellowship group scored higher than all other groups (Table 2). The post hoc analysis showed that the fellowship group had significantly higher scores compared to the practicing pediatricians group (mean difference = 2.635, std. error = 0.739; P = .004). There was no significant difference in scores between other groups. The independent samples test in a joined group of pediatricians and fellowship participants (30 subjects) showed that only previous experience in training on ethics correlated with a higher TREK-P score (Table 3).
TREK-P Mean Scores.

The Correlation of the Mean Score of TREK-P With Other Variables Among the Pediatrics Practitioners and Postdoctoral Trainees With Research Education Experience.

Bold, t-test significant.
Discussion
It is important to formally develop reliable and valid measures of research ethics knowledge that can effectively discriminate among learners and to improve methods for measuring outcomes at all levels of medical education. The present research is the first to assess research ethics knowledge among medical students, residents, and pediatric medical professionals in Azerbaijan by means of a structured questionnaire previously developed in the United States. The results of this study revealed a lack of knowledge in several aspects of the research ethical principles related to pediatrics. Participation in structured formal training on ethical principles was the only factor related to better performance on the TREK-P among medical professionals. The use of the TREK-P is a novel application in the context of medical education in Azerbaijan, where there is a notable gap in research ethics education and where there are no medical education and residency training accredited requirements in ethics.
Clearly, a broader emphasis on measures of attitudes, skills, and behaviors is needed in addition to general knowledge of ethical principles and the use of the TREK-P in Azerbaijan represents an initial step in the development of benchmarks to evaluate research ethics training for medical students and pediatric residents, as well as continuing educational experiences in this area for practicing pediatrics professionals. It is important that the results reflect the current situation in settings involving students and residents at the AMU. The study can more broadly influence medical practice in Azerbaijan by improving the medical research education process. There are several reasons why we selected research ethics knowledge of pediatrics professionals as a focus of the study. Children are a vulnerable population and need more protection during research. Pediatrics has been the topic of Fogarty/NIH research in the country (“Optimizing prevention approaches for children reintegrating from orphanages in Azerbaijan” by NIH 1R01HD099847). The decisions in clinical and research practice involving children and adolescents are complicated by many aspects such as the involvement of third parties (parents and caregivers), and different levels of capacity to consent depending on the age of the child.
In the original TREK-P report, 6 performance on the test improved appropriately with degree of expertise with mean scores increasing with training levels, and residents performed significantly better than medical students. We expected that in our study residents also would score higher than the medical students and that the pediatricians would score higher than residents. In the original study, the median score for medical students was 15 (range, 11-19), which was close to the scores of medical students in the current study (Table 2). The median score for pediatric residents in the original study was 19 (range, 14-23), which was higher than medical students in this study. Our findings are of interest in that we noted a reverse though non-significant tendency with lower median scores for pediatric residents compared to those of medical students. Furthermore, the practicing pediatricians’ scores were lower than that of residents showing a temporal improved trend or greater proximity to training. The Fogarty/NIH fellowship group showed significantly better scores compared to the other 3 groups (Table 2). A positive aspect of the findings related to medical students at the AMU, the leading center in medical education in the country, is that they performed comparatively favorably (mean score 13.1, range 10-19) to students in the United States (median score 15, range 11-19). This may reflect the inclusion of modern curricula in medical education at the AMU and greater awareness and idealism of the novice group in the service of the patients.
This may reflect the inclusion of modern curricula in medical education at the AMU and greater awareness and idealism of the novice group in the service of the patients. Practicing pediatricians with greater experience were more defensive because they are not protected by approved governmental clear guidelines covering this area and they may be avoiding contradictory situations related to this area (eg, stopping ventilators or nutrition for terminally ill patients). We believe that the results revealed that practicing pediatricians already had negative experiences related to medical situations with significant ambiguity and learned to avoid making decisions that require a higher level of ethical responsibility. On the other hand, the students never experienced such difficult situations and took on a more idealistic common-sense stance on these ethical questions. Such a defensive approach taken by practicing pediatricians may influence their decision-making when they are involved in research studies. Given that these practitioners represent the higher echelon of urban practitioners in the country, the situation is likely to be worse in rural regions. These findings suggest that just practicing medicine per se is not enough to improve knowledge of ethical principles. Active training is the key to developing a solid understanding of ethics.
Given their stage of practice, we combined practicing pediatricians and fellowship groups to find out if other aspects of medical practice correlate with the TREK-P scores (Table 3). In our analysis, combining pediatricians who received medical education abroad and those who had previous experience of participation in research seemed to score higher, the comparative difference was not significant. The previous Fogarty/NIH training in research ethics was the only aspect that showed a significant positive correlation with the TREK-P mean score. We believe that participation in a structured training program on research ethics provides the participants with essential knowledge of ethical principles and enriches their understanding of fundamental ethical concepts, would explain their better performance on the TREK-P. These findings support the importance of R25-based postgraduate training on research ethics principles in Azerbaijan.
There are several possible explanations for the lack of correlation between performance on the TREK-P and the degree of expertise in our study population. The TREK-P questions correspond to the statements on the American Academy of Pediatrics Committee on Bioethics. 6 Though they reflect universal ethical principles, these principles haven’t been explicitly stated by similar bodies in Azerbaijan. Another obstacle is a general deficit of ethical training for residents and practicing pediatricians. For example, questions related to ethical issues constitute less than 1% of all questions used in the pediatrics residency examination and the license examination for pediatricians in Azerbaijan (sample test questions are available at the website of the Certification Commission of the Ministry of Health: http://snsk.az/). There are also usually a few sections and talks dedicated to ethical principles in programs of local conferences and seminars. Another factor that can contribute to the relative underperformance of practitioners is the lack of medical research overall in the country involving human subjects as well as participation in human subject ethics reviews.
We compared the pattern of TREK-P questions that the participants in all 4 groups answered either correctly or incorrectly (Figure 1). Such similarities in the rate of incorrect answers, independent of participants’ background, may point to specific areas that need greater attention during the research education process. Items Q3 (adolescent’s independent consent to therapy), Q8 (request for genetic testing of a 5-year-old by mother), and Q9 (request for genetic testing of a 5-year-old by mother after meeting with a genetic counselor) showed a very low rate of correct answers in our participants, and there was a high rate of correct answers in the original report (Figure 2). The answers to these questions might be significantly influenced by cultural differences (eg, a parent-dominated decision-making approach in children’s healthcare), as well as local legislation (as in the absence of emancipated minor concept) regarding research inclusion, as well as the age of consent and assent involving pediatric populations. Item Q3 is about a 15-year-old with Chlamydia giving consent for treatment without the involvement of the parents. According to Azerbaijani legislation, the person must be 18 years of age to give consent, therefore the answers are dominated by established practicing rules, rather than by ethical considerations. On the other hand, the treatment of sexually transmitted disease in a teenage female without permission and involvement of her parents is unacceptable from the point of view of the paternalistic tradition of Azerbaijan. Items Q8 and Q9 are about mother’s request to test her 5-year-old daughter. Most of the participants incorrectly answered that it is ethically acceptable to fulfill mother’s request. On 1 side this is appropriate from the point of the local legislation, on the other hand, the culturally accepted norm is that parents hold full rights over their little children. Interestingly, in item Q10 (request for genetic testing of a 17-year-old by mother against child’s wish) there was a higher correct answers rate in all our groups as compared to the original report data. Item Q10 is similar to Q9, but here the child’s age is 17 and she expresses unwillingness to have the test. This suggests that our participants accept the younger age as a main determinant of judging of request as ethical, providing more autonomy to teenagers and limiting the decision-making rights of 5-year-olds in favor of their parents. Participants in all groups showed high rates of correct answers in item Q7 (disclosure to parents regarding their newborn child’s being a carrier for sickle cell disease) and item Q17 (administration of large doses of analgesics to a child with refractory metastatic cancer). These questions focus on topics that are less influenced by either cultural or legal environment.

Rate of correct answers in 4 groups of participants.
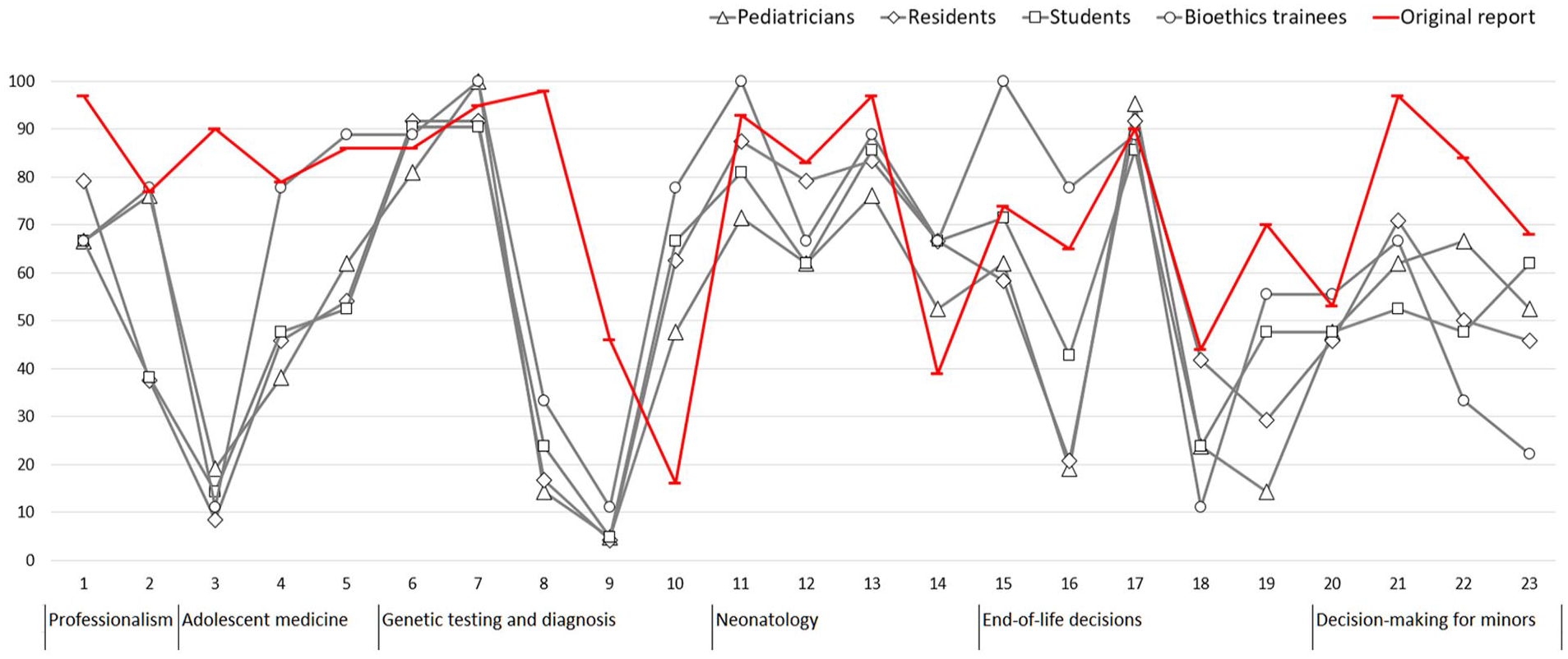
Rate of correct answers in 4 groups of our participants (gray) and reported original data (red).
In this study, questions most frequently answered incorrectly pertained to decision-making for minors. This is true for the last 4 items of the questionnaire that are designed as a separate domain, but also this holds true for other questions where participants incorrectly assigned full authority to decide to parents (Q3, Q8, and Q9). Another domain that was difficult is end-of-life decisions, where some questions particularly yielded a very low rate of correct answers.
In the study by Tekleab and Lantos, 19 the mean ethics knowledge score of the respondents (the residents and consultants in the department of pediatrics) was 12.3 ± 2.34, which is close to the scores of residents and pediatricians in our study. The participants of both studies performed poorly on the same items, for example, Q16 (decision to refuse further life-sustaining medical treatment by a 16-year-old), Q18 (distinctions between deciding not to start a life-sustaining treatment and deciding to stop it), and Q19 (withdrawal of enteral nutrition in a child in persistent vegetative state; Figure 1). Interestingly, the highest scores in that study 19 were among third-year residents, which has another similarity with our study, where residents scored higher than more experienced practitioners.
Limitations
Our study has several limitations. First, the TREK-P instrument was developed for assessing ethical knowledge in the setting of a pediatric residency training program in the United States. There are significant differences between the educational systems in Azerbaijan and the United States as noted above. The issues raised in some questions are strictly regulated by legislation in Azerbaijan, and many professionals are used to these rules and are likely not to question their ethical validity. Nevertheless, the questioning of ethical aspects of currently accepted practice precedes future changes of practice to more ethically appropriate and justifiable directions. Second, participation was voluntary across the groups leading to the influence of selection bias in the results likely to reflect more favorable knowledge among participating groups. Such a bias, however, will clearly lead to more favorable direction in the outcome of the results which otherwise reflected considerable deficits in knowledge except for the fellowship group who had received postdoctoral training in research ethics. This suggests the situation in terms of research ethics education in the country requires important attention. Third, further work is needed to establish internal reliability within the subscales in the TREK-P. Given the brevity of the TREK-P and the need for efficiency, its questions cover some domains, but not all relevant areas. Furthermore, the TREK-P does not measure attitudes, skills, or behaviors. Fourth, the fellowship group consisted of medical professionals who applied and were selected for an NIH program and represented a special group. Thus, their better performance on the TREK-P may not necessarily reflect the impact of training experience alone, but also an interest in the field. However, such a possibility highlights an important need to build not only on training but also opportunities to enhance interest and motivation in the burgeoning field of research ethics that serves as an important foundation of research career development in Azerbaijan.
Conclusions
Our study revealed deficits in knowledge about different aspects of pediatric-oriented research ethical principles. Previous research showed evidence of errors in physicians’ judgment related to areas such as informed consent, end-of-life care, and the provision of information to patients regarding certain morally difficult medical procedures. 12 Our results support the importance of the inclusion of structured formal training on ethical principles during and after residency. We showed that professionals who participated in such training programs have a deeper understanding of the subject. A promising aspect of the results involving the medical students was that they showed performance comparable to the United States students in the original study and further training can be built in the future upon it. There is a need for tools used to measure knowledge of ethics in LMIC settings, with acknowledgment of the need for a balance between universally accepted ethical values and local cultural and legal aspects of practice.
Supplemental Material
sj-doc-1-gph-10.1177_2333794X231224989 – Supplemental material for Assessment of Research Ethics Knowledge of Pediatricians
Supplemental material, sj-doc-1-gph-10.1177_2333794X231224989 for Assessment of Research Ethics Knowledge of Pediatricians by Kamran Salayev, Ulviyya Aslanova, Narmin Guliyeva, Geray Geraybeyli and Kerim Munir in Global Pediatric Health
Footnotes
Author Contributions
KS: Contributed to conception and design; Contributed to analysis; Drafted the manuscript; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. UA: Contributed to conception and design; Contributed to analysis; Drafted the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. NG: Contributed to analysis; Drafted the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. GG: Contributed to conception and design; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy. KM: Contributed to conception and design; Contributed to analysis; Drafted the manuscript; critically revised the manuscript; Gave final approval; Agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research education component of this work was supported by a FIC/NIH D43 TW011237 grant at Boston Children’s Hospital, USA.
Ethical Approval and Consent to Participate
All methods were carried out in accordance with relevant guidelines and regulations. The study was approved by the Ethical Committee of the Azerbaijan Psychiatric Association with Boston Children’s Hospital Institutional Review Board compliance. Written informed consent was obtained from all the respondents. Data were presented in such a way that no individual can be identified.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.